
Abstract
Alpha-fetoprotein is an effective biomarker as an aid in hepatocellular carcinoma detection in many countries. However, alpha-fetoprotein has its limitations, especially in early hepatocellular carcinoma diagnosis. Protein induced by vitamin K absence or antagonist-II is another biomarker that is used for hepatocellular carcinoma detection. The aim of this study is to compare the diagnostic performance of alpha-fetoprotein and protein induced by vitamin K absence or antagonist-II alone and in combination to explore improving biomarker performance as an aid in early hepatocellular carcinoma detection. In this study a total of 582 serum samples including 132 hepatocellular carcinoma patients, 250 non-hepatocellular carcinoma patients, and 200 healthy volunteers were collected. Alpha-fetoprotein and protein induced by vitamin K absence or antagonist-II levels were measured by both chemiluminescent enzyme immunoassay on LUMIPULSE platform and by chemiluminescent microparticle immunoassay on ARCHITECT platform. Receiver operation characteristic curve analyses were performed for each biomarker and in combination. The results showed that Alpha-fetoprotein and protein induced by vitamin K absence or antagonist-II in combination have shown higher area under the curve compared to alpha-fetoprotein alone for diagnosis in whole patients (0.906 vs 0.870) in hepatocellular carcinoma early-stage patients (0.809 vs 0.77) and in hepatitis B virus–related hepatocellular carcinoma patients (0.851 vs 0.788) with ARCHITECT platform. Protein induced by vitamin K absence or antagonist-II showed higher area under the curve than alpha-fetoprotein for diagnosis of hepatitis B virus–related hepatocellular carcinoma patients (0.901 vs 0.788).We conclude that Combining alpha-fetoprotein and protein induced by vitamin K absence or antagonist-II may improve the diagnostic value for early detection of hepatocellular carcinoma. Protein induced by vitamin K absence or antagonist-II performs better than alpha-fetoprotein in diagnosis of hepatitis B virus–related hepatocellular carcinoma patients.
Keywords
Introduction
Liver cancer is the sixth most common cancer worldwide (for both sex) and the second most common cause of cancer death. About 745,000 people die annually around the world because of liver cancer. 1 In China, incidence and mortality of liver cancer have significantly increased in recent years. The incidence reached 29/100,000 persons while mortality reached 28.1/100,000 persons in 2010 making liver cancer to be second leading cause of cancer-related death.2,3 Liver cancer treatment and prevention for general population is a big challenge in China. 4
Alpha-fetoprotein (AFP) is the most commonly used biomarker for diagnosis of hepatocellular carcinoma (HCC) in China, which is also recommended by the National Health and Family Planning Commission (NHFPC) Guideline. 5 However, AFP is not tumor specific, which can be produced and released from injured liver tissue or other tissues.6–8 Elevated serum AFP levels also can be found in patients with non-cancerous liver diseases, for example, hepatitis or cirrhosis. 9 AFP has limitations in detecting of HCC; thus, new biomarkers for detection of HCC are needed.
Protein induced by vitamin K absence or antagonist-II (PIVKA-II), also called des-gamma carboxyprothrombin (DCP) is another biomarker for HCC.10–15 PIVKA-II and AFP are independently produced in human body and are not strongly correlated with each other. 16 Therefore, measurement of PIVKA-II and AFP panel may have better diagnostic performances on HCC compared to either AFP or PIVKA-II alone.
The aims of this study were to compare the diagnostic performance of the biomarkers alone and in combination among HCC patients; in metastatic liver cancer patients; in other non-HCC patients including viral hepatitis, cirrhosis, and other benign liver diseases; and in healthy volunteers.
