
Abstract
The Platelet to lymphocyte ratio (PLR) has been reported to predict prognosis of patients with hepatocellular carcinoma (HCC). This study examined the prognostic potential of stratified PLR for HCC patients undergoing curative liver resection. Medical records were retrospectively analyzed for 778 HCC patients undergoing curative liver resection at the Affiliated Tumor Hospital of Guangxi Medical University and the First People’s Hospital of Changde between April 2010 and October 2013. Patients were stratified based on quintile analysis of their preoperative PLR, and patients in different quintiles were analyzed for overall survival (OS) and disease-free survival (DFS) using Kaplan-Meier analysis. Independent predictors of death or recurrence were explored using multivariable Cox proportional hazard regression. Higher PLR quintiles were significantly associated with poorer overall survival (p < 0.001). Multivariate analysis showed PLR to be an independent risk factor for OS (p = 0.003). Patients in PLR quintile 5 had lower overall survival than in quintile 1 (hazard ratio (HR) = 2.780, 95% confidence interval (CI): 1.769–4.367, p < 0.001). Although patients in PLR quintile 5 had significantly lower disease-free survival (DFS) than in quintile 1 (HR = 1.534, 95% CI: 1.112–2.117, p = 0.009), this association was not significant after multivariable adjustment (p = 0.220). Subgroup analysis also showed that PLR quintiles were significantly associated with poor OS in patients positive for HBsAg or with cirrhosis (both p < 0.001). Similar results were obtained when PLR was analyzed as a dichotomous variable with cut-off values of 110 and 115. Elevated preoperative PLR may be independently associated with poor OS and DFS in HCC patients following curative resection.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is one of the most commonly occurring malignancy and the third major cause of tumor-related death in worldwide.1–3 Even though hepatectomy has reached significant improvements, the prognosis of patients with HCC is far from satisfactory due to tumor recurrence and distant metastasis.4,5
Several criteria have been suggested to predict HCC patient prognosis, such as Tumor Node Metastasis (TNM), functional liver reserve, and Barcelona Clinic Liver Cancer (BCLC) score. However, as these criteria are cumbrous, they are seldom used in clinical practice. Thus, identification of a simple, efficient, and easily obtained biomarker for prognosis and recurrence of patients with HCC is necessary.
Systemic inflammatory response plays a key role in the pathogenesis and progression of tumor. 6 Inflammation index, such as neutrophil-to-lymphocyte ratio (NLR), C-reactive protein (CRP), lymphocyte–monocyte ratio (LMR), 7 and platelet-to-lymphocyte ratio (PLR), has been identified as prognostic biomarker in multiple cancers.7–11
Among these markers, high PLR was considered as a poor prognostic factor in multiple cancers such as breast cancer, 12 colorectal cancer, 13 and gastric cancer. 14 The prognostic value of PLR in HCC has also been investigated.15–17
However, conflicting results have emerged regarding the prognostic value of PLR to foretell disease-free survival (DFS) and overall survival (OS) in HCC.
Therefore, we intend to construct the stratification with PLR to enhance the prognostic utility for patients with HCC.
Materials and methods
This research was approved by the Ethics Committee of the Affiliated Tumor Hospital of Guangxi Medical University and the First People’s Hospital of Changde, and written informed consent was obtained from patients prior to surgery.
Patients
All patients with HCC who underwent liver resection with curative intent at the Affiliated Tumor Hospital of Guangxi Medical University and the First People’s Hospital of Changde between April 2010 and October 2013 were included in our study. The inclusion criteria were as follows: initial hepatectomy with curative intent performed at the authors’ centre; no treatment for HCC before hepatectomy; no other simultaneous malignancies; no coexistent hematologic disorders, so that the preoperative platelet count reflected normal baseline values; and no cerebral, renal, or cardiopulmonary dysfunction before hepatectomy.
Diagnosis and definitions
Diagnose of HCC was based on histological evidence after operation. Liver resection with curative intent is defined with complete resection of all visible tumor and no residual tumor cells at surgical margins. 18 PLR was calculated as the absolute platelet count divided by absolute lymphocyte. Complete blood count (CBC) samples were generated by the automated hematology analyzer (DxH800; Beckman Coulter Inc., Miami, FL, USA). Preoperative PLR was determined within 7 days before surgery.
Follow-up visits
All patients were followed up at 1 month after hepatectomy and subsequently at 3-month intervals in the first year, and then every 3–6 months in subsequent years, as appropriate. At each follow-up visit, serum fetoprotein (AFP) assay, serum biochemistry, ultrasound, chest X-ray, and abdominal computed tomography (CT) or magnetic resonance imaging (MRI) were performed.
