
Abstract
The RARβ and FHIT promoter methylation are observed in some cervical carcinoma. However, the association between RARβ and FHIT promoter methylation and cervical carcinogenesis remains unclear. This study was carried out to evaluate the correlation between RARβ or FHIT promoter methylation and cervical carcinogenesis. Eligible publications were searched via online databases. The combined odds ratios and corresponding 95% confidence intervals were calculated and summarized. In all, 17 eligible articles on RARβ and FHIT promoter methylation were identified in the study. RARβ promoter methylation was significantly higher in cervical cancer than in cervical intraepithelial neoplasia lesions and normal cervical tissues (odds ratio = 3.90, p = 0.018; odds ratio = 12.98, p < 0.001, respectively). There was more FHIT promoter methylation in cervical cancer than in cervical intraepithelial neoplasia lesions and normal controls (odds ratio = 8.0, p = 0.055; odds ratio = 10.75, p < 0.001, respectively). In addition, FHIT promoter methylation was correlated with clinical stage (advanced stage vs early stage: odds ratio = 2.69, p = 0.056) and tumor grade (high grade vs low grade: odds ratio = 4.11, p < 0.001). RARβ and FHIT promoter methylation may be associated with the carcinogenesis of cervical cancer. FHIT promoter methylation may play a crucial role in cervical cancer progression. Additional studies with large sample sizes are essential to confirm our findings.
Introduction
Cervical cancer is the most common gynecologic malignancy and the leading cause of gynecologic cancer-related deaths worldwide. 1 Based on global cancer statistics, approximately 527,600 new cases were clinically diagnosed as cervical carcinoma in 2012, leading to an estimate of about 265,700 deaths. 1 Cervical cancer comprised three main histotypes: squamous cell carcinoma (SCC), adenocarcinoma (AC), and adenosquamous carcinoma. The SCC accounts for 85%–90% of cervical cancer patients. 2 The cervical cancer survival varies greatly by tumor stage. Due to lymph node and distant metastases,3,4 advanced-stage patients are remarkably incurable with the poor 5-year survival of 17%, compared with early stages that have a good survival rate. 5
Studies have shown that epigenetic modifications are significantly linked to cancer.6,7 DNA methylation, a major mechanism of epigenetic alterations, plays a crucial role in carcinogenesis and cancer progression.8–10 Aberrant promoter methylation of tumor suppressor genes (TSGs), such as death-associated protein kinase 1 (DAPK1) gene, was reported to be involved in the pathogenesis of cervical cancer. 11 The retinoic acid receptor beta (RARβ) gene, a TSG located at human chromosome 3p24, is a member of the RAR receptor family that encodes RARβ protein.12,13 Loss of RARβ expression through promoter methylation within CpG islands was demonstrated to be involved in carcinogenesis.12,14 The fragile histidine triad (FHIT) gene, another TSG mapped to chromosome 3p14.2, belongs to the histidine triad gene family. 15 FHIT has a variety of biological functions such as the regulation of apoptotic cell death and inhibition of cell proliferation.16,17 The promoter of RARβ and FHIT has been reported to be methylated in cervical cancer.18,19
Kang et al. 19 reported that no significant correlation was observed between FHIT promoter methylation and cervical cancer risk. On the contrary, Bai et al. 20 found that FHIT promoter methylation was significantly correlated with cervical cancer risk. However, similar frequency of RARβ promoter methylation was observed in cervical cancer and cervical intraepithelial neoplasia (CIN) lesions by Sun et al. 21 However, according to Feng et al., 22 RARβ promoter methylation was significantly higher in cervical cancer than in CIN lesions. Therefore, eligible studies were collected to investigate the correlation between RARβ and FHIT promoter methylation and cervical carcinogenesis. In addition, whether FHIT promoter methylation was associated with the grade and stage of cervical cancer was also analyzed.
Materials and methods
Search strategy
An exhaustive search of online electronic databases was conducted in the PubMed, Embase, EBSCO, and Cochrane Library for eligible articles published before 11 December 2016. The relevant databases were searched using the following key words and free terms: “uterine cervix or cervical,” “cancer or carcinoma or tumor or neoplasm,” “FHIT or Fragile histidine triad,” “RARβ or RAR-beta or RARB or retinoic acid receptor-β,” and “methylation or hypermethylation or promoter methylation or epigenetic silencing or epigenetic inactivation.”
