
Abstract
The aim of this study is investigate the influence of endoscopic sinus surgery on the quality of life and prognosis of patients with early nasopharyngeal carcinoma. Patients initially diagnosed with early nasopharyngeal carcinoma and received surgical treatment were matched with nasopharyngeal carcinoma patients who received chemoradiotherapy at a ratio of 1:1, according to the following seven factors: gender, age, T staging, N staging, clinical staging, radiotherapy options, and chemotherapy options. Patients in the surgery group received endoscopic sinus surgery plus chemoradiotherapy, while subjects in the control group received chemoradiotherapy. The quality of life of patients before and after treatment was evaluated based on the FACT-H&N (Functional Assessment of Cancer Therapy-Head and Neck) and QLQ-H&N35 (Head and Neck Cancer Specific Module) questionnaires. In addition, overall survival and disease-free survival were compared between these two groups. The results showed overall survival was superior in the surgery group compared with the control group (p = 0.007). However, the difference in disease-free survival between these two groups was not statistically significant (p = 0.128). Furthermore, subgroup analysis revealed that for N0 patients, the effect of surgery combined with chemoradiotherapy on overall survival was superior to that of chemoradiotherapy (p = 0.048); while for N1 patients, the difference in overall survival between these two groups was not statistically significant (p = 0.065). For early nasopharyngeal carcinoma patients without lymph node metastasis, overall survival and disease-free survival in T1 patients were superior to those in T2 patients (χ2 = 4.403, p = 0.036; χ2 = 4.542, p = 0.033). At the end of treatment, the pain score was found to be significantly lower in the surgery group than in the chemoradiotherapy group (p = 0.027). At 3 months and 1 year after treatment, dry mouth scores were significantly lower in the surgery group than in the chemoradiotherapy group (p = 0.002, p = 0.026). These results demonstrated that the curative effect of surgery combined with chemoradiotherapy in the treatment of nasopharyngeal carcinoma was satisfactory and was particularly suitable for N0 patients.
Keywords
Introduction
Nasopharyngeal carcinoma (NPC) is a malignant tumor common in the southern region of China. 1 Since the anatomical location of the nasopharynx is deep, early local lesions cannot easily be found, and most of these patients are in the middle and late stages of NPC when were diagnosed. The preferred regimen for middle and late stage NPC is concurrent chemoradiotherapy. For early NPC (stage I and II), majority of scholars have advocated concurrent chemoradiotherapy, 2 while some scholars do not advocate chemotherapy due to its side effects. 3 It is certain that the prognosis of patients with early NPC is satisfactory, and the 5-year survival rate is 89.7%. 4 However, the required radiation dose is high and its sequelae seriously affect the quality of life of patients, which is one of the urgent problems that need to be solved at present. Related studies have been carried out in our department since 1987. We have resected the primary lesions of NPC via the hard palate approach and administered a reduced dose of radiotherapy and chemotherapy for patients after surgery, achieving relatively satisfactory results. However, the hard palate approach is difficult to popularize due to large trauma, small surgical field, and long postoperative recovery time. Since July 2008, we have also resected primary lesions via minimally invasive endoscopic sinus surgery instead of the hard palate approach surgery. Up to July 2013, a total of 64 patients with early NPC were treated. Details are reported as follows.