Materials and methods
Patients
From September 2015 to July 2016, 148 HCC patients were recruited, 16 subjects, who were identified as non-first diagnosed HCC, were excluded according to the protocol. A total of 200 healthy volunteers and 250 non-HCC patients including 50 cirrhosis patients, 100 viral hepatitis patients, 50 metastatic hepatic carcinoma patients, and 50 other benign liver diseases were enrolled as controls. This study was performed after approval by the respective institutional review board (IRB) of Beijing Youan Hospital, Capital Medical University. This study was conducted according to the principles expressed in the Declaration of Helsinki. All serum samples are leftover samples. Informed consent process is not required per IRB approval for the use of these types of samples for this exploratory study.
All HCC patients were initially diagnosed by histological findings and without extrahepatic malignancy. HCC staging was determined by tumor–node–metastasis (TNM) staging system that was developed and maintained by the Union for International Cancer Control/American Joint Committee on Cancer (UICC/AJCC). 17 Cirrhosis was diagnosed by histological examination or clinical findings of portal hypertension. Viral hepatitis includes hepatitis B virus (HBV) and hepatitis C virus (HCV) infected subjects, according to the measurement results for these viruses. Metastatic hepatic carcinoma was determined using TNM staging system in patients with documented cancer diagnosis in their medical histories. Benign liver diseases include alcohol or drug induced liver injury, fat liver, and hepatic hemangioma. For healthy volunteers, they were enrolled from those of healthy voluntary donation.
Samples were excluded if they met one of the following criteria: (1) Source patients received warfarin or vitamin K within 1 month, (2) samples are contaminated or with precipitants or floccules, (3) samples are not enough for testing. All the samples were stored at −80°C before testing.
Measurement of PIVKA-II and AFP
Samples were collected before the treatment for HCC groups. Concentrations of PIVKA-II and AFP in serum samples were determined by both chemiluminescent enzyme immunoassay (CLEIA) on LUMIPULSE® G1200 (Fujirebio Diagnostics, Fujirebio, Japan) platform and chemiluminescent microparticle immunoassay (CMIA) on ARCHITECT® i2000 (Abbott Diagnostics, Abbott, USA) platform, according to manufacturer’s instructions. The cutoff values for PIVKA-II and AFP are defined as 40 mAU/mL and 20 ng/mL, respectively.10,12
Statistical analysis
All the statistical analyses were performed using SPSS statistics 22 software (IBM, USA) and MedCalc software version 12.2.1.0 (MedCalc Software, Belgium). Cutoff values of PIVKA-II and AFP are 20 ng/mL and 40 mAU/mL, respectively. The samples with either AFP ⩾ 20 ng/mL or PIVKA-II ⩾ 40 mAU/mL were defined as positives. We used one-way analysis of variance (ANOVA) for continuous variables. To summarize test performance, receiver operating characteristic (ROC) curve was plotted for each biomarker and in combination. Area under the ROC curve (AUC) and its 95% confidence interval (CI) were calculated. AUC Differences between single biomarker and the panel were calculated using logistic regression model. 18
Results
Patient characteristics and biomarker levels
Table 1 shows the demographics of the study population, a total of 382 patients and 200 healthy volunteers were included in this study. Among 132 HCC patients (mean age of 57.5 ± 9.2 years in early stage of HCC and 55.9 ± 9.1 years in late stage of HCC), all were originally diagnosed. The viral hepatitis controls (mean age of 41.3 ± 11.8 years) and healthy controls (mean age of 33.1 ± 8.5 years) were younger than those with other diseases (p < 0.005 and p < 0.000, respectively). A male predominance in all group were found except in other benign liver disease control group. A total of 14 (22.2%) in early stage of HCC group and 41 (59.4%) in late stage of HCC group were HBsAg (surface antigen of the HBV) positive. Besides, 80 (80%) viral hepatitis controls and 28 (56%) cirrhosis patients were induced by HBV infection. The TNM stages of enrolled HCC patients were 27 (20.5%) in stage I, 36 (27.3%) in stage II, 66 (50%) in stage III, and 3 (2.2%) in stage IV.
Characteristics of patients enrolled in this study.