Selection of the eligible studies
The following selection criteria of eligibility were applied for the included studies: (1) patients with cervical cancer were diagnosed by histopathological examination; (2) studies provided complete information about the frequency of the FHIT or RARβ promoter methylation in cervical cancer, CIN lesions, and normal control samples, to assess the relationship between methylation and cervical cancer; (3) the correlation between FHIT or RARβ promoter methylation and clinicopathological features (and prognostic parameters if possible) was analyzed in cervical cancer patients; and (4) only studies published in English were included in this meta-analysis. The most recent publication with larger population was selected if the author published more than one paper using the same sample data.
Data extraction
Two authors independently abstracted the following information based on a standard form: last name of the first author, publication year, country, ethnic population, sample type, case number (cancer, CIN lesions, and normal samples), detection method, methylation frequency, clinicopathological parameters (tumor grade, clinical stage, and pathological subtype), and the prognosis. Disagreements on the data were resolved by all authors.
Statistical analysis
This study was conducted using the Stata software (version 12.0; Stata Corporation, College Station, TX, USA). The overall odds ratios (ORs) and corresponding 95% confidence intervals (95% CIs) were calculated to evaluate the relationship between FHIT or RARβ promoter methylation and cervical carcinogenesis in the samples from cervical cancer, CIN lesions, and normal controls. For studies with adequate information, the association of FHIT or RARβ promoter methylation with clinicopathological characteristics of cervical cancer patients was also analyzed in this meta-analysis. Heterogeneity of effect sizes among studies was estimated using the Cochran’s Q test and I2 statistic. 23 The random-effects model was applied in this study. For the results calculated from the data presented in more than nine studies, there was obvious evidence of heterogeneity (I2 > 50% or p < 0.1). Sensitivity analyses were carried out by omitting each study at a time to determine its influence on the pooled ORs.24,25 Moreover, subgroup analyses were performed to detect potential sources of heterogeneity.
Results
Study selection and characteristics
Figure 1 shows the initial search strategy, resulting in a total of 209 potential publications. According to the above-described inclusion criteria, 17 eligible articles 18–22,26–37 were finally collected in this meta-analysis. Of the eligible studies, 10 studies analyzed the correlation between RARβ promoter methylation and cervical carcinogenesis,18,21,22,27,29,31,32,34,36,37 including 477 patients with cervical cancer, 577 patients with CIN lesions, and 124 normal controls. The relationship between FHIT promoter methylation and cervical carcinogenesis was examined among 10 studies,19,20,26–28,30,32,33,35,37 including 643 patients with cervical cancer, 177 patients with CIN lesions, and 324 normal controls. The baseline characteristics of the included studies were listed in Table 1.

Flow diagram of the study selection.
The main characteristics of the included studies in this meta-analysis.