Data and methods
Clinical data
Between July 2008 and July 2013, a total of 1139 patients admitted in the Nasopharyngeal Carcinoma Research Institute of the People’s Hospital of the Guangxi Zhuang Autonomous Region were diagnosed with NPC by pathology. Before treatment, all patients received essential examinations such as magnetic resonance imaging (MRI), B ultrasound, chest X-ray, and blood biochemical tests. According to the 2007 NPC staging of the Union for International Cancer Control (UICC), a total of 339 patients were in the early stage. According to selection criteria of this study, 339 patients were at the early stage. Among these patients, 128 patients (64 pairs) were included in this study. The specific selection criteria were as follows—Inclusion criteria: (1) patients pathologically diagnosed with early NPC (stage I and II), (2) patients who were between 18–70 years, (3) patients with Karnofsky scores >80 points, and (4) patients who agreed to participate in this study and provided a signed informed consent. Exclusion criteria: (1) T2 patients with oropharynx invasion or posterior parapharyngeal space involvement, or patients with parapharyngeal lymph node enlargement; (2) patients who suffer from severe liver and kidney damage or serious heart, cerebrovascular, and respiratory system diseases; (3) patients who suffer from hemorrhagic diseases, diabetes, and other systemic diseases; and (4) patients projected to have poor compliance. Elimination criteria: (1) patients who could not complete the planned treatment due to various reasons and (2) patients who were required to withdraw from the study. The enrolled subjects comprised 100 males and 28 females, and the age of these subjects ranged between 22 and 66 years, with a median age of 45 years.
Methods
Grouping method
Patients were divided into two groups according to the treatment methods patients received: surgery group and control group. The patient’s condition, as well as the advantages and disadvantages of various treatment regimens, was introduced to the patient and their families by the physician in charge. Then, the patients themselves chose the treatment regimen and signed an informed consent. The stage-matching pairing of patients who chose chemoradiotherapy and surgery plus chemoradiotherapy was performed by the physician in charge according to NPC cell type, T staging, N staging, clinical staging, chemotherapy regimen, age (n ± 5 years), and gender.
Treatment regimen in the surgery group
Patients in the surgery group received endoscopic sinus surgery plus concurrent chemoradiotherapy. Before surgery and in the interval between surgery and chemoradiotherapy, MRI of the nasopharynx, skull base, and neck was performed for all patients. Specific procedures were as follows—(A) Surgical method: The surgery was performed under general anesthesia. Patients were laid in the supine position, and their nasal mucosa was stimulated to contract two to three times by a cotton piece treated with 1% adrenaline hydrochloride. The tumors in the nasopharynx were resected via the nasal approach guided by a nasal endoscope (Figure 1). After surgery, the nasal and nasopharyngeal cavities were obturated with Surgicel and an expansion sponge for hemostasis. For N1 patients, functional neck dissection was performed during the same period. According to the results of the MRI examination of the nasopharynx and skull base, the scope of resection of the primary lesion was determined—Roof and posterior wall: clivus, inferior wall of the sphenoid sinus, and part of the anterior wall; Lateral wall: musculus pterygoideus internus; Front boundary: nasal septum and posterior part of the nasal cavity; Low boundary: flat soft palate. The dissection scope was determined according to preoperative cervical MRI and B ultrasound examination results and intraoperative findings. Within 1 week after the surgery, MRI was performed again (Figure 2). (B) Chemotherapy: (1) Approximately 30–40 mg/m2 of cisplatin was intravenously injected from first to third day; 2000 mg/m2 of flurouracil was continuously infused for 120 h; the course of treatment was every 21 days and two to three courses of treatment were performed for each patient. (2) At the first day, 500 mg/m2 of carboplatin was used and 2000 mg/m2 of flurouracil was continuously infused for 120 h; the course of treatment was every 21 days and two to three courses of treatment were performed for each patient. (3) Radiotherapy: Conventional radiotherapy was performed as follows: the in vitro radiation source was a 6–8 mV high-energy X-ray source, the scope of irradiation included the nasopharynx, skull base, and neck; the irradiation method was conventional continuous radiotherapy: 2 Gy/time, 1 time/day, and 5 times/week. Intensity-modulated radiation therapy (IMRT): The target area was sketched based on the boundaries of the tumor image acquired by MRI. The following doses of irradiation were performed—gross tumor volume (GTV): 2.0–2.2 Gy/time; planning target volume (PTV): 1.8/2.0 Gy/time; 5 days/week. The total dose was 50–60 Gy for GTV and 45–60 Gy for PTV.

Comparison of total survival rate of different treatment methods.

Comparison of survival rate of different treatment methods.
