
Abstract
Pancreatic ductal adenocarcinoma is a lethal disease with an overall 5-year survival of less than 5%. Prognosis among surgically treated patients is difficult and identification of new biomarkers is essential for accurate prediction of patient outcome. As part of one of the major cellular protein degradation systems, the proteasome plays a fundamental role in both physiological and pathophysiological conditions including cancer. The proteasome-associated deubiquitinating enzyme ubiquitin C-terminal hydrolase L5 (UCHL5)/Uch37 is a modulator of proteasome activity with cancer prognostic marker potential. Cytoplasmic and nuclear immunoexpression of UCHL5 was evaluated in 154 surgical specimens from pancreatic ductal adenocarcinoma patients treated at Helsinki University Hospital, Finland, in 2000–2011. UCHL5 expression in relation to clinicopathological parameters and the association between UCHL5 In this study, positive expression and patient survival were assessed. Positive nuclear UCHL5 expression was associated with increased patient survival (p = 0.005). A survival benefit was also detectable in these subgroups of patients: over 65 years (p < 0.001), at tumor stages IIB to III (p = 0.007), or with lymph-node positivity (p = 0.006). In stages IIB to III disease, patients with positive nuclear UCHL5 expression showed a twofold increase in 5-year cancer-specific survival compared to those with negative expression. Multivariate analysis identified positive nuclear UCHL5 expression as an independent prognostic factor (p = 0.012). In conclusion, UCHL5 expression could function as a prognostic marker in pancreatic ductal adenocarcinoma, particularly at disease stages IIB to III. As UCHL5 is one of the few markers predicting increased survival, our results may be of clinical relevance.
Keywords
Introduction
Pancreatic ductal adenocarcinoma (PDAC) patients have poor prognosis, with an overall 5-year survival under 5%. In the United States, PDAC causes over 40,000 deaths each year, constituting the fourth leading cause of cancer-related mortality. 1 Finland has about 1000 new cases annually, with PDAC as the third leading cause of cancer-related death (Finnish Cancer Registry; www.cancerregistry.fi). Over the last few decades, overall disease outcome has not improved significantly, despite advances in treatment. 1 At diagnosis, only 10% of patients have localized disease, and 25% have regional disease. Radical surgical resection combined with oncological therapy serves as curative treatments, but is possible for only about 20% of the patients. 2 Despite recent progress in assessment of PDAC biomarkers,3–5 no biomarker is yet recommended for clinical praxis. Hence, identification of new markers is essential to more accurately predict PDAC patient outcome and to improve understanding of the molecular mechanisms involved.
Of late, the search for novel cancer markers and treatment targets has created growing interest in modulators of the ubiquitin-proteasome system (UPS). UPS is an essential cellular pathway for controlled proteolysis, by which protein substrates are targeted for degradation by the proteasome after their polyubiquitination via a cascade of E1, E2, and E3 enzymes. 6 Prior to degradation, the attached polyubiquitin chains are removed by deubiquitinating enzymes (DUBs). Overall, the human genome contains approximately 80 known DUBs, around 40 of which have been associated with various types of cancer.7,8 Among them is ubiquitin C-terminal hydrolase L5 (UCHL5)/Uch37, a cysteine protease from the family of ubiquitin C-terminal hydrolases (UCHs), one of the three proteasome-associated DUBs. UCHL5 interacts with the 26S-proteasome subunit Admr1/Rpn13 in a reversible 9 and evolutionarily conserved manner, 10 inducing its DUB activity. UCHL5 also binds to the NFRKB subunit of the INO80 chromatin remodeling complex, rendering it DUB inactive, but the physiological role of this interaction is unclear.11,12 UCHL5 knockout mice display embryonic lethality, 13 demonstrating the essential function of this DUB. In Caenorhabditis elegans, the UCHL5 homolog UBH-4 regulates proteasome activity in a tissue-specific manner, as well as affecting both health and lifespan. 9
In human tissues, UCHL5 expression level and subcellular location vary in both cancer and healthy tissues. 14 High UHCL5 expression has been reported to correlate with poor survival and increased cancer recurrence in esophageal squamous cell carcinoma, hepatocellular carcinoma, and epithelial ovarian cancer.15–17 In contrast to these results, we have, in another study, demonstrated that in lymph node–positive rectal cancer (Dukes C/stage III), strong UCHL5 positivity as well as lack of UCHL5 expression is linked to markedly increased patient survival 18 . The aim of this study is to evaluate UCHL5 tumor tissue expression and its connection to survival in PDAC patients, estimating UCHL5’s potential as a prognostic marker for the disease.
