
Abstract
Hypoxia plays a critical role in the progression and metastasis of hepatocellular carcinoma by activating the key transcription factor, hypoxia-inducible factor-1. This study aims to identify the novel mechanisms underlying the dysregulation of hypoxia-inducible factor-1α in hepatocellular carcinoma. We found that histone deacetylase 5, a highly expressed histone deacetylase in hepatocellular carcinoma, strengthened the migration and invasion of hepatocellular carcinoma cells under hypoxia but not normoxia condition. Furthermore, histone deacetylase 5 induced the transcription of hypoxia-inducible factor-1α by silencing homeodomain-interacting protein kinase-2 expression, which was also dependent on hypoxia. And then knockdown of hypoxia-inducible factor-1α decreased the expressions of mesenchymal markers, N-cadherin, and Vimentin, as well as matrix metalloproteinases, MMP7 and MMP9; however, the epithelial marker, E-cadherin, increased. Phenotype experiments showed that the migration and invasion of hepatocellular carcinoma cells were impaired by knockdown of histone deacetylase 5 or hypoxia-inducible factor-1α but rescued when eliminating homeodomain-interacting protein kinase-2 in hepatocellular carcinoma cells, which suggested the critical role of histone deacetylase 5–homeodomain-interacting protein kinase-2–hypoxia-inducible factor-1α pathway in hypoxia-induced metastasis. Finally, clinical analysis confirmed the positive correlation between histone deacetylase 5 and hypoxia-inducible factor-1α in hepatocellular carcinoma specimens and a relatively poor prognosis for the patients with high levels of histone deacetylase 5 and hypoxia-inducible factor-1α. Taken together, our findings demonstrated a novel mechanism underlying the crosstalk between histone deacetylase 5 and hypoxia-inducible factor-1 in hepatocellular carcinoma.
Keywords
Introduction
Hepatocellular carcinoma (HCC) is one of the most malignant cancers, which has a high fatality rate. 1 Although various improved therapies have been applied in diagnosis and treatment of patients with HCC, a poor prognosis is commonly observed after treatment. 2 The high incidence of metastasis after hepatic resection is one of the main causes which result in the decrease in overall 5-year survival rate, 3 and epithelial–mesenchymal transition (EMT) with acquired migratory and invasive capabilities plays a crucial role in the process.
As epigenetic regulator, histone deacetylase (HDAC) is indispensable during activation of gene transcription in physiological condition and is also involved in tumor genesis and development. Previous works demonstrated that HDACs were overexpressed in many cancers and then conferred malignant phenotypes through activating oncogenes or inhibiting specific tumor suppressor genes.4,5 HDAC5, one of Class II HDACs, was reported to result in the dysregulation of cell proliferation and apoptosis in different cancers including HCC, and ectopic high expression of HDAC5 was also observed in liver cancer tissues. 6 However, the role of HDAC5 in migration and invasion of HCC remains unknown.
Hypoxia, a common characteristic of solid tumors, facilitates tumor metastasis by increasing migration and invasion. 7 Hypoxia-inducible factor-1 (HIF1), composed of two subunits: HIF1α and HIF1β, functions as a key transcription factor in response to hypoxia. 8 As an oxygen-regulated protein, HIF1α determines the activity of HIF1 transcription complex and is aberrantly expressed in a variety of solid tumors, including HCC. 9 Previous studies indicated that the increased protein stability and nucleus-translocation of HIF1α promoted the transcription of downstream oncogene which contained a hypoxia-responsive element (HRE), thereby regulating tumor metabolism, proliferation, and metastasis.10,11
Although the abnormal expression or activity of HIF1α was described in many solid tumors, the regulatory mechanisms for HIF1α in different cancer types have not been well elucidated. It has been reported that inhibition of HDAC activity triggers HIF1α degradation and represses HIF1 function.12,13 Further studies showed that HDAC5 increased the transactivation function of HIF1α by promoting dissociation of HIF1α from factor inhibiting HIF-1 (FIH-1) and association with p300. 14 In addition, HDAC5 could also facilitate the hypoxia-induced stabilization and nuclear accumulation of HIF1α. 15
Here, we found a novel mechanism for transcriptional regulation of HIF1α in response to hypoxia. Briefly, HDAC5 induces the transcription of HIF1α by blocking homeodomain-interacting protein kinase-2 (HIPK2) expression in hypoxic HCC cells. And then the upregulated HIF1α leads to the EMT of HCC cells, as is reflected in increased migration and invasion. Consistently, clinical analysis indicates a positive correlation between HDAC5 and HIF1α in HCC specimens and a poor prognosis of HCC patients with high expressions of HDAC5 and HIF1α. Therefore, our findings suggest that the HDAC5–HIPK2–HIF1α axis plays a crucial role in hypoxia-induced aggressiveness of HCC by activating HIF1α transcription.