Treatment methods for the control group
(1) The chemotherapy regimen and dose were the same with those in the surgery group; (2) the radiotherapy regimen was the same with that in the surgery group, and the total dose was 50–60 Gy for GTV.
The survival rates observed included the following
(1) The 3-year overall survival (OS) and disease-free survival (DFS) rates in all patients, (2) the 5-year OS and DFS rates in two groups of patients, (3) the 3-year and 5-year OS and DFS rates in T1N1 patients in the two groups, (4) the 3-year and 5-year OS and DFS rates in T2N1 patients in the two groups, (5) the 3-year and 5-year OS and DFS rates in stage I patients in the two groups, and (6) the 3-year and 5-year OS and DFS rates in stage II patients in the two groups.
Evaluation method of the quality of life of patients
The quality of life of patients was compared between the two groups before treatment, at 3 months and 1 year after treatment, based on the Functional Assessment of Cancer Therapy-Head and Neck (FACT-H&N) and head and neck cancer specific module (QLQ-H&N35) questionnaires. The FACT-H&N questionnaire comprised a core questionnaire FACT-G and a specific sub-scale (additional concern) for the evaluation of head and neck tumors. FACT-G includes four sub-scales: physiological status, functional status, emotional status, and social and family status. The standard score was 108 points. The specific sub-scale consists of 11 questions related to head and neck organ functions, with a standard score of 36 points. The higher the score is, the better the quality of life. QLQ-H&N35 consists of 35 items, including even fields and 11 solitary items. The seven fields are pain, swallowing difficulty, sensory disorder, language disorder, eating difficulty, social disorder, and sexual life. The 11 solitary items are dental problems, trismus, dry mouth, sticky saliva, cough, morbid sense, the use of painkillers, history of nutrient use, the use of a nasogastric tube, loss of body weight, and increase in body weight. The higher the score is, the worse the quality of life becomes.
Statistical methods
Raw data were input into the Excel software. The raw score (RS) acquired by the scales was converted to the standard score that ranged within 0–100 points. Then, these were analyzed using SPSS 18.0 software. Count data were compared using the χ2 test, and measurement data were compared using t test. Univariate survival analysis was conducted using Kaplan–Meier survival curves, and these survival curves were compared between groups using log-rank test. p < 0.05 was considered to be statistically significant.
Results
Selection of patients in the two groups
A total of 128 patients (64 pairs) were included in this study, according to the case selection criteria and grouping method. The case data of these two groups are listed in Table 1.
General data distribution of the two groups.

Three patients disagree with cervical lymph node dissection operation.
Recurrence and metastasis
Among these 128 patients, local recurrence occurred in two patients, lymph node recurrence occurred in one patient, and distant metastasis occurred in 10 patients; and all these occurred after treatment. In the surgery group, recurrence occurred in one patient and recurrence time was 47 months, while distant metastasis occurred in three patients with a median time of 9 months. In the chemoradiotherapy group, recurrence occurred in two patients and recurrence times were 17 and 49 months, respectively, while distant metastasis occurred in seven patients with a median time of 9 months. The differences in recurrence and metastasis rates between these two groups were not statistically significant (χ2 = 2.140, p = 0.143). Furthermore, tumor recurrence and metastasis rates were significantly lower in patients who underwent cervical lymph node dissection compared with patients who did not undergo this procedure, but the differences were not statistically significant (p = 0.359, Table 2).
Recurrence and metastasis.

OS and DFS rates
The 3-year OS was 95.22% and 3-year DFS was 92.10% in all patients, while 5-year OS was 91.53% and 5-year DFS rate was 88.09% in all the patients. In the surgery group, 3-year and 5-year OS rates were 98.44% and 98.44%, respectively, while in the chemoradiotherapy group, 3-year and 5-year OS rates were 91.98% and 84.21%, respectively. OS was superior in the surgery group compared with the chemoradiotherapy group (χ2 = 7.220, p = 0.007), and the difference in DFS between these two groups was not statistically significant (χ2 = 2.316, p = 0.128, Figures 1 and 2). For N0 patients, the effect of surgery combined with chemoradiotherapy on OS was superior to that of chemoradiotherapy alone (χ2 = 3.906, p = 0.048), while for N1 patients, the difference in OS between these two groups was not statistically significant (χ2 = 3.393, p = 0.065, Figures 3 and 4).