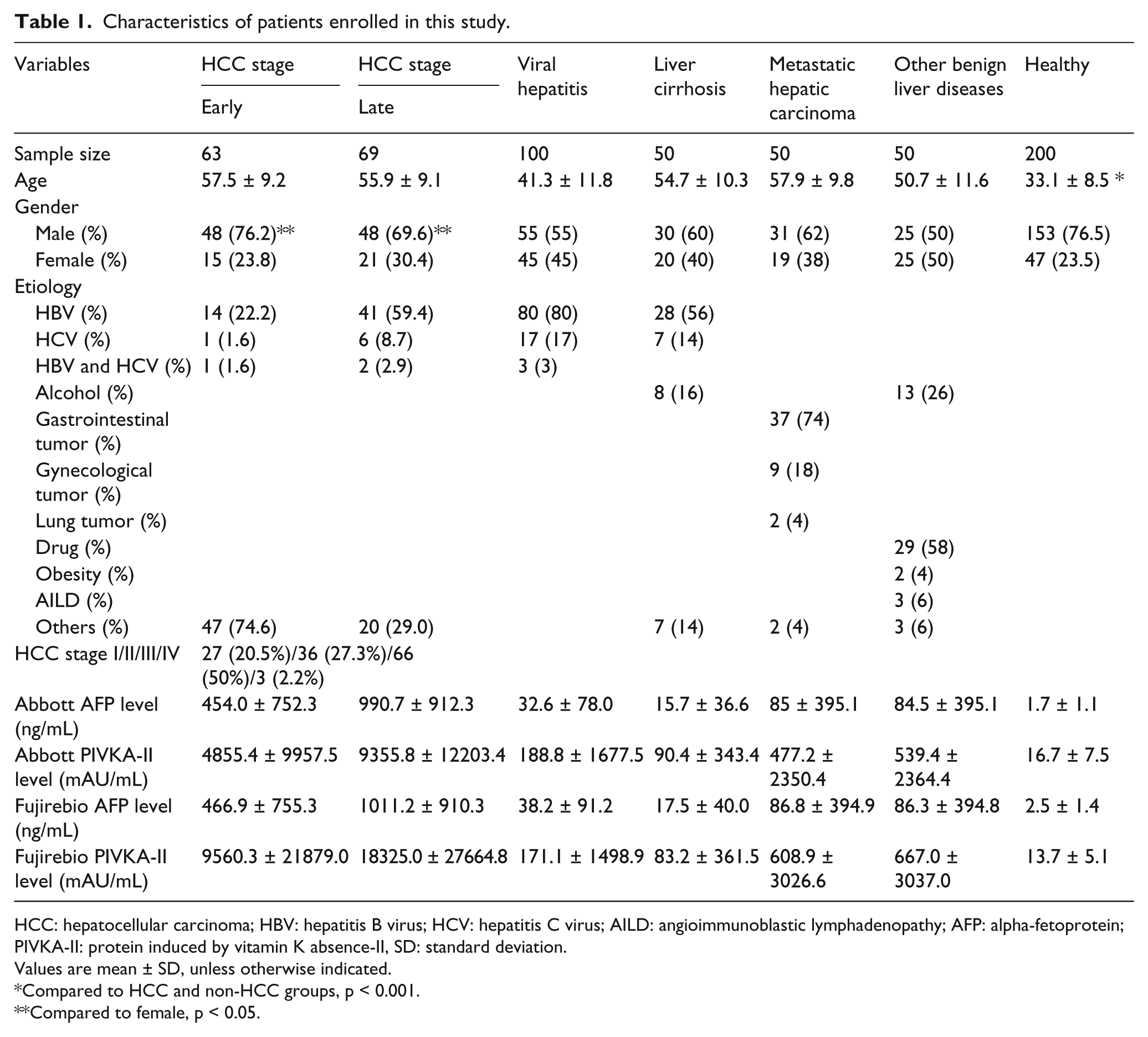
HCC: hepatocellular carcinoma; HBV: hepatitis B virus; HCV: hepatitis C virus; AILD: angioimmunoblastic lymphadenopathy; AFP: alpha-fetoprotein; PIVKA-II: protein induced by vitamin K absence-II, SD: standard deviation.