Materials and methods
Patients
Between 2000 and 2011, 188 PDAC patients underwent surgery at the Department of Surgery, Helsinki University Hospital, Finland. In total, 34 patients were excluded from the cohort: 22 who received neoadjuvant chemotherapy, 8 with stage IV disease, 19 and 4 lacking data on stage. Only PDAC, but no other variants of exocrine pancreatic cancer, was included in the study. Median age at surgery was 64 (range: 39–83) years. Median follow-up was 2.0 (range: 0.2–13.1) years. Clinical data came from patient records, survival data from the Finnish Population Registry, and cause of death for those deceased from Statistics Finland.20–22
Preparation of tumor tissue microarrays and immunohistochemistry
Formalin-fixed and paraffin-embedded surgical tissue samples came from the archives of the Department of Pathology, Helsinki University Hospital. All samples were re-evaluated by an experienced pathologist for confirmation of the histopathological diagnosis of PDAC. Representative areas of tumor specimens were defined and marked on hematoxylin and eosin–stained slides for preparation of tissue microarray (TMA) blocks. Six 1.0-mm cores were taken from each tumor block with a semiautomatic tissue microarrayer (Tissue Arrayer 1; Beecher Instruments Inc., Silver Spring, MD, USA).
TMA blocks were newly cut into 4-µm sections. The slides were deparaffinized in xylene and rehydrated through a gradually decreasing concentration of ethanol to distilled water, followed by treatment in a PreTreatment module (Lab Vision Corp., Fremont, CA, USA) in Tris-HCl (pH 8.5) buffer for 20 min at 98°C for antigen retrieval. Staining of sections was performed in an Autostainer 480 (Lab Vision Corp.) by the Dako REAL EnVision Detection system, Peroxidase/DAB+, Rabbit/Mouse (Dako, Glostrup, Denmark). Tissues were incubated with rabbit polyclonal anti-UCHL5 antibody (HPA005908; diluted to 1:800 = 8 µg/mL; Sigma Aldrich, Missouri, USA) for 1 h at room temperature. A subset of samples (approximately 120) was validated with an additional anti-UCHL5 antibody (mouse monoclonal UCHL5 antibody, sc-271002; diluted to 1:500; Santa Cruz, TX, USA) with similar results on UCHL5 expression levels and pattern (data not shown).
Evaluation of stainings
Cytoplasmic and nuclear staining of UCHL5 was scored separately. Cytoplasmic staining was scored according to staining intensity as negative (0), low positive (1), moderate positive (2), or high positive (3). Nuclear staining was scored according to the proportion of positive nuclei in the tumor tissue: 0%–10% positive nuclei scored as 0, 11%–40% as 1, 41%–75% as 2, and 76%–100% as 3. Stainings were evaluated independently by two investigators (L.A. and J.H.) without knowledge of clinical data or outcome. Discrepancies in scoring were discussed until consensus. Representative staining intensities were imaged at random, and image brightness was adjusted similarly by Adobe Photoshop version CS6 (64 bit).
Statistical analysis
For statistical purposes, UCHL5 expression was dichotomized. UCHL5 cytoplasmic expression was divided into low (scores: 0–1) and high (scores: 2–3) expression and nuclear expression into negative (<10% nuclear positivity, score: 0) and positive (>10%, scores: 1–3) staining. The median score of each patient served in further analysis because expression in pancreatic tumor tissue may vary greatly. To evaluate associations between tumor-marker expression and clinicopathological variables, Fisher’s exact test and the linear-by-linear association test were conducted. Survival analysis was done with the Kaplan–Meier method, and the Breslow test was the choice for comparing groups. The Cox regression proportional hazard model served for uni- and multivariate survival analysis adjusted for age, gender, stage, metastasized lymph node ratio (LNR) ≥/<20% (cutoff: ≥/<20%), and postoperative adjuvant therapy. Since stage and LNR are internally correlated, a combination variable was made for multivariate analyses. Interaction terms were considered. The Cox model assumption of constant hazard ratios over time was tested. A time-dependent covariate was included separately for each testable variable at a time. All variables fulfilled the assumption. A p value < 0.05 was considered significant, and all tests were two-sided. Statistical analyses were carried out with SPSS version 24.0 (IBM SPSS Statistics, version 24.0 for Mac; SPSS, Inc., Chicago, IL, USA, an IBM Company).