Materials and methods
Cell culture and transfection
Human HCC cell lines, Hep3B, Huh7, and HepG2 were purchased from Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences (Shanghai, China). The control liver cell line, THLE-3, was purchased from American Type Culture Collection (ATCC, Manassas, VA, USA). All the cells were cultured in RPMI 1640 medium containing 10% fetal calf serum, 100 units/mL penicillin, and 100 µg/mL streptomycin in 5% CO2, 95% air at 37°C. For hypoxia experiments, cells were incubated in 1% O2, 5% CO2, and 94% N2. Transfection of plasmids and small interfering RNAs (siRNAs) was performed with X-tremeGENE HP DNA Transfection Reagent (Roche Applied Science, Mannheim, Germany) according to the manufacturer’s protocol. The stable transfection of HDAC5 short hairpin RNA (shRNA) or overexpression plasmids was maintained by G418 treatment.
Quantitative real-time reverse transcription polymerase chain reaction
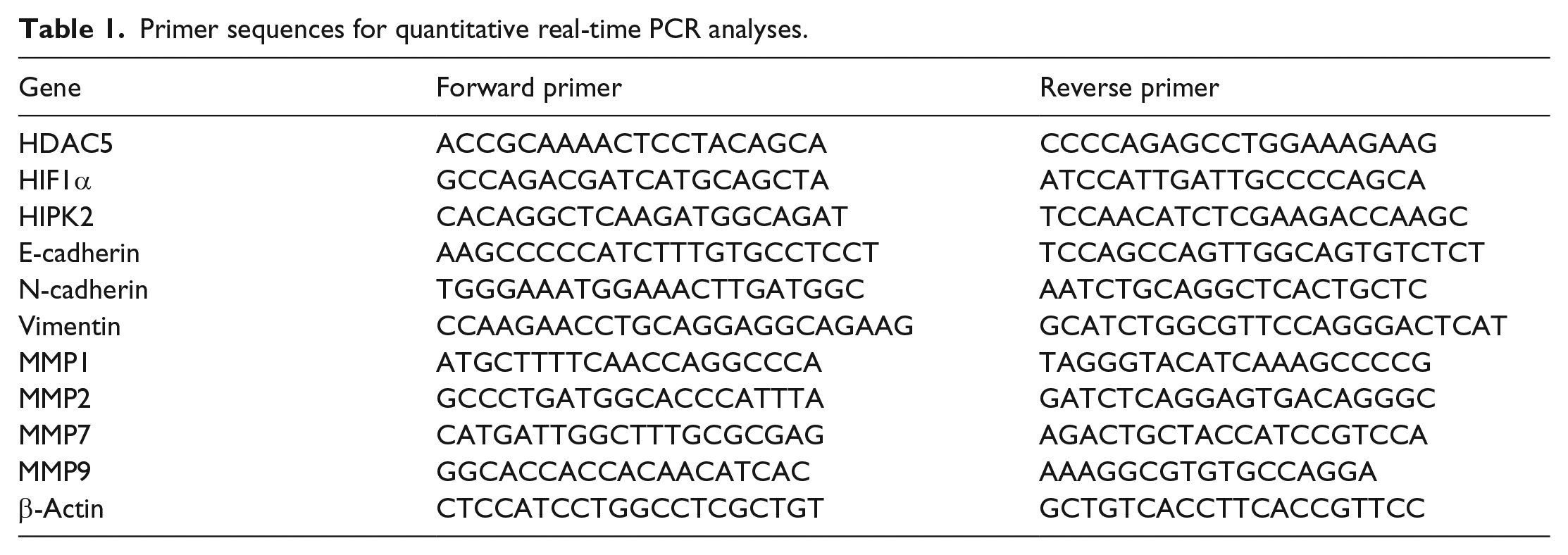
Reverse transcription polymerase chain reaction (RT-PCR) was carried out according to a previous study. 16 Total RNA was extracted using the RNAiso™ Plus reagent (Takara, Otsu, Japan) and reverse-transcribed using a PrimeScript™ RT reagent kit (Takara). Quantitative PCR (qPCR) was implemented with SYBR Green Mix (Takara) according to the manufacturer’s instructions. β-Actin served as loading control. The primer information is listed in Table 1.
Primer sequences for quantitative real-time PCR analyses.
Western blot
Western blot was performed according to a previous study. 16 The whole cell lysate was examined using the antibodies mouse anti-human HDAC5 (sc-133225; Santa Cruz Biotechnology, Santa Cruz, CA, USA), mouse anti-human HIF1α (ab16066; Abcam, Cambridge, UK), mouse anti-human HIPK2 (sc-100383; Santa), rabbit anti-human E-cadherin (sc-7870), rabbit anti-human N-cadherin (sc-7939), mouse anti-human Vimentin (sc-6260; Santa), rabbit anti-human MMP7 (ab38996; Abcam), and rabbit anti-human MMP9 (ab137651; Abcam). IRDye® 800CW- or IRDye 680–conjugated secondary antibodies (LI-COR Biosciences, Lincoln, NE, USA) were used for staining and then detected by an Odyssey® infrared imaging system (LI-COR).