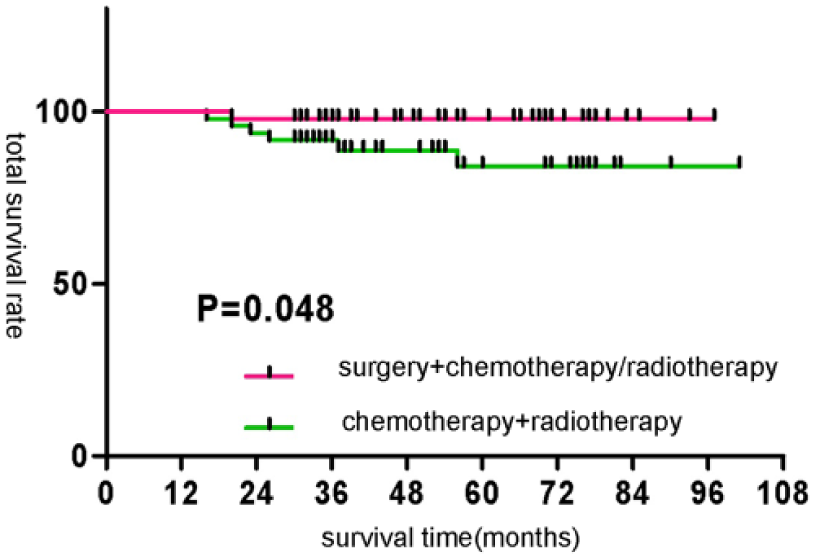
Comparison of survival rate of different treatment methods for T1–2N0 nasopharyngeal cancer.
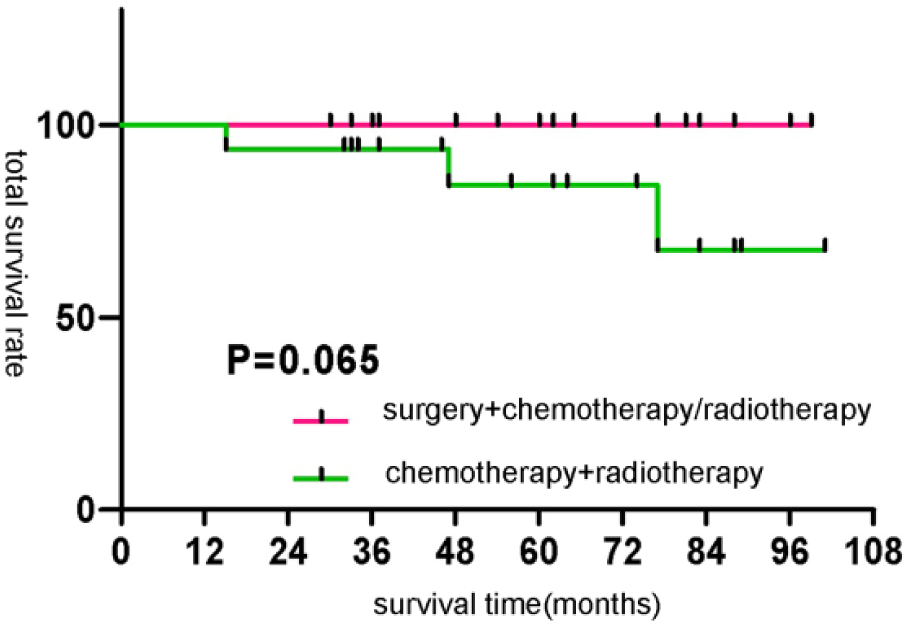
Comparison of survival rate of different treatment methods for T1–2N1 nasopharyngeal cancer.