Values are mean ± SD, unless otherwise indicated.
Compared to HCC and non-HCC groups, p < 0.001.
Compared to female, p < 0.05.
Serum levels of AFP and PIVKA-II are significantly elevated in HCC group especially in late stage of HCC patients compared to non-HCC and healthy controls. Both Abbott and Fujirebio assays show that geometric AFP average value for HCC is higher than non-HCC groups (p < 0.001). Geometric PIVKA-II average level for HCC is higher than non-HCC groups (p < 0.001).
Comparison of AUC, sensitivity, and specificity of the two biomarkers alone and in combination to distinguish HCC from non-HCC patients and healthy controls
As shown in Table 2, Abbott PIVKA-II (40 mAU/mL) has better sensitivity (80%) but decreased specificity (89%) compared to AFP (20 ng/mL). It also has the best overall sensitivity and specificity performances among all four markers.
Diagnostic performances of two biomarkers alone and in combination for HCC diagnosis with control groups.
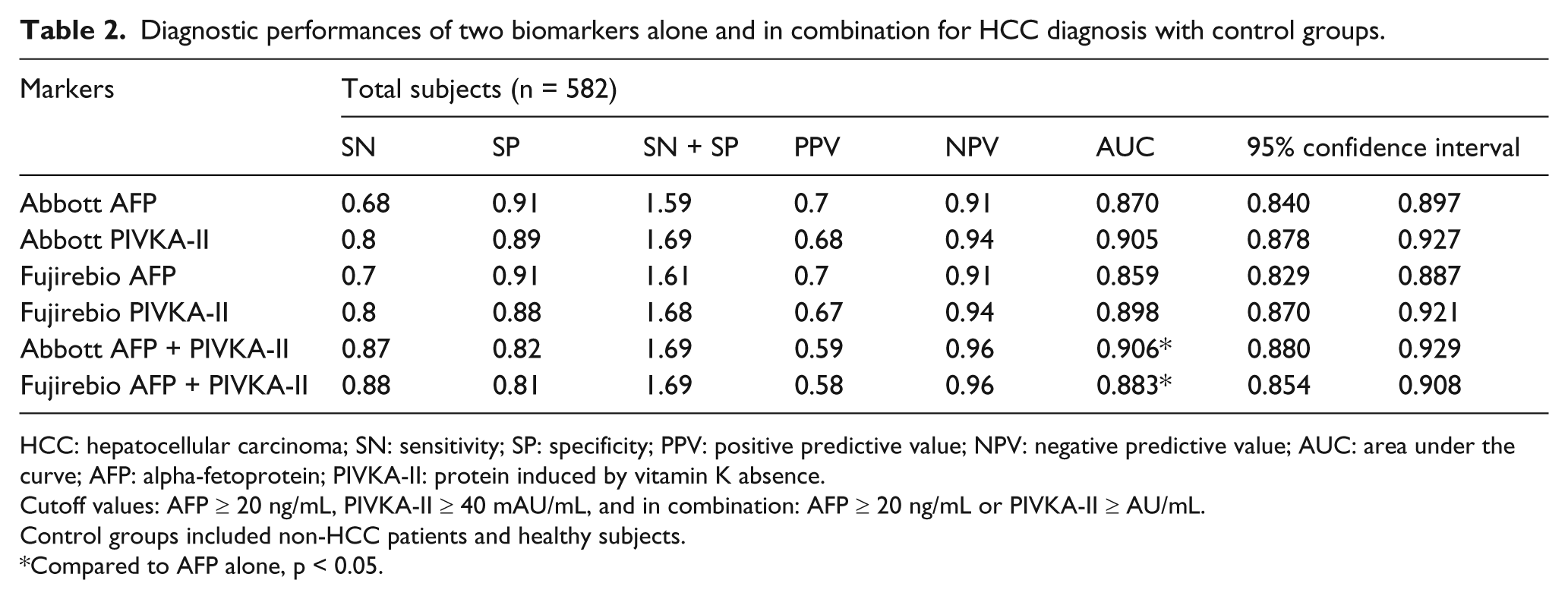
HCC: hepatocellular carcinoma; SN: sensitivity; SP: specificity; PPV: positive predictive value; NPV: negative predictive value; AUC: area under the curve; AFP: alpha-fetoprotein; PIVKA-II: protein induced by vitamin K absence.