Reporter gene assay
The promoter sequences (−2100/+25) of the human HIF1α gene were amplified by PCR and inserted into the pGL3-Basic Luciferase Reporter Vectors (Promega, Madison, WI, USA). Cells were plated onto 24-well plates the day before transfection. The cells were co-transfected with 0.5 µg of firefly luciferase reporter constructs, 0.02 µg of pRL-TK Renilla luciferase reporter plasmids (Promega), and HDAC5 expression plasmids using the X-tremeGENE HP DNA Transfection Reagent. The luciferase activity was measured by a Dual-Luciferase Reporter Assay System (Promega).
Chromatin immunoprecipitation
Chromatin immunoprecipitation (ChIP) was performed according to a previous study. 17 Chromatin was crosslinked using 1% formaldehyde for 10 min and sonicated to obtain DNA fragments of 200–500 bp. After centrifugation, the supernatants were subjected to immunoprecipitation overnight at 4°C with antibodies against HDAC5 (sc-133225; Santa), HIPK2 (sc-100383; Santa), H3K9ac (ab4441; Abcam), or normal rabbit IgG. Protein A/G PLUS-Agarose (sc-2003; Santa) was used to isolate the chromatin–antibody complexes. The crosslinking was reversed, and the precipitated DNA fragments were purified and analyzed by qPCR.
Wound healing assay
HCC cells were seeded in six-well plates. After transfection for 24 h, the monolayer was gently scratched with a pipette tip and then washed with phosphate-buffered saline (PBS) to remove detached cells. The well was re-loaded with serum-free medium, and cells were cultured for additional 48 h, when images of scratched monolayer were captured on a microscope. The wound was evaluated using ImageJ.