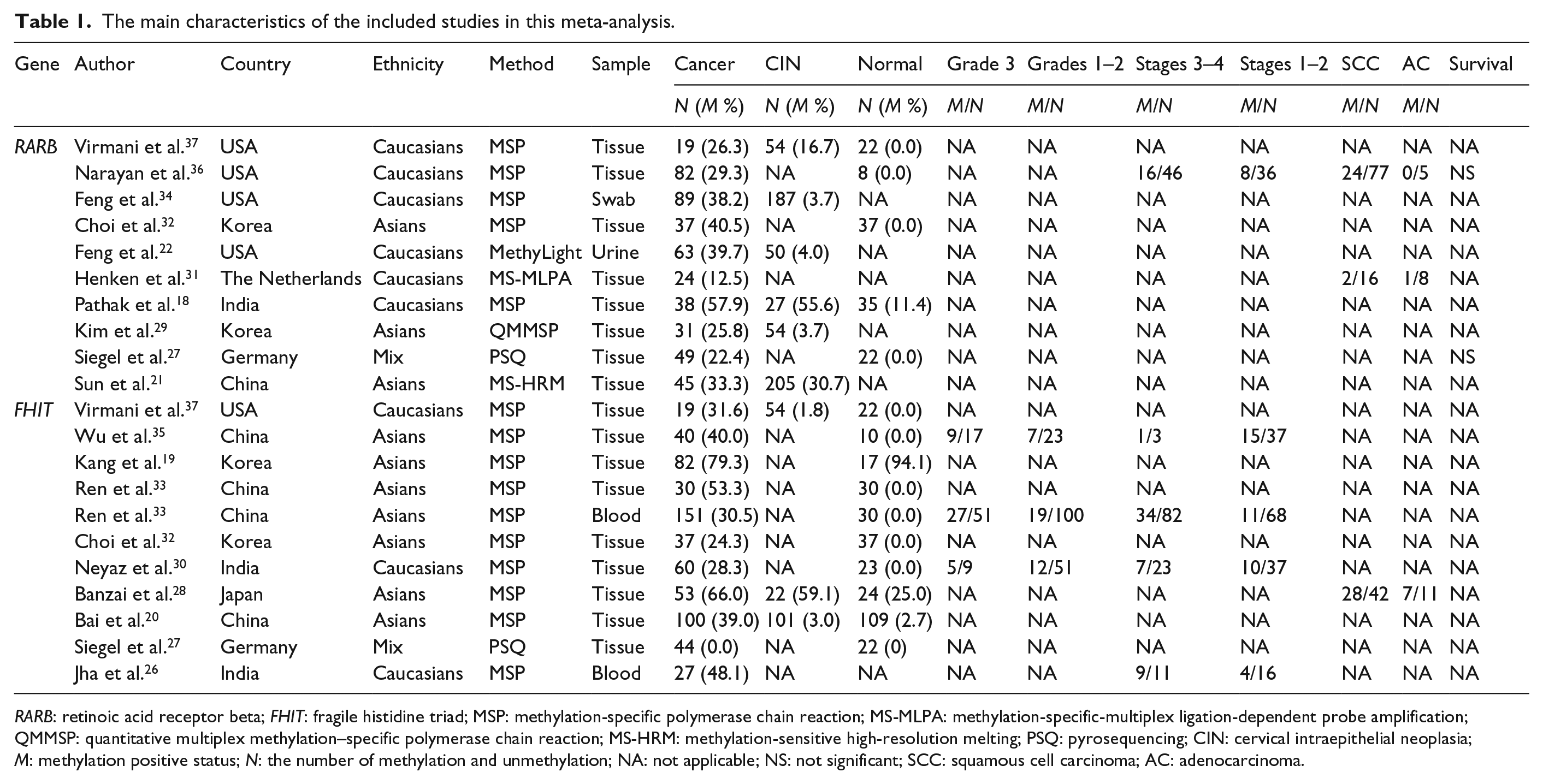
RARB: retinoic acid receptor beta; FHIT: fragile histidine triad; MSP: methylation-specific polymerase chain reaction; MS-MLPA: methylation-specific-multiplex ligation-dependent probe amplification; QMMSP: quantitative multiplex methylation–specific polymerase chain reaction; MS-HRM: methylation-sensitive high-resolution melting; PSQ: pyrosequencing; CIN: cervical intraepithelial neoplasia; M: methylation positive status; N: the number of methylation and unmethylation; NA: not applicable; NS: not significant; SCC: squamous cell carcinoma; AC: adenocarcinoma.
RARβ promoter methylation and cervical cancer risk
The results of the correlation between RARβ promoter methylation and cervical cancer risk included two comparisons: (1) 285 cervical cancer patients compared to 577 CIN lesions and (2) 225 cervical cancer patients compared to 124 normal controls (Figure 2). RARβ promoter methylation was shown to be significantly higher in cervical cancer than in CIN lesions and normal cervical tissues (OR = 3.90, 95% CI = 1.27–12.02, p = 0.018; OR = 12.98, 95% CI = 5.09–33.08, p < 0.001, respectively).

Forest plot of the association between RARβ promoter methylation and cervical cancer risk from the comparison between cervical cancer, cervical intraepithelial neoplasia (CIN) lesions, and normal controls.