Cutoff values: AFP ⩾ 20 ng/mL, PIVKA-II ⩾ 40 mAU/mL, and in combination: AFP ⩾ 20 ng/mL or PIVKA-II ⩾ AU/mL.
Control groups included non-HCC patients and healthy subjects.
Compared to AFP alone, p < 0.05.
Compared to AFP, AFP and PIVKA-II panel shows significantly a better AUC (0.906, 95% CI: 0.880–0.929) for the diagnosis of HCC with sensitivity of 87% and specificity of 82%, using the currently recommended clinical cutoffs for AFP (20 ng/mL) and PIVKA-II (40 mAU/mL). The AUC of Abbott AFP was 0.870 (95% CI: 0.840–0.897), sensitivity was 68%, and specificity was 91%. The AUC for Abbott PIVKA-II was 0.905 (95% CI: 0.878–0.927), sensitivity was 80%, and specificity was 89%. Fuji assays showed the same tendency as Abbott assays that two markers in combination had better performance in HCC diagnosis than AFP alone. No significant difference was found between Abbott and Fujirebio assays.
Comparison of AUC, sensitivity, and specificity of the two biomarkers alone and in combination to distinguish early stage of HCC from non-HCC patients
A total of 63 (47.7%) patients in early stage of HCC (TNM stage I or II) and 250 non-HCC patients were included. As shown in Table 3, single PIVKA-II (Abbott) has sensitivity of 71% with specificity of 80% indicating better sensitivity and slightly decreased specificity compared to AFP. In combination, Abbott PIVKA-II and AFP showed the better AUC of 0.809 (95% CI: 0.761–0.851) compared to AFP alone, the sensitivity for early HCC diagnosis was increased to 83% with specificity of 68%.
Diagnostic performances of two biomarkers alone and in combination for early-stage HCC diagnosis with control groups.
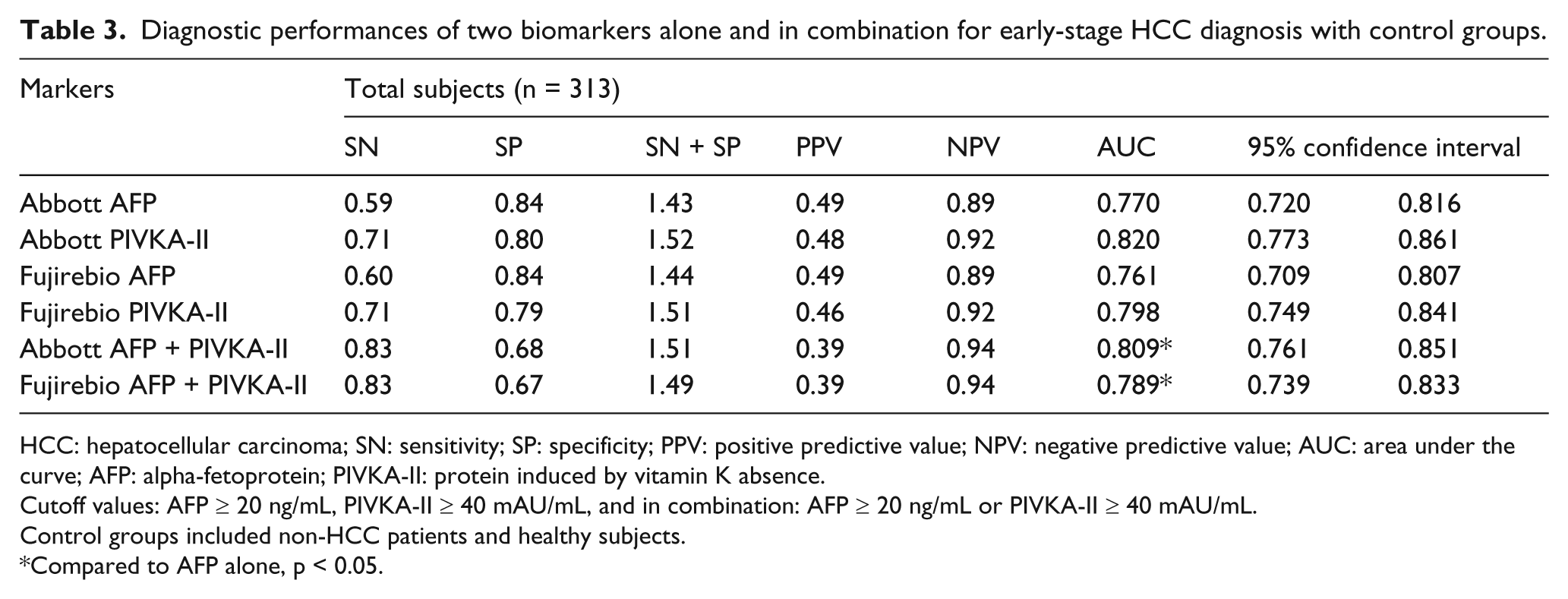