Results
Immunohistochemical staining
Cytoplasmic and nuclear UCHL5 expression was evaluable in the tumor tissue of 153 (99.4%) specimens. The cytoplasmic immunoexpression was negative in 94 (61.4%), low in 51 (33.3%), moderate in seven (4.6%), and strongly positive in one (0.7%) specimen (Figure 1(a)–(d)). When cytoplasmic UCHL5 expression was observed, the staining was uniform in intensity and prevalent throughout the whole tumor tissue. Nuclear expression was evaluated according to the proportion of positive nuclei in the tumor tissue as 0 in 74 (48.4%), as 1 in 50 (32.7%), as 2 in 20 (13.1%), and as 3 in nine (5.9%) tumor specimens (Figure 1(e)). One patient with strong cytoplasmic UCHL5 expression scored 3 in nuclear expression, whereas seven patients with moderate cytoplasmic UCHL5 expression scored predominantly 0 or 1. No statistical correlation between nuclear and cytoplasmic UCHL5 staining was found (p = 0.117, data not shown). Normal-appearing cells adjacent to the tumor tissue displayed predominantly low or negative cytoplasmic staining and low percentage of nuclear positive staining (Figure 1(f)). The staining pattern and intensity of UCHL5 expression were validated with one additional anti-UCHL5 antibody displaying a similar staining pattern (data not shown).

Immunohistochemical staining pattern of UCHL5 in PDAC and in normal pancreas. (a) Negative cytoplasmic UCHL5 expression. (b) Low cytoplasmic expression. (c) Moderate cytoplasmic expression. (d) Strong cytoplasmic expression. (e) Positive nuclear UCHL5 expression (e.g. white arrows). (f) UCHL5 staining pattern in normal-appearing pancreatic tissue adjacent to tumor tissue. Original magnification ×400.
Association of UCHL5 expression with clinicopathological parameters