Transwell assays
The transwell assays were carried out according to a previous study. 16 The invasive capability of HCC cells was evaluated in Boyden chambers with Matrigel according to the manufacturer’s protocol (Invitrogen, Carlsbad, CA, USA). The 8-mm-porosity polycarbonate membrane was covered with 200 mL of serum-free medium containing 1 × 105 cells per well. The plates were then incubated with 10% fetal bovine serum (FBS) medium for 48 h at 37°C in a 5% CO2 incubator. The invasion cells on the bottom surface of the filter were fixed, stained, and counted using optical microscopy.
Immunofluorescence
According to a previous study, 17 Hep3B monolayer on glass coverslips was fixed for 15 min using 4% paraformaldehyde, permeabilized for 20 min in PBS containing 0.2% Triton X-100, and then blocked for 2 h with PBS containing 1% BSA and 0.5% goat serum at 37°C. The cells were incubated with primary antibody at 4°C overnight. The antibodies rabbit anti-human E-cadherin (sc-7870) and rabbit anti-human N-cadherin (sc-7939) were purchased from Santa Cruz Biotechnology. After rinsing with PBS, they were probed with fluorescein isothiocyanate (FITC)- or tetramethylrhodamine-5-(and 6)-isothiocyanate (TRITC)–conjugated secondary antibodies (Santa) for 1 h at 37°C. The nuclei were stained with 4′,6-diamidino-2-phenylindole (DAPI; Sigma, St Louis, MO, USA) for 15 min. The slides were mounted and visualized by a fluorescence microscope (AX70; Olympus, Tokyo, Japan).
ELISA
Conditioned media were collected 24 h after cell treatment and centrifuged to remove any detached cells. Enzyme-linked immunosorbent assays (ELISAs) were carried out using Human Quantikine ELISA kit (R&D Systems, Minneapolis, MN, USA) according to the manufacturer’s instructions.
Immunohistochemistry
A total of 164 human HCC samples were collected at the Sanmen People’s Hospital after informed consent had been given by all patients. The immunohistochemistry was performed using an EnVision Detection System (DAKO, Carpinteria, CA, USA) according to the manufacturer’s instructions. To estimate the score for each slide, at least 10 individual fields at 100× were chosen, and 100 cancer cells were counted in each field. The antibodies for HDAC5 (1:200 dilutions) IHC staining were purchased from Santa Cruz Biotechnology (sc-133225) and HIF1α (1:100 dilutions) were purchased from Abcam (ab16066). The immunostaining intensity was divided into four grades: 0, negative; 1, weak; 2, moderate; and 3, strong. The proportion of positive staining cells was divided into five grades: 0, <5%; 1, 6%–25%; 2, 26%–50%; 3, 51%–75%; and 4, >75%. The staining results were evaluated and confirmed by two independent investigators blinded to the clinical data. The percentage of positivity of the tumor cells and the staining intensities were then multiplied to generate the IHC score and graded as low expression (score 0–6) and high expression (score 7–12). Cases with a discrepancy in scores were discussed to obtain a consensus.
Statistics
A database was created and transferred to SPSS 22.0 for Windows. Statistical data analysis was performed using the two-tailed Student’s t-test and analysis of variance (ANOVA), and the results are presented as the mean ± standard deviation (SD) of three separate experiments. A value of p <0.05 was considered statistically significant. Spearman test was used in analyzing the correlation.