Subgroup analysis of RARβ promoter methylation and cancer risk (cancer vs CIN)
According to the subgroup analysis by testing method (methylation-specific polymerase chain reaction (PCR; MSP) and non-MSP), RARβ promoter methylation was not associated with cervical cancer in MSP or non-MSP subgroups (OR = 3.23, 95% CI = 0.55–18.94, p = 0.194; OR = 4.93, 95% CI = 0.74–32.64, p = 0.098, respectively; Figure 3).

Subgroup analysis of RARβ promoter methylation by detection methods based on the comparison between cervical cancer and cervical intraepithelial neoplasia (CIN).
FHIT promoter methylation and cervical cancer risk
The result from the comparison between 172 cervical cancer and 177 CIN lesions indicated that the frequency of FHIT promoter methylation was significantly higher in cervical cancer than in CIN lesions (OR = 8.0, 95% CI = 0.95–66.96, p = 0.055; Figure 4). With respect to the comparison between 616 cervical cancer and 324 normal controls, the result demonstrated that there was more FHIT promoter methylation in cervical cancer than in normal controls (OR = 10.75, 95% CI = 3.65–31.62, p < 0.001).

Forest plot of the association between FHIT promoter methylation and cervical cancer risk from the comparison between cervical cancer, cervical intraepithelial neoplasia (CIN) lesions, and normal controls.
Subgroup analysis of FHIT promoter methylation and cancer risk (cancer vs normal controls)
Subgroup analysis by ethnicity demonstrated that FHIT promoter methylation was significantly correlated with cervical cancer risk in both Caucasians and Asians (OR = 20.19, 95% CI = 2.59–157.38, p = 0.004; OR = 9.61, 95% CI = 2.63–35.08, p = 0.001, respectively; Figure 5).

Subgroup analysis of FHIT promoter methylation by ethnicity based on the comparison between cervical cancer and normal controls.
Sensitivity analysis of FHIT promoter methylation and cancer risk (cancer vs normal controls)
In the comparison between cervical cancer and normal controls, sensitivity analysis of FHIT promoter methylation was conducted by omitting an individual study to assess the stability of the pooled result. We omitted the study by Kang et al. 19 and re-calculated the overall result from the remaining studies. The pooled OR was 14.08 (95% CI = 7.23–27.43), resulting in a significantly decreased heterogeneity (I2 = 0.0%, p = 0.649; Figure 6).

Sensitivity analysis of FHIT promoter methylation based on the comparison between cervical cancer and normal controls.
Correlation of FHIT promoter methylation with clinicopathological features
The result from four studies involving 277 cervical cancer patients suggested that the FHIT promoter methylation frequency was significantly higher in advanced-stage (stages 3–4) cervical cancer compared with early-stage patients (stages 1–2; OR = 2.69, 95% CI = 0.97–7.41, p = 0.056; Figure 7).

Forest plot of the correlation of RARβ and FHIT promoter methylation with clinicopathological features, including clinical stage, tumor grade, and histology.
There was also more FHIT promoter methylation in high-grade cervical cancer (grade 3) compared to low-grade patients (grades 1–2), with the combined OR of 4.11 (95% CI = 2.28–7.41, p < 0.001), which was calculated from three studies with 251 cervical cancer patients (Figure 7). More studies with large sample sizes are necessary to further confirm the relationship between RARβ and FHIT promoter methylation and clinicopathological features of cervical cancer patients.
RARβ or FHIT alteration from the Cancer Genome Atlas Research Network
The data from the Cancer Genome Atlas Research Network were finally analyzed to evaluate the association between RARβ or FHIT alteration and the survival of cervical cancer in terms of overall survival (OS) and disease-free survival (DFS; 38 www.cbioportal.org). The result involving 309 samples indicated that RARβ or FHIT alteration was not correlated with the prognosis of patients with cervical cancer in terms of OS or DFS (p > 0.1; Table S1).