Nuclear UCHL5 expression showed a significant association with T stage, and patients with positive nuclear UCHL5 expression had smaller tumors than did those with negative nuclear expression (p = 0.018; Table 1). Patients with positive nuclear UCHL5 expression were significantly older (≥65 years) than patients with negative nuclear expression (p = 0.004; Table 1). Nuclear UCHL5 expression showed no association with gender, stage, histological grade, metastasized LNR, perineural or with perivascular invasion (Table 1). No significant association existed between cytoplasmic UCHL5 expression and any of the clinicopathological parameters assessed (Supplementary Table 1). The intensity of cytoplasmic UCHL5 expression and the amount of nuclear UCHL5 expression showed no correlation (p = 0.117; Spearman correlation).
Association of UCHL5 nuclear expression and clinicopathological parameters.
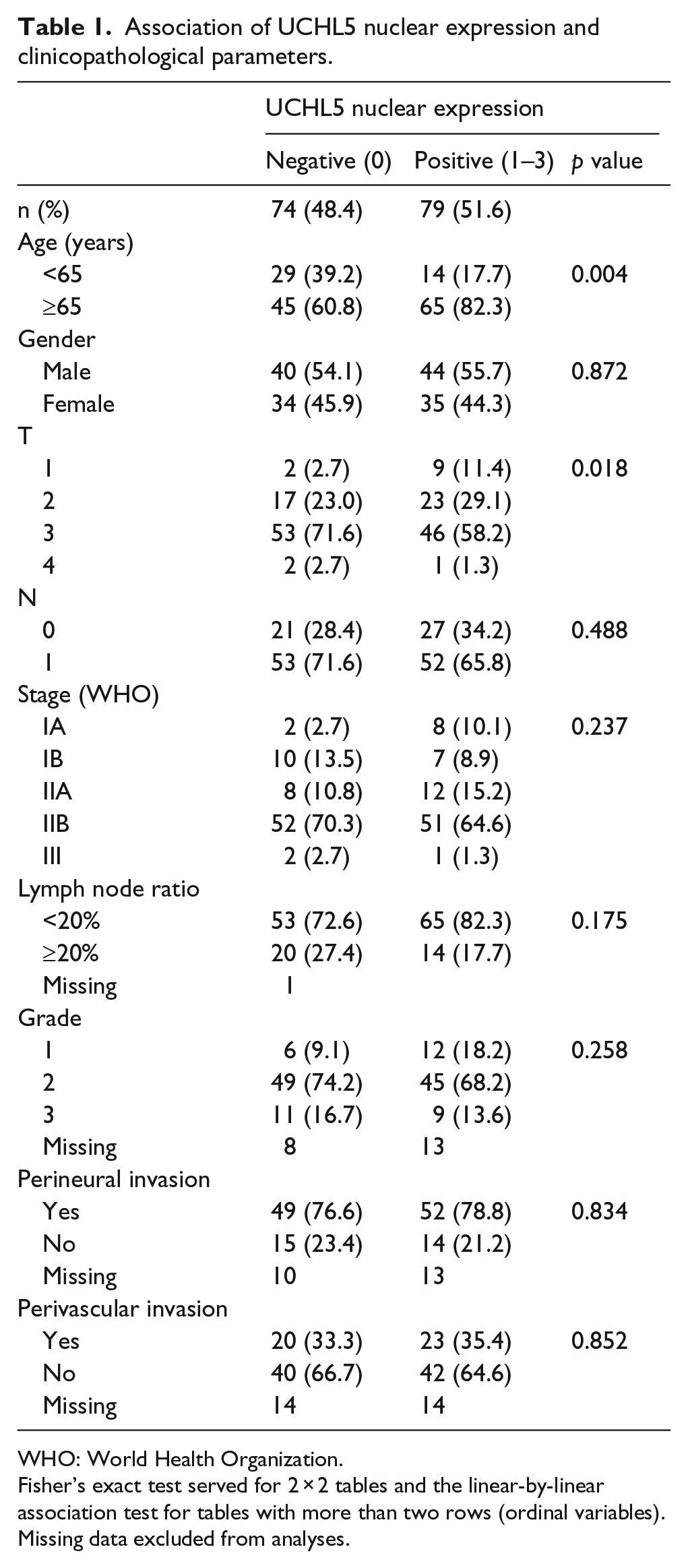
WHO: World Health Organization.
Fisher’s exact test served for 2 × 2 tables and the linear-by-linear association test for tables with more than two rows (ordinal variables). Missing data excluded from analyses.
Survival analysis
The 5-year cancer-specific survival (CSS) was significantly better for PDAC patients with either high cytoplasmic UCHL5 expression (p = 0.034; Figure 2) or positive nuclear UCHL5 expression (p = 0.005; Figure 2). The 5-year CSS for patients with high cytoplasmic expression was 57.1% (95% confidence interval (CI): 17.2%–83.7%, Table 2) and for patients with low cytoplasmic expression, 18.1% (95% CI: 12.2%–24.9%, Table 2). Correspondingly, 5-year CSS for patients with positive nuclear expression was 22.1% (13.5%–32.1%, Table 2) and for those with negative expression, 17.4% (95% CI: 9.7%–27.0%, Table 2).
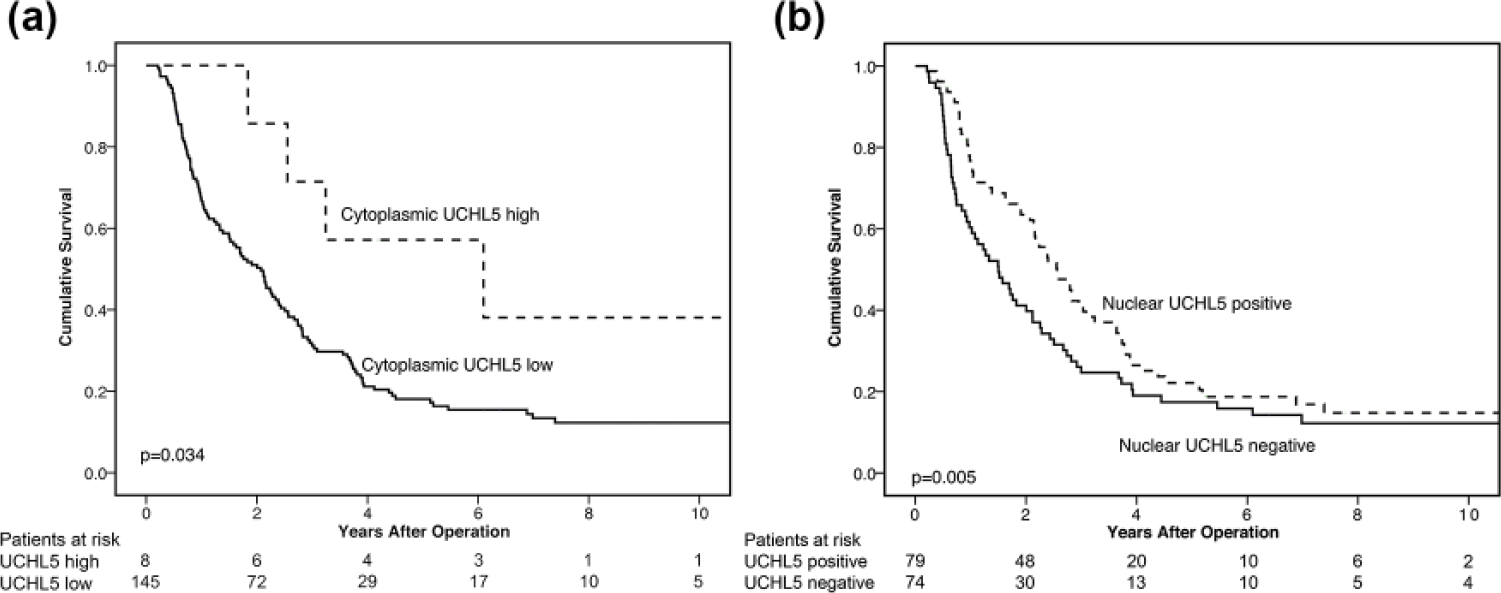
Positive nuclear UCHL5 expression as a marker for better prognosis in PDAC. Cancer-specific survival according to the Kaplan–Meier test for (a) cytoplasmic and (b) nuclear UCHL5 expression in patients with PDAC.
CSS of PDAC by cytoplasmic and nuclear UCHL5 expression.

CSS: cancer-specific survival; CI: confidence interval; PDAC: pancreatic ductal adenocarcinoma.