Statistical analysis
Statistical analysis was performed using SPSS 19.0 (IBM, Armonk, NY, USA). Continuous variables were analyzed by nonparametric Kruskal–Wallis test or the one-way analysis of variance (ANOVA), as appropriate. Differences of categorical data were analyzed by two-sided χ2 test, Mann–Whitney U test, or Fisher’s exact test, as appropriate.
Based on the distribution of PLR and the size of the study population, patients with HCC were stratified into quintiles of the PLR (quintile 1, quintile 2, quintile 3, quintile 4, quintile 5). Receiver operating curve (ROC) analysis identified 110 as the PLR cut-off giving the greatest sensitivity and specificity in our cohort (Figure 1). Survival analysis was performed to compare the OS and DFS rates using Kaplan–Meier survival curves with log-rank tests and Cox proportional hazard regression analyses, and p <0.05 was considered statistically significant.

Receiver operating curve (ROC) for the preoperative PLR (platelet-to-lymphocyte ratio) with an optimal cut-off value of 110 (sensitivity 53.5%, specificity 63.3%).
Results
Baseline characteristics of all patients in PLR quintiles
During the study period, a total of 1015 patients with HCC underwent hepatectomy with curative intent at our hospital. Of these, 237 patients with HCC (23.3%) were excluded for the following reasons: 188 patients with HCC (18.5%) underwent other treatments before hepatic resection; 21 patients (2.1%) had other malignant tumors simultaneously; 15 patients (1.5%) had coexistent hematologic disorders; and 13 patients (1.3%) had cerebral, renal, or cardiopulmonary dysfunction before hepatic resection. In the end, 778 patients (76.7%) were enrolled in the study.
The study consisted of 107 females and 671 males. Details of demographic and clinical characteristics are presented in Table 1. According to the quintiles of PLR, the patients with HCC were divided into five groups, and this method offered most categories with a sufficient number of patients with HCC per category from the range of 10–433.The cut-off points of this stratification were as follows: (Q1) 10 ⩽ PLR ⩽ 66, (Q2) 66 < PLR ⩽ 87, (Q3) 87 < PLR ⩽ 110, (Q4) 110 < PLR ⩽ 150, and (Q5) 150 < PLR ⩽ 433 (Table 1).
Characteristics of 778 patients with HCC treated by resection according to PLR quintile.

PLR: platelet-to-lymphocyte ratio; HBsAg: hepatitis B surface antigen; AFP: alpha-fetoprotein; BCLC: Barcelona Clinic Liver Cancer; AST: aspartate aminotransferase; ALT: alanine aminotransferase.
Data are mean ± standard deviation or median (25th–75th interquartile range) unless otherwise indicated.
A higher PLR was significantly associated with higher values of BCLC grade, Child–Pugh grade, tumor size, platelet counts (PLT), and total bilirubin (all p < 0.05). On the other hand, A higher PLR was significantly associated with lower values of albumin and alanine aminotransferase (ALT; both p < 0.05).
Cox analyses of survival associated with PLR
Unadjusted univariable Cox proportional hazard models were used to identify factors associated with OS and DFS, and the detailed results are shown in Table 2.
Cox proportional hazard regression models of risk factors associated with overall and disease-free survival among 778 patients with HCC.