Results
Stable knockdown of HDAC5 impairs the migratory and invasive capabilities of HCC cells under hypoxia condition, as well as hypoxia-induced EMT
The messenger RNA (mRNA) and protein levels of HDAC5 in a normal liver cell line and several HCC cell lines were examined, and the results showed higher expressions of HDAC5 on both mRNA and protein level in HCC cells compared with normal liver cells (Figure 1(a) and (b)). Then Hep3B cells with stable knockdown of HDAC5 were constructed (Figure 1(c)) and studied for migration and invasion. Interestingly, under normoxia condition, knockdown of HDAC5 had no effect on migration and invasion; however, weakened abilities of migration and invasion were observed after stable knockdown of HDAC5 under hypoxia condition (Figure 1(d) and (e)). So the above evidences suggested a crucial role of HDAC5 in HCC metastasis under hypoxia. In hypoxia state, deprivation of HDAC5 significantly increased the epithelial marker, E-cadherin, but decreased the mesenchymal markers, N-cadherin and Vimentin, which indicated a main feature of EMT (Figure 1(f) and (g)). In addition, the expressions of matrix metalloproteinases, MMP7 and MMP9, were suppressed by HDAC5 knockdown only under hypoxia condition (Figure 2(h) and (i)). These findings demonstrate that HDAC5 is indispensable for hypoxia-induced EMT of HCC.

Stable knockdown of HDAC5 impairs the migratory and invasive capabilities of HCC cells under hypoxia condition, as well as hypoxia-induced EMT. The (a) mRNA or (b) protein levels of HDAC5 were analyzed by qRT-PCR or western blot in the indicated cell lines. Three independent experiments were performed for quantitative analysis in (b). *p < 0.05. (c) Hep3B cells with stable knockdown of HDAC5 were constructed and verified by western blot. (d) Scratch assays with shHDAC5-Hep3B and shCtrl-Hep3B cells under normoxia (21% O2) or hypoxia (1% O2) condition. Scale bar: 200 µm. Percentage wound closure from three independent experiments was analyzed. *p < 0.05. (e) Transwell assays with shHDAC5-Hep3B and shCtrl-Hep3B cells under normoxia or hypoxia condition. Scale bar: 200 µm Numbers of invasive cells from three independent experiments were analyzed. *p < 0.05. The (f) mRNA or (g) protein levels of E-cadherin, N-cadherin, and Vimentin were analyzed by qRT-PCR or western blot in shHDAC5-Hep3B and shCtrl-Hep3B cells under normoxia or hypoxia condition. *p < 0.05. The (h) mRNA levels of MMPs and (i) protein levels of MMP7 and MMP9 were analyzed by qRT-PCR or western blot in shHDAC5-Hep3B and shCtrl-Hep3B cells under normoxia or hypoxia condition. *p < 0.05.

HDAC5 promotes the transcription of HIF1α under hypoxia condition. The (a) mRNA or (b) protein levels of HIF1α were analyzed by qRT-PCR or western blot in shHDAC5-Hep3B and shCtrl-Hep3B cells under normoxia or hypoxia condition. *p < 0.05. The mRNA levels of VEGF served as a positive control. (c) Huh7 cells with stable overexpression of HDAC5 were constructed and verified by western blot. The (d) mRNA or (e) protein levels of HIF1α were analyzed by qRT-PCR or western blot in HDAC5-Huh7 and EV-Huh7 cells under normoxia or hypoxia condition. *p < 0.05. The mRNA levels of VEGF served as a positive control. The (f) mRNA or (g) protein levels of HIF1α were analyzed by qRT-PCR or western blot in HDAC5-Huh7 and EV-Huh7 cells after 1 µg/ml ActD treatment under hypoxia. Three independent experiments were performed for quantitative analysis in G. *p < 0.05. (h) Relative luciferase activity in Huh7 cells co-transfected with different amounts of HDAC5 expression plasmid, HIF1α promoter reporter (−2100/+25), and an internal control reporter pRL-TK. *p < 0.05. (i) Relative luciferase activity in shCtrl/shHDAC5-Hep3B cells co-transfected with HIF1α promoter reporter (−2100/+25) and an internal control reporter pRL-TK. *p < 0.05.