Radiotherapy dose comparison
The median radiotherapy dose was 60 Gy in the surgery group and 72 Gy in the chemoradiotherapy group, and the difference between these two groups was statistically significant (t = 40.356, p = 0.000).
Comparison of quality of life at each time point
Before treatment, differences in quality of life scores (FACT-H&N and QLQ-H&N35, as well as its items) between these two groups were not statistically significant (p > 0.05 for all). At the end of treatment, pain score was significantly lower in the surgery group than in the chemoradiotherapy group (p = 0.027). At 3 months and 1 year after treatment, dry mouth scores were significantly lower in the surgery group than in the chemoradiotherapy group (p = 0.002, p = 0.026). Surgical treatment also improved the patient’s physical condition and contributed to weight gain, and the differences between these two groups were statistically significant (p < 0.05 for all; Tables 3–5).
Comparison of quality of life at the end of surgery and radiation and chemotherapy in patients (
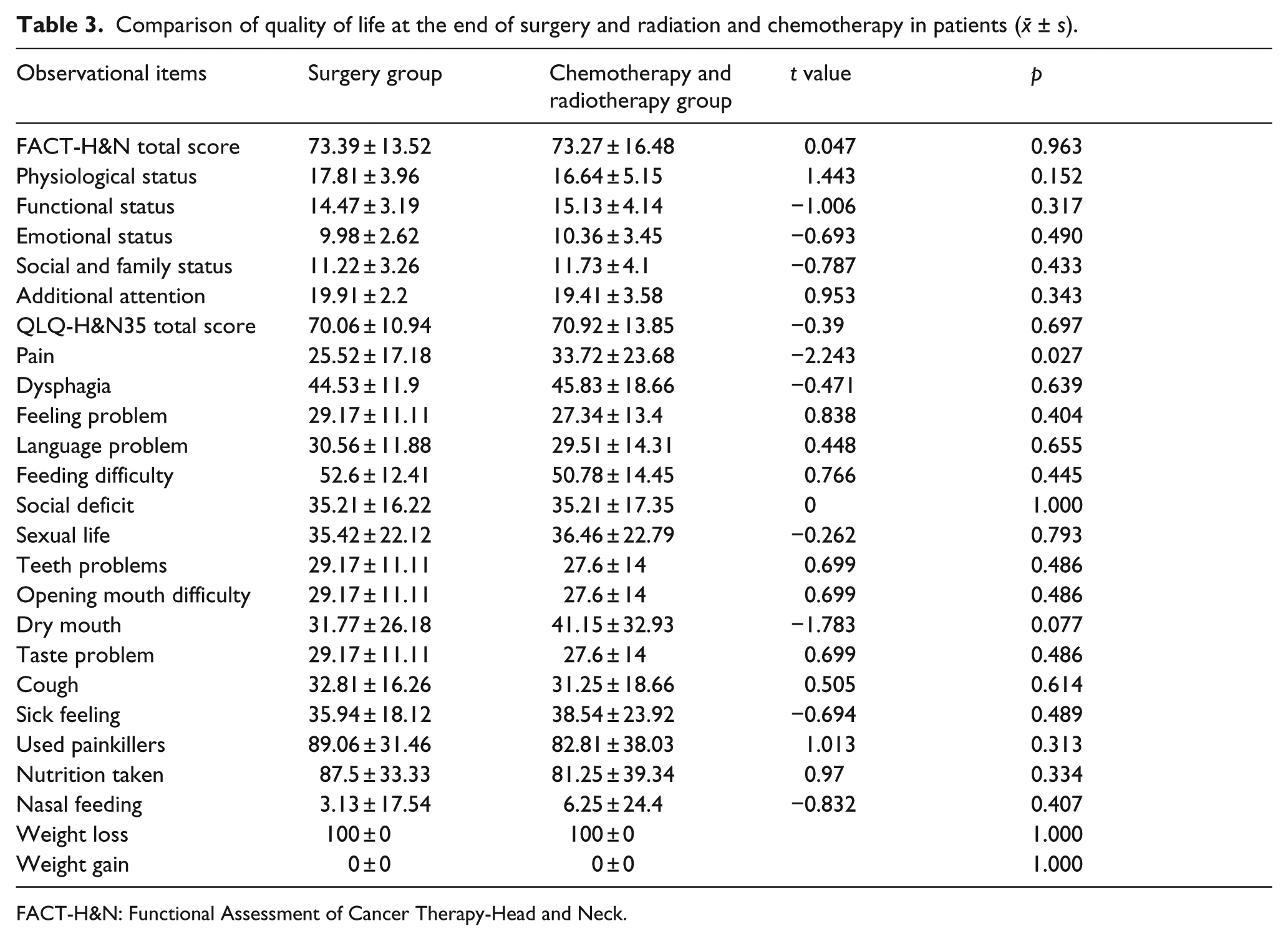
FACT-H&N: Functional Assessment of Cancer Therapy-Head and Neck.