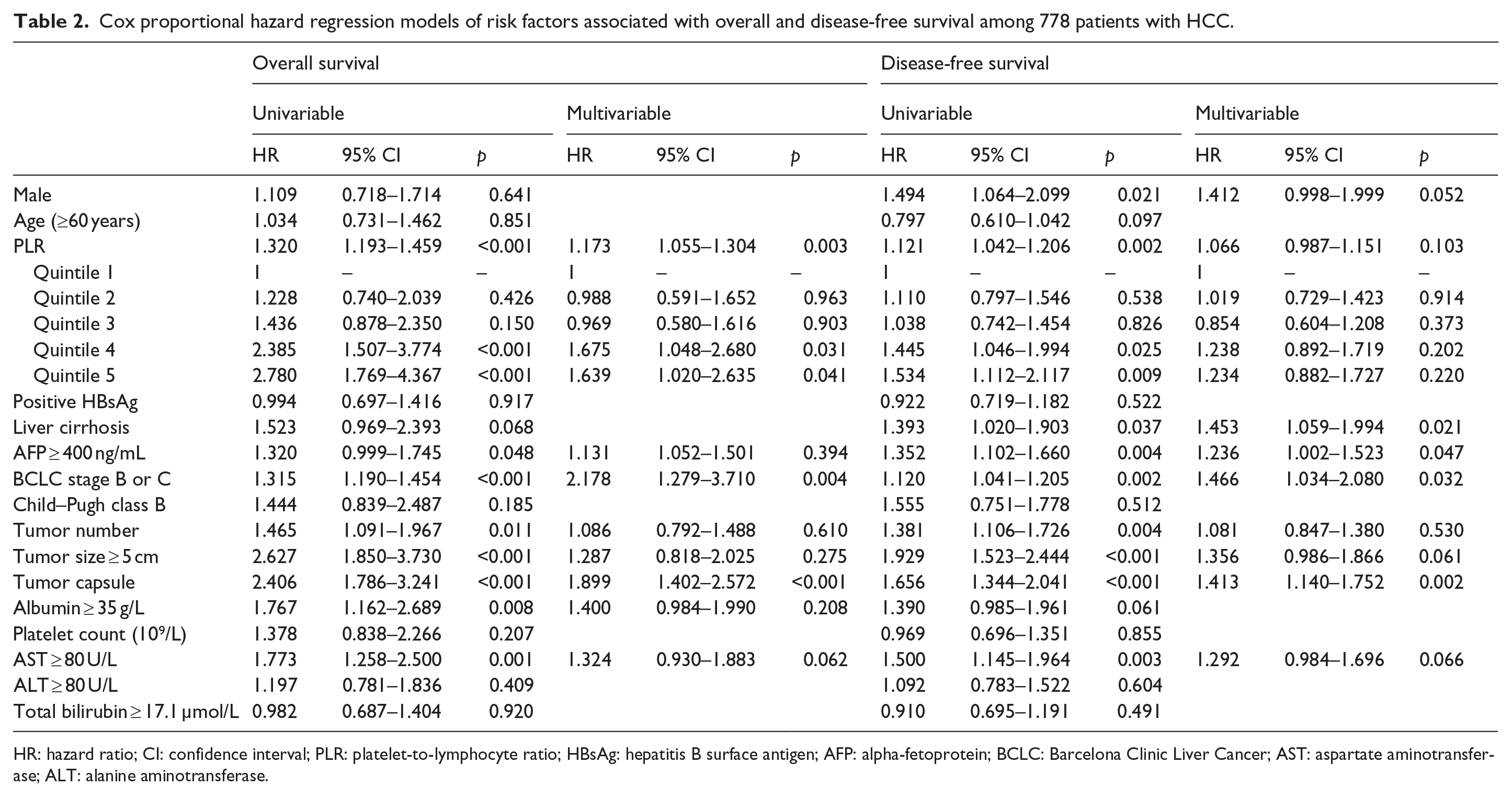
HR: hazard ratio; CI: confidence interval; PLR: platelet-to-lymphocyte ratio; HBsAg: hepatitis B surface antigen; AFP: alpha-fetoprotein; BCLC: Barcelona Clinic Liver Cancer; AST: aspartate aminotransferase; ALT: alanine aminotransferase.
The patients in highest quintile of PLR had 178% increase in hazard death and 53.4% increased hazard of having recurrence of disease compared with the first quintile (hazard ratio (HR) = 2.780; 95% confidence interval (CI): 1.769–4.367, p < 0.001 and HR = 1.534; 95% CI: 1.112–2.117, p = 0.009, respectively). Univariate analysis identified several factors significantly associated with poor OS: PLR (quintiles), AFP ⩾400 ng/mL, BCLC stage B or C, multiple tumors, tumor size ⩾5 cm, incomplete tumor capsule, albumin ⩾35 g/L, and aspartate aminotransferase (AST) ⩾80 U/L. Male, PLR (quintiles), liver cirrhosis, AFP ⩾400 ng/mL, BCLC stage B or C, multiple tumors, tumor size ⩾5 cm, incomplete tumor capsule, and AST ⩾80 U/L were also found to be significantly associated with poor DFS (Table 2 and Figure 2).

Kaplan–Meier survival curves showing (a) overall survival and (b) disease-free survival stratified by quintiles of PLR in patients with hepatocellular carcinoma.
Multivariate analysis (Table 2) identified the following independent predictors of poor OS: PLR (quintiles), BCLC stage B or C, and incomplete tumor capsule. Liver cirrhosis, AFP ⩾400 ng/mL, BCLC stage B or C, and incomplete tumor capsule were also found to be significantly associated with poor DFS.