HDAC5 promotes the transcription of HIF1α under hypoxia condition
To further understand the hypoxia-dependent function of HDAC5, we studied the relationship between HDAC5 and HIF1α, a key transcription factor in response to hypoxia, in HCC cells. Silence of HDAC5 by stable knockdown inhibited the hypoxia-induced expression of HIF1α on both mRNA and protein level. However, no significant alternation of HIF1α expression was observed after HDAC5 knockdown under normoxia condition (Figure 2(a) and (b)). Then Huh7 cells with stable overexpression of HDAC5 were constructed (Figure 2(c)). Consistently, ectopic expression of HDAC5 failed to change the level of HIF1α under normoxia but increased the HIF1α expression which was induced by hypoxia (Figure 2(d) and (e)). To explore the mechanism for the upregulation of HIF1α by HDAC5, a transcription inhibitor, actinomycin D (ActD), was used to determine the necessity of HDAC5-induced HIF1α transcription in the accumulation of HIF1α under hypoxia. As shown in Figure 2(f) and (g), the upregulation of HIF1α mRNA, which was induced by HDAC5 overexpression, was completely abolished after ActD treatment, while the increased HIF1α protein by HDAC5 was evidently attenuated after ActD addition. Under hypoxia, ectopic expression of HDAC5 increased the transcription activity of HIF1α promoter (Figure 2(h)) while knockdown of HDAC5 repressed HIF1α transcription (Figure 2(i)). These data suggest that the transcription of HIF1α is promoted by HDAC5 in response to hypoxia.
HDAC5 induces the transcription of HIF1α through silencing the tumor suppressor HIPK2 by histone modification
To explore the regulatory mechanism for HIF1α by HDAC5, ChIP assays were performed to verify whether HDAC5 directly activated the transcription of HIF1α in response to hypoxia. It was found that hypoxia had no influence on the binding of HDAC5 to the HIF1α promoter but significantly increased the level of H3K9ac, an active histone modification, at the HIF1α promoter (Figure 3(a) and (b)). In consideration of a well-known function of HDAC5 as a transcriptional co-repressor by histone acetylation, indirect regulation for HIF1α transcription is probable. In previous studies, HIPK2 which belongs to a family of co-repressors for homeodomain transcription factors was found to repress the transcription of HIF1α, 18 and HIPK2 degradation induced by hypoxia was associated with chemoresistance in hepatoma cells. 19 In this work, we noticed that HIPK2 mRNA and protein levels significantly increased after knockdown of HDAC5 only under hypoxia condition (Figure 3(c) and (d)). Consistently, hypoxia was required for the reduced HIPK2 expression by overexpressed HDAC5 (Figure 3(e) and (f)). To identify HDAC5 potentially involved in HIPK2 transcriptional repression, ChIP assays were carried out in hypoxic hepatoma cells. As shown in Figure 3(g), HDAC5 was efficiently recruited onto HIPK2 promoter in the HCC cells with hypoxia but not with normoxia, which was abrogated by knockdown of HDAC5. Consistently, HDAC5 knockdown resulted in a higher relative enrichment of active histone modification H3K9ac at the HIPK2 promoter in hypoxic HCC cells; however, no significant alteration of H3K9ac level was found under normoxia (Figure 3(h)). Consequently, the increased HIPK2 proteins after HDAC5 knockdown were bound to HIF1α promoter (Figure 3(i)). In an attempt to investigate whether the induction of HIF1α by hypoxia arose from HDAC5-mediated epigenetic silence of HIPK2, the Hep3B cells with stable knockdown of HDAC5 were transfected with HIPK2 siRNA. The results showed that the reduction in HIF1α by HDAC5 knockdown was partly reversed in hypoxic Hep3B cells after deprivation of HIPK2 (Figure 3(j) and (k)). The above findings suggest that HDAC5 increases the transcription of HIF1α by inhibiting HIPK2, a transcription repressor of HIF1α.