Comparison of quality of life at the 3 months of surgery and radiation and chemotherapy in patients (

FACT-H&N: Functional Assessment of Cancer Therapy-Head and Neck.
Comparison of quality of life at the 1 year of surgery and radiation and chemotherapy in patients (

FACT-H&N: Functional Assessment of Cancer Therapy-Head and Neck.
Discussion
The anatomy of the nasopharynx is complex and is located adjacent to vital organs. In the past, it was considered that it was difficult to surgically remove NPCs. In addition, most NPCs are sensitive to radiotherapy. Therefore, radiotherapy is the main means of treatment for initially diagnosed NPCs. Furthermore, chemotherapy can be used to improve the prognosis of patients with middle and advanced NPCs. It was reported in a previous literature that the 5-year OS rate of patients with middle and advanced NPC was 75%, 5 and this rate was as high as 89.7% for patients with early NPCs. 4 However, recurrence and metastasis continued to occur in some patients. In order to improve the curative effect, some scholars advocate that early NPC patients should undergo chemotherapy. 2 However, other scholars have held opposite views. 6 They consider that chemotherapy cannot benefit patients; on the contrary, it can increase the side effects and reduce the quality of life of patients. Many studies have confirmed that IMRT could increase the local control rate and OS of patients, and reduce the incidence of xerostomia and trismus,7,8 but not that of radiation-induced oral mucositis (ROM). Therefore, determining a method of treatment that can be used to manage tumors and avoiding normal tissue damage has been a hot topic in clinical research.
In the early stage of this study, we surgically removed the initially diagnosed NPC via the external nasal approach (hard palate approach) and performed reduced-dose radiotherapy after surgery. As a result, a good curative effect was obtained. 9 However, the surgical field in the hard palate approach is small and causes the hard palate osseous substance to be injured. This reduces the quality of life of patients to a certain extent. Endoscopic sinus surgery can avoid the disadvantages of the hard palate approach. A number of scholars have applied endoscopic sinus surgery to remove recurrent NPC,10,11 achieved a better curative effect than that of re-radiotherapy, and improved the quality of life of patients. Based on this, we applied endoscopic sinus surgery to remove the primary lesions in initially diagnosed NPC patients. For patients with lymph node metastatic carcinoma, functional neck lymph node dissection was additionally performed. In the surgery group, 3-year and 5-year OS rate was 98.44% and 98.44%, respectively, and in the control group, 3-year and 5-year OS rate was 91.98% and 84.21%, respectively. The difference in DFS between these two groups was not statistically significant. Few literatures have reported the removal of NPC by endoscopic sinus surgery. Castelnuovo et al. 12 reported that the endoscopic resection of nasopharyngeal tumors would bring about good curative effects, in which 5-year survival rate was 75.1%. In the past, it was customarily considered that the skull base was the operative forbidden zone. The reason is that the anatomy of the nasopharynx is complex, and it is adjacent to important nerves and vessels. With the development of endoscopic technology, a study reported the application of endoscopic sinus surgery for the removal of recurrent T3 (rT3) NPC in recent years. 13 It was considered that the indications of the initially diagnosed NPC that can be surgically removed include the pathological types of adenocarcinoma or highly differentiated squamous cell carcinoma. The data in this study revealed that the pathological types of the included patients were undifferentiated non-keratinzing cancers, which was similar to previous research results.9,14 OS in the surgery group was better than in the chemoradiotherapy group. Furthermore, we analyzed and considered that the possible reason was that surgery could remove the primary lesions of tumors in one time. A previous study has confirmed that the prognosis of patients was associated with the presence of residual tumors after treatment. 15 In general, residual tumors are found in 7%–10.52% of patients who undergo chemoradiotherapy.16,17 For residual tumors, the reasons may be as follows: (1) tumors are resistant to radiation, and (2) the presence of tumor stem cells.