Based on our study’s optimal cut-off value and those applied in previous studies, we chose values of 110 (our cohort), 115,19,20 and 15021,22 for the dichotomous analysis (Table 3). In the multivariate analysis, patients with HCC with the higher level of PLR were significantly associated with poor OS compared with the lower PLR using the different cut-off values of 110 and 115 (p = 0.001, p = 0.011, respectively; Table 3).However, by applying the cut-off value of 150, a higher PLR was not significantly associated with poor OS (p = 0.062; Table 3). For DFS, in the multivariate analysis, using the cut-off values of 110, 115, and 150, a high PLR was not significantly associated with the poor DFS (p = 0.053, p = 0.184, p = 0.242, respectively; Table 3).
Association between PLR and survival in patients with HCC applying different cut-off values.

PLR: platelet-to-lymphocyte ratio; HR: hazard ratio; CI: confidence interval.
Subgroup analyses associated with PLR
To elucidate the subgroups of patients with HCC negatively influenced by preoperative PLR, we stratified patients with HCC by hepatitis B virus (HBV) infection and liver cirrhosis, and we found that PLR quintiles were significantly associated with poor OS for patients with HBV infection (p < 0.001; Figure 3(a)) and significantly associated with poor DFS for patients without HBV infection (p = 0.042; Figure 3(d)). PLR quintiles were also significantly associated with poor OS and DFS for patients with liver cirrhosis (p < 0.001 and p = 0.009; Figure 4(a) and (c)) but not for patients without cirrhosis (p = 0.174 and 0.648; Figure 4(b) and (d)).

(a, b) Overall survival and (c, d) disease-free survival of patients with HCC stratified by quintiles of PLR according to (a, c) positive HBsAg and (b, d) negative HBsAg.

(a, b) Overall survival and (c, d) disease-free survival of patients with HCC stratified by quintiles of PLR according to (a, c) cirrhosis and (b, d) non-cirrhosis.
Discussion
Our research implies that higher preoperative PLR is significantly and independently associated with poor OS and DFS in patients with HCC who have suffered curative resection. The results remain robust when using cut-off values of 110 (our cohort) or 11519,20 and on analysis of the subgroups stratified by hepatitis B surface antigen (HBsAg) and cirrhosis status, especially when comparing the highest quintile of PLR with the lowest quintile. Therefore, it could be concluded that the PLR has potential utility in indicating the survival of patients with HCC.
The optimal cut-off values for prognosis are usually acquired by ROC or selected by validating previous cut-off values from other studies. When analyzing the cut-off values of PLR of 110 (our cohort) or 115,19,20 we found that PLR was also able to discriminate between those with poor OS and those with good OS in univariate and multivariate analyses using dichotomous categorization. Although patients with HCC with PLR ⩾150 was not significantly associated with poor DFS. One possible explanation is that due to the distribution of patients with HCC (Table 3), the number of patients who show preoperative PLR ⩾150 is more than four times less than preoperative PLR <150, which may lead to variance to the results.
Why elevated PLR should predict poor survival remains unclear. One possible explanation is that many patients with HCC with elevated PLR have high preoperative platelet count, which protects tumor cells from immune attack by promoting their catch at the endothelium, thus supporting the formation of secondary lesions.23,24 Elevated platelet can also release some factors, such as αIIbβ3, 25 basic fibroblast growth factor, platelet-derived growth factor, and hepatocyte growth factor, 26 which have been reported to be associated with tumor metastasis. Another possible explanation is that many patients with HCC with elevated PLR may also have decreased lymphocyte levels, which may likely reflect an impaired T-lymphocyte-mediated tumor immune response, 27 and an increasing T8/T4 ratio results in a weaker lymphocyte-mediated tumor immune response. 28 This lymphocyte-mediated tumor response normally helps eliminate abnormal cells and produces cytokines that inhibit tumor proliferation, metastasis, and invasion. 29
In summary, our study implies that the preoperative PLR is an independent prognostic factor in patients with HCC. However, a prospective research with a larger population is needed to demonstrate our researches.
Footnotes
Acknowledgements
H.-J.Y., B.-D.X., and N.-Z.C. contributed to the study design and conception. J.-H.J., Y.-f.D., and T.W. collected the relative data. H.-J.Y., Q.-A.L., and C.-M.Z. analyzed and interpreted the data. H.-J.Y., Q.-A.L., and B.-D.X. contributed to editing of the article. B.-D.X. and N.-Z.C. contributed to quality control and review of the data and article. H.-J.Y., J.-H.J., and Q.-A.L. contributed equally to this work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by grants to B.-D.X. from the National Natural Science Foundation of China (81260331). The funders had no role in study design, data collection or analysis, decision to publish, or preparation of the article.