Discussion
Aberrant promoter methylation of TSGs plays an important role in the initiation and progression of various types of human cancers.39–42 Numerous studies have suggested that aberrant methylated TSGs within the promoter regions inactivate the genes, leading to the expression loss and dysfunction.8,43,44 The loss of TSGs through promoter methylation may affect cell proliferation, cell death, cell migration, and cell invasion in cancers. 45 In cervical cancer, the loss or downregulation of RARβ expression was observed to be correlated with RARβ promoter methylation.29,32,36 Similarly, the loss of FHIT expression was also shown to be associated with its promoter methylation in cervical cancer.35,46,47 The promoter methylation of TSG RARβ and FHIT may play a crucial role in the pathogenesis of cervical cancer.20,32
With respect to the frequency of RARβ and FHIT promoter methylation in cervical cancer, CIN lesions, and normal samples, there exist some controversial results. Pathak et al. 18 reported that no correlation in terms of RARβ promoter methylation was found between cervical cancer and CIN lesions, but RARβ promoter methylation was notably higher in cervical cancer than in normal cervical tissues. However, according to the study by Feng et al., 22 the level of RARβ promoter methylation was significantly higher in cervical cancer than in CIN lesions. However, although significant difference regarding FHIT promoter methylation was found between cervical cancer and CIN lesions according to some studies,20,37 Banzai et al. 28 indicated that no significant relationship was observed. Thus, we explored whether RARβ and FHIT promoter methylation was correlated with cervical carcinogenesis in the samples from cervical cancer, CIN lesions, and normal controls. Our results showed that RARβ and FHIT promoter methylation was significantly higher in cervical cancer than in CIN lesions and normal samples, which suggested that RARβ and FHIT promoter methylation may be involved in the cervical carcinogenesis. Considering the small sample sizes, the results according to the comparison between cervical cancer and CIN lesions (FHIT gene) and the comparison between cervical cancer and normal cervical tissues (RARβ gene) should be treated with caution in our study.
Furthermore, whether RARβ or FHIT promoter methylation was correlated with the progression and prognosis of cervical cancer was also analyzed based on the data presented in more than two studies. The results revealed that FHIT promoter methylation was significantly associated with the clinical stage and tumor grade of cervical cancer, which was higher in advanced-stage and high-grade patients. Thus, FHIT promoter methylation may play a critical role in the progression of cervical cancer. Additional studies with large sample size of cervical cancer patients are essential to further validate the relationship between RARβ or FHIT promoter methylation and clinicopathological features and survival outcomes in the future.
For the heterogeneity originated from the comparison of FHIT promoter methylation between cervical cancer and normal controls, we conducted a sensitivity analysis to evaluate the influence by omitting an individual study. When removing the study by Kang et al., 19 the pooled OR remained significant with no evidence of heterogeneity, indicating the stability of the current analyses. The reason for bias in the current meta-analysis was not very clear, possibly due to the inappropriate use of different primers and conditions (MSP method) in the detection of FHIT promoter methylation.
Our results were consistent with the previous study by Wentzensen et al. 48 In addition, the sample sizes included in the current meta-analysis (RARβ: 1178 samples and FHIT: 1144 samples) were larger than the previous meta-analysis (RARβ: 780 samples and FHIT: 983 samples). Furthermore, the previous study did not analyze the relationship between RARβ or FHIT promoter methylation and cervical cancer among different subgroups.
Several limitations should be mentioned in the present meta-analysis. First, only full-text papers published in English were selected in the study. Papers in other languages were excluded because of unreadable contents or insufficient data, which may result in a selection bias. Second, for the analyses based on fewer than three studies, more prospective clinical studies are needed to confirm the clinical significance of RARβ or FHIT promoter methylation in cervical cancer in the future. Third, with respect to whether FHIT promoter methylation was correlated with the prognosis of cervical cancer, more studies are necessary to validate the prognostic role of FHIT promoter methylation. Finally, only two studies reported that RARβ promoter methylation was not correlated with the survival of patients with cervical cancer.27,36
In conclusion, our findings reveal that RARβ and FHIT promoter methylation is higher in cervical cancer than in CIN lesions and normal controls. RARβ promoter methylation is not significantly correlated with clinical stage, tumor histology, or the survival of cervical cancer patients. FHIT promoter methylation may be associated with the progression of cervical cancer. Further prospective clinical studies with large samples sizes are essential to confirm our findings in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Program of Jiangxi Provincial Department of Science and Technology (20151BBG70196).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.