Lymph node metastasis is a risk factor that affects the prognosis of patients with NPC. 18 Our data revealed that endoscopic sinus surgery could improve prognosis for N0 patients but could not significantly improve the prognosis of N1 patients. Furthermore, analysis revealed that this may be related to part of the N1 patients who did not agree to undergo neck lymph node dissection due to fear of neck scarring. In the data for this study, three N1 patients did not undergo neck lymph node dissection, and out of the 13 patients who underwent neck lymph node dissection, no patient encountered recurrence and metastasis after surgery, although the difference was not statistically significant. However, this may be related to the small number of patients who underwent non-neck dissection. Therefore, in the next step, it is necessary to perform surgical treatment and follow-up for this type of patients.
Radiotherapy is the most important means of initially diagnosing NPCs without distant metastasis. Since the head and neck are unavoidably in the irradiation range, the incidence of ROM is 100%, which is the most common complication of radiotherapy. ROM leads to pain, decrease in intake, and treatment interruption in patients. In addition, treatment interruption may affect the prognosis of patients. Ideal radiotherapy technology should be given at a high dose to the target area according to the shape of the tumor, and normal tissues around the target area should not affected by irradiation. Compared with 2D-radiotherapy (2DRT), current IMRT significantly reduces the incidence of truisms. 7 However, normal tissues continue to receive a considerable dose of irradiation. For example, the incidence and severity of ROM in patients undergoing IMRT is not lower compared with patients undergoing 2DRT. Therefore, some scholars have put forward the reduced-dose radiotherapy. 19 The data in this study revealed that the dose for patients in the surgery group was also reduced to 60 Gy, which was significantly lower than that in the chemoradiotherapy group (70 Gy). The evaluation of ROM at the end of treatment revealed that the degree of pain was significantly lower, compared with that in the chemoradiotherapy group. During the follow-up at 3 months and 12 months after treatment, it was also found that the severity of xerostomia was lower in the surgery group. Little et al. 8 revealed that the severity of xerostomia was related to the total dose of radiotherapy the salivary gland received. Therefore, we concluded that slighter pain and xerostomia in the surgery group was mainly due to the lower dose of radiotherapy. The median radiotherapy dose was 60 Gy in the surgery group and 72 Gy in the chemoradiotherapy group. In the earlier stage of our study, it was also found that surgical treatment and nasal irrigation were protective factors of ROM. 20 The fast restoration of body weight in patients in the surgery group may be related to lighter pain and xerostomia, as well as more intake in patients in the surgery group.
The limitation of this study is that the sample used was small. Furthermore, a sub-group should be set in the surgery group, in which the radiotherapy dose is the same with that in the chemoradiotherapy group, in order to perform a better control. Based on the current data, the curative effect of surgery combined with chemoradiotherapy is better than that of conventional chemoradiotherapy, is especially suitable for N0 patients, and can reduce the incidence of ROM and xerostomia to some extent. Hence, this is worthy of further studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by major projects of Guangxi science and technology development projects (Gui Science Attack 14124003-3), Guangxi fit health technology research and development projects (Gui Health S201313-03) and Scientific Research Project of Guangxi Health and Family Planning Commission (Z2014629).