When classified by tumor stage, the beneficial survival trend associated with nuclear UCHL5 expression became more explicit. In patients with stage IA–IIA disease, no difference appeared in survival between those with UCHL5 nuclear-positive and nuclear-negative tumors (data not shown). The 5-year CSS in stage IIB–III patients with positive nuclear expression was 19.9% (95% CI: 10.2%–31.9%, Table 2), compared to patients with negative expression who had 10.4% (95% CI: 3.8%–20.8%, Table 2, p = 0.007; Figure 3(a)). The 5-year CSS for patients over 65 years and positive nuclear UCHL5 expression was 19.1% (95% CI: 10.3%–29.8%) compared to 13.3% (95% CI: 5.2%–25.1%) for patients with negative expression (p < 0.001, Table 2, Figure 3(b)). Furthermore, in this subgroup of patients over 65 years, those with stage IIB–III disease and positive nuclear UCHL5 expression had a 5-year CSS of 15.4% (95% CI: 6.3%–28.4%) and those with negative expression 8.1% (95% CI: 1.7%–21.3%, Table 2, p = 0.002; Figure 3(c)). Additionally, a significant survival difference was also detectable in lymph node–positive patients (p = 0.006, Table 2, Figure 3(d)). The 5-year CSS for patients with lymph node positivity and positive nuclear UCHL5 expression was 19.9% (95% CI: 10.2%–31.9%) compared to 10.6% (95% CI: 3.9%–21.2%) for patients with lymph node positivity and negative expression (Table 2). Both 2-year and 5-year CSS showed similar survival trends (Table 2).

Positive nuclear UCHL5 expression corresponds to better prognosis in subgroups of patients with PDAC. Cancer-specific survival analysis according to the Kaplan–Meier test. (a) Nuclear UCHL5 expression in patients with regional disease (stages IIB–III). (b) Nuclear UCHL5 expression in patients over 65 years. (c) Nuclear UCHL5 expression in patients over 65 years and with regional disease (stages IIB–III). (d) Nuclear UCHL5 expression in patients with lymph node–positive PDAC.