HCC: hepatocellular carcinoma; SN: sensitivity; SP: specificity; PPV: positive predictive value; NPV: negative predictive value; AUC: area under the curve; AFP: alpha-fetoprotein; PIVKA-II: protein induced by vitamin K absence.
Cutoff values: AFP ⩾ 20 ng/mL, PIVKA-II ⩾ 40 mAU/mL, and in combination: AFP ⩾ 20 ng/mL or PIVKA-II ⩾ 40 mAU/mL.
Control groups included non-HCC patients and healthy subjects.
Compared to AFP alone, p < 0.05.
Comparison of AUC, sensitivity, and specificity of the two biomarkers alone and in combination to distinguish HCC from non-HCC patients induced by HBV
We also evaluated the performance of AFP and PIVKA-II in HBsAg-positive patients including 55 HCC patients, 28 cirrhosis patients, and 80 hepatitis patients. As shown in Table 4, Abbott PIVKA-II showed better sensitivity (85%) and specificity (93%) compared to AFP (sensitivity of 73% and specificity of 73%). The AUC of Abbott PIVKA-II is 0.901 (95% CI: 0.845–0.942), which is significantly better than Abbott AFP alone (AUC: 0.788; 95% CI: 0.717–0.848; p < 0.05) and in combination (AUC: 0.851; 95% CI: 0.763–0.884; p < 0.05) as shown in Figure 1(a). The ROC of Fuji also showed the same tendency as Abbott assays that PIVKA-II alone showed the best AUC compared to AFP alone and in combination (Figure 1(b)).
Diagnostic performances of two biomarkers alone and in combination for HBV-related HCC diagnosis with hepatitis and cirrhosis.

HBV: hepatitis B virus; HCC: hepatocellular carcinoma; SN: sensitivity; SP: specificity; PPV: positive predictive value; NPV: negative predictive value; AUC: area under the curve; AFP: alpha-fetoprotein; PIVKA-II: protein induced by vitamin K absence.
Cutoff values: AFP ⩾ 20 ng/mL, PIVKA-II ⩾ 40 mAU/mL, and in combination: AFP ⩾ 20 ng/mL or PIVKA-II ⩾ 40 mAU/mL.
Control groups included HBV-related HCC patients, HBV hepatitis patients, and cirrhosis patients.