HDAC5 induces the transcription of HIF1α through silencing the tumor suppressor HIPK2 by histone modification. (a) Chromatin prepared from Hep3B cells with normoxia (21% O2) or hypoxia (1% O2) was immunoprecipitated with HDAC5 antibody; qPCR was performed on immunoprecipitated DNAs or soluble chromatin using specific primer pairs for the HIF1α promoter. *p < 0.05. (b) In the same cells with (a), H3K9ac antibody was used for ChIP, followed by qPCR with specific primer pairs for the HIF1α promoter. *p < 0.05. The (c) mRNA or (d) protein levels of HIPK2 were analyzed by qRT-PCR or western blot in shHDAC5-Hep3B and shCtrl-Hep3B cells under normoxia or hypoxia condition. *p < 0.05. The (e) mRNA or (f) protein levels of HIPK2 were analyzed by qRT-PCR or western blot in HDAC5-Huh7 and EV-Huh7 cells under normoxia or hypoxia condition. *p < 0.05. (g) Chromatin prepared from shHDAC5-Hep3B and shCtrl-Hep3B cells was immunoprecipitated with HDAC5 antibody; qPCR was performed on immunoprecipitated DNAs or soluble chromatin using specific primer pairs for the HIPK2 promoter. *p < 0.05. (h) In the same cells with (g), H3K9ac antibody was used for ChIP, followed by qPCR with specific primer pairs for the HIPK2 promoter. *p < 0.05. (i) In the same cells with (g), HIPK2 antibody was used for ChIP, followed by qPCR with specific primer pairs for the HIF1αpromoter. *p < 0.05. The (j) mRNA or (k) protein levels of HIF1α were analyzed by qRT-PCR or western blot in shCtrl/shHDAC5-Hep3B cells with siHIPK2 transfection under hypoxia condition. *p < 0.05.
HIF1α drives the EMT induced by HDAC5 in HCC cells under hypoxia condition
Considering the effect of HDAC5 knockdown on the phenotypes of HCC cells under hypoxia (Figure 1), we examined the levels of EMT markers and MMPs after knocking down HIF1α. As expected, silencing HIF1α by siRNA induced E-cadherin but reduced N-cadherin, Vimentin, MMP7, and MMP9 on both mRNA and protein levels in hypoxic HCC cells (Figure 4(a) and (b)). Furthermore, immunofluorescence confirmed the attenuated EMT of HCC cells with HIF1α knockdown by detecting E/N-cadherin (Figure 4(c)). ELISAs showed that the levels of secreted MMP7 and MMP9 were reduced by silencing HIF1α in hypoxia-treated HCC cells (Figure 4(d)). To verify whether HIF1α mediates the promotive effect of HDAC5 on hypoxia-induced EMT of HCC, Huh7 cells with stable overexpression of HDAC5 were transfected with siRNA targeting HIF1α. Overexpression of HDAC5 decreased E-cadherin but increased N-cadherin, Vimentin, MMP7, and MMP9, while knockdown of HIF1α abrogated the effect of HDAC5 overexpression (Figure 4(e)–(g)), which indicated that HIF1α may function as a potent downstream effector of HDAC5 to drive hypoxia-induced EMT of HCC cells.

HIF1α drives the EMT induced by HDAC5 in HCC cells under hypoxia condition. Hep3B cells were transfected with HIF1α siRNA under hypoxia. The expressions of indicated EMT markers and MMPs were analyzed by (a) qRT-PCR and (b) western blot. *p < 0.05. The expressions of E-cadherin and N-cadherin were shown by immunofluorescence (c). Scale bar: 20 µm. The relative levels of secreted MMP7 and MMP9 were measured by ELISA (d). *p < 0.05. HDAC5-Huh7 and EV-Huh7 cells were transfected with HIF1α siRNA under hypoxia. The mRNA levels of indicated EMT markers were analyzed by (e) qRT-PCR. *p < 0.05. The protein levels of indicated EMT markers and MMPs were analyzed by (g) western blot. The relative levels of secreted MMP7 and MMP9 were measured by (g) ELISA. *p < 0.05.