In univariate analysis, neither cytoplasmic nor nuclear UCHL5 expression associated significantly with risk of death from PDAC (hazard ratio (HR) = 0.38, 95% CI: 0.14–1.04, p = 0.060 and HR = 0.71, 95% CI: 0.50–1.01, p = 0.056, respectively, Supplementary Table 2). In multivariate analysis adjusted for age, gender, stage, LNR, and postoperative adjuvant chemotherapy, cytoplasmic UCHL5 expression did not significantly predict survival (HR = 0.47, 95% CI: 0.17–1.29, p = 0.144, Table 3). Similarly adjusted multivariate analysis, however, demonstrated that positive nuclear UCHL5 expression was linked to significantly better patient survival (HR = 0.63, 95% CI: 0.44–0.90, p = 0.012, Table 3).
Cox multivariate analysis of relative risk of death from PDAC by UCHL5 expression.

CI: confidence interval; HR: hazard ratio; PDAC: pancreatic ductal adenocarcinoma; LNR: lymph node ratio.
Multivariate analysis included adjustment for age, gender, stage (IA–IIA, IB, and III), lymph node ratio (≥/<20%), and postoperative adjuvant therapy.
Discussion
Here, we show that positive nuclear UCHL5 expression, and potentially also high cytoplasmic UCHL5, expression is a predictive factor of better prognosis in PDAC patients. For patients with positive nuclear UCHL5 expression, marked differences in survival were identified in the subgroups of patients over 65 years, with regional disease (stages IIB–III) and with lymph node–positive disease. To our knowledge, our study is the first to report on UCHL5 tissue expression in a cohort of PDAC patients.
According to the Human Protein Atlas, 14 moderate to low staining of UCHL5 is detectable in pancreatic cancer samples. To date, only a few publications on UCHL5 involve analysis by immunohistochemistry in cancer. Chen et al. 15 showed that higher overall UCHL5 expression, without division into cytoplasmic and nuclear localization, associated in esophageal squamous cell carcinoma with decreased survival, but it was not an independent prognostic factor. In hepatocellular carcinoma, UCHL5 expression has been called an independent prognostic factor for recurrence but not for overall survival. 16 In epithelial ovarian cancer, immunopositive cytoplasmic UCHL5 expression was reportedly an independent factor for poor prognosis. 17 In contrast to these findings, we show here that both UCHL5 nuclear positivity and potentially also high cytoplasmic expression are associated with increased survival. In support of the survival benefit of UCHL5, we have shown in another study that high as well as negative cytoplasmic UCHL5 immunoreactivity correlates with increased survival in lymph node–positive (Dukes C/stage III) rectal cancer 18 . Interestingly, in colorectal cancer, positive nuclear UCHL5 immunoexpression was rare and therefore not scored separately 18 . In our study, high cytoplasmic UCHL5 expression appears to support survival, but it is hard to draw strong conclusions regarding the significance of cytoplasmic immunostaining in PDAC prognosis due to the small number of patients (four patients alive at 5 years after surgery). It will be important to corroborate the survival benefit linked to high cytosolic UCHL5 expression in another PDAC patient cohort.
UCHL5 interacts with the proteasome and functions as a negative regulator of proteasome activity in both human cell lines and C. elegans.9,11,23 A high level of nuclear UCHL5 may lead to excessive inhibition of the proteasome, and, over time, to increased accumulation and aggregation of proteasomal substrates detrimental to the cell. As inactive UCHL5 can also be a part of the INO80 chromatin remodeling complex,11,12 abnormally high nuclear UCHL5 expression in tumor tissues may affect the function of this complex in cell survival. Identifying molecular mechanisms by which UCHL5 operates both in cancer and normal healthy tissues calls for vigorous effort. It is intriguing that high UCHL5 expression correlates with better prognosis, especially in more severe stages in both rectal cancer (Dukes C/stage III 18 and PDAC (stage IIB–III). PDAC patients with positive nuclear UCHL5 expression tended to be older, with tumors of smaller size. Decline in proteostasis is one of the hallmarks of aging, 24 and dysfunction of the proteasome has appeared in various in vitro systems in aging-related disorders. Thus, one could speculate that high UCHL5 expression further reduces proteasome activity in the elderly, thereby perhaps rendering tumor cells more susceptible to apoptosis.