Compared to AFP alone, p < 0.05.

ROC curve of AFP, PIVKA-II, and in combination for the diagnosis of HCC with non-HCC patients infected by HBV. (a) ROC of Abbott assays. (b) ROC of Fujirebio assay performance.
Discussion
This control evaluation study demonstrated that panel of PIVKA-II and AFP has better diagnostic value for HCC compared to AFP, even in early stage. PIVKA-II showed better performance in HBV-related HCC patients than AFP.
HCC early detection with imaging diagnosis has been developed in recent years; tumor markers are still commonly used in HCC detection and follow-up visits. AFP has been widely used for HCC diagnosis for many years. However, about 30% of HCC patients have false negative results, especially in early stage.19–22 Other benign liver diseases might also have elevated AFP including patients with cirrhosis or chronic viral hepatitis.9,23 In our study, AFP significantly increased in HCC patients included in early stage. AFP has a sensitivity of 68% and specificity of 91% in diagnosis of HCC, and the sensitivity decreased to 59% in early stage. Our data are consistent with previous publications that showed that AFP has limitations in HCC detection.24,25
It was reported that PIVKA-II has better sensitivity and specificity than AFP.26–28 However, other researchers had different opinions.29,30 The current data of all patients showed that AUC of PIVKA-II for HCC detection was 0.905, which is higher than that of AFP. However, the difference is not significant in this study. If focusing on patients with HBV infection, AUC of PIVKA-II was significantly higher than AFP. PIVKA-II also has better sensitivity and specificity compared to AFP in these patients. The data are consistent with previous publications which reported that PIVKA-II has better performance in patients with viral etiology including HBV or HCV. 10 About 80% of all newly diagnosed HCC were developed from chronic HBV infection in China that was higher than western countries.31,32 In our study, about 41.7% HCC patients had positive HBsAg. Etiology difference should be considered for the contrary PIVKA-II performance compared to AFP in China and in western countries.
In our study, the panel of AFP and PIVKA-II improves sensitivity to 87% in all stages of HCC patients. In HCC early stage, the sensitivity increased to 83%. In addition, the panel showed significantly increased AUC (0.906 in whole patients and 0.809 in HCC early-stage patients) compared to AFP. These results suggested that these two biomarkers in combination should be used with imaging to improve the diagnostic value in HCC patients.
Two platforms were used in our study to validate our results. No significant difference was found between Abbott and Fujirebio assays in HCC detection in all the HCC patients. However, in HCC early-stage detection, Abbott AFP showed better AUC (0.770) compared to Fujirebio AFP (0.761), Abbott PIVKA-II (AUC 0.820) performed better than Fujirebio PIVKA-II (AUC 0.798) in these patients. On combining these two biomarkers, Abbott assay performed better (AUC 0.809).
ROC curve was drawn to compare AFP, PIVKA-II, and in combination diagnosis value in HCC patients with positive HBsAg. The results revealed that PIVKA-II alone has the highest AUC (0.901) compared to AFP alone (0.788) and in combination (0.851). PIVKA-II was expected to play more important role in the setting of HBsAg-positive HCC diagnosis.
Limitation of our study is that the small size of HBsAg-positive HCC early-stage patients (10.6%) was enrolled. Most of HBsAg-positive HCC patients came at late stage. Further studies are needed to investigate the performance of PIVKA-II in large number of early-stage HCC patients with HBV infection, as well as potential future intent to use high-risk populations where the biomarker utilization may aid in early identification of HCC.
In conclusion, we demonstrated that PIVKA-II can be used as effective as AFP in HCC diagnosis, PIVKA-II combined with AFP performed better than AFP alone in HCC diagnosis, especially in early stage. PIVKA-II has better performance than AFP in HBsAg-positive HCC patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Abbott Diagnostics Division.
Open access
This article is distributed under the terms of the Creative Commons Attribution License which permits any use, distribution, and reproduction in any medium, provided the original author(s) and the source are credited.