We have demonstrated earlier that high expression of β-catenin associates with a better prognosis in PDAC. 20 As the expression level of β-catenin is directly regulated by proteasomal degradation, 25 the UCHL5-mediated decrease in proteasome activity may elevate β-catenin levels. Additionally, PDAC is characterized by considerable desmoplastic reaction, involving stromal cells and the extracellular matrix (ECM). 26 The stromal cells, referred to as pancreatic stellate cells (PSCs), are responsible for the reaction and are capable of proliferating and producing ECM and tumor-promoting growth factors. 27 The PSCs are involved in PDAC progression. 28 Recently, Smad7 and transforming growth factor beta (TGF-β) signaling were reported to be affecting PSC-induced carcinoma-cell migration. 29 Because UCHL5 has links to Smads and to TGFβ signaling,30–33 it may play a role also in the desmoplastic reaction. This hypothesis, however, needs further investigation.
About a decade ago, the proteasome inhibitor bortezomib was approved for treatment of multiple myeloma34,35 and mantle cell lymphoma. 36 Proteasome inhibitors are potent therapeutics, but with a limited therapeutic window and often dose-dependent toxicity, as well as considerable drug resistance, especially upon cancer recurrence. 37 Interest is growing in alternative therapeutic targets in cancer that modulate the UPS, including DUBs.38,39 Dual pharmacological inhibition of the proteasome-associated DUBs, Usp-14 and UCHL5, has been shown to promote cytotoxicity in cancer cells and inhibited tumor growth7,38,40 and to extend survival in xenograft models of multiple myeloma. 41 Thus, targeting proteasome-associated DUB activity may provide an attractive strategy to combat drug resistance associated with conventional proteasome inhibitors.
The overall prognosis in PDAC is poor, and it would be important to be able to predict the course of the disease as precisely as possible. PDAC is a genetically heterogeneous cancer, with several key mutated genes. 42 Many researches have contributed to progress in the assessment of new biomarkers in PDAC.3,4,5 However, there is still a distinct lack of feasible prognostic markers in clinical praxis. We have recently demonstrated that PODXL, PROX1, and β-catenin function as promising immunohistochemical prognostic markers in PDAC.20,21 In this study, we show significant survival differences in PDAC patients depending on nuclear UCHL5 expression level of the tumor, and our results may provide future clinical relevance.
Unfortunately, due to the long period (approximately 10 years) needed for data collecting, some essential clinicopathological parameters were unavailable. The TMA technique enables analysis of large patient cohorts with relative ease and accuracy. Less than 1% of specimens were lost for technical reasons. Compared to whole-tissue sections, much smaller areas of tumors are actually evaluated, but this potential sampling error is reduced by taking core samples from various parts of the tumor. The strength of this study is therefore a quite large patient cohort with a long follow-up period.
In conclusion, we demonstrate that UCHL5 is a novel prognostic biomarker in PDAC, and that positive nuclear UCHL5 expression correlates with better prognosis. Validation of our findings in other patient cohorts is imperative, but UCHL5 may prove to have prognostic significance in other cancer forms as well.
Footnotes
Acknowledgements
The authors thank Päivi Peltokangas and Olli-Matti Sirviö for technical assistance and Stig Nordling for histopathological evaluation. L.A. and K.S. shared the first authorship. H.S., C.H., and C.I.H. equal last authorship. C.H. and C.I.H worked in experimental design and conception. H.S. and K.S worked in clinical data collection. L.A. and J.H. worked in experimentation, L.A., K.S., and H.M. in data analysis, C.H and C.I.H in reagent/material/analysis tool contribution. L.A., K.S., H.M., H.S., C.H., and C.I.H. worked in writing of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted according to the World Medical Association Declaration of Helsinki. It was approved by the Surgical Ethics Committee of Helsinki University Hospital (Dnro HUS 226/E6/06, extension TMK02 §66, 17 April 2013) and the National Supervisory Authority of Welfare and Health (Valvira Dnro 10041/06.01.03.01/2012). Written informed consent was acquired from the participants for their clinical records to be used in this study.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants to C.I.H. from the Academy of Finland (259797, 297776), Medicinska Understödsföreningen Liv och Hälsa r.f., and the Ruth and Nils-Erik Stenbäck Foundation, to C.H. from the Sigrid Jusélius Foundation and the Cancer Society of Finland, and to H.S. from the Mary and Georg C Ehrnrooth Foundation, the Sigrid Jusélius Foundation, and the Helsinki University Hospital Research Fund. L.A. was supported by the Doctoral Programme in Biomedicine, University of Helsinki and by grants from the Victoria Foundation and the K. Albin Johansson Foundation. K.S. was supported by grants from the K. Albin Johansson Foundation and from the Ida Montin Foundation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.