HDAC5–HIPK2–HIF1α pathway may contribute to the acquired migration and invasion of HCC cells by hypoxia
Phenotype experiments showed that overexpression of HDAC5 stimulated the migration and invasion of Huh7 cells under hypoxia, and knockdown of HIF1α by siRNA reduced the aggressive phenotypes induced by hypoxia (Figure 5(a)–(d)). Notably, HDAC5 overexpression was not able to restore the decreased migration and invasion of Huh7 cells with knockdown of HIF1α (Figure 5(a)–(d)). As expected, silence of HIPK2 rescued the migratory and invasive capacities in HCC cells with stable knockdown of HDAC5, which suggested the function of HIPK2 as a mediator in HDAC5 downstream pathway (Figure 5(e) and (f)). Therefore, based on previous studies and our findings, we hypothesize a critical role of HDAC5–HIPK2–HIF1α pathway in hypoxia-induced migration and invasion of HCC cells.

HDAC5–HIPK2–HIF1α pathway may contribute to the acquired migration and invasion of HCC cells by hypoxia. HDAC5-Huh7 and EV-Huh7 cells were transfected with HIF1α siRNA under normoxia or hypoxia condition. (a) Scratch and (c) transwell assays were carried out in the treated Huh7 cells. (b) Percentage wound closure and (d) numbers of invasive cells from three independent experiments were analyzed. Scale bar: 200 µm. *, #p < 0.05. shCtrl/shHDAC5-Hep3B cells were transfected with HIPK2 siRNA under hypoxia condition. (e) Scratch and transwell assays were carried out in the treated Hep3B cells. (f) Percentage wound closure and numbers of invasive cells from three independent experiments were analyzed. Scale bar: 200 µm. *, #p < 0.05.
Ectopic high expressions of HDAC5 and HIF1α indicate a poor prognosis in HCC patients
To characterize the expressions of HDAC5 and HIF1α in HCC, immunohistochemical analysis of specimens from HCC patients was performed. As shown in Figure 6(a), different levels of HDAC5 and HIF1α were detected in the HCC tissues from different patients. And a positive correlation between HDAC5 and HIF1α was found in HCC specimens (Figure 6(b)). Further analysis indicated that the HDAC5 and HIF1α staining was positively correlated with tumor size, intrahepatic metastasis, and distant metastasis, and HIF1α expression was also positively correlated with tumor–node–metastasis (TNM) stage (p < 0.05; Table 2). By analyzing the prognosis of included HCC patients, it was found that the 5-year overall survival (OS) rate of HDAC5 or HIF1α high-expression group was lower than that of HDAC5 or HIF1α low-expression group (31.76% versus 50.63%, p = 0.0371; 27.63% versus 52.27%, p = 0.0175; Figure 6(c) and (d)), and the OS rate of group with HDAC5 and HIF1α double-high levels was significantly lower than that of group with HDAC5 and HIF1α double-low levels (26.32% versus 56.67%, p < 0.05; Figure 6(e)). Of note was that HCC patients with high levels of HIF1α had a worse prognosis than HIF1α low-expression patients regardless of the HDAC5 expression status (Figure 6(e)). These data support that HDAC5-induced accumulation of HIF1α may contribute to the poor prognosis of HCC.

Ectopic high expressions of HDAC5 and HIF1α indicate a poor prognosis in HCC patients. (a) Representative images of HDAC5 and HIF1α immunostaining in HCC tissues. Scale bar: 500 µm. (b) The correlation of concurrent immunostaining scores of HDAC5 and HIF1α in HCC tissues. (c–e) The survival rate plot of indicated expression groups in HCC.
Correlation of the expression of HDAC5 and HIF1α with clinicopathological features in HCC.

HDAC5: histone deacetylase 5; HIF1: hypoxia-inducible factor-1; AFP: alpha-fetoprotein; TNM: tumor–node–metastasis.
p < 0.05
Discussion
In HCC, HDAC5 is upregulated in cancer cells compared to normal tissue and indicates a reduced patient survival.6,20 Furthermore, upregulation of HDAC5 mRNA was found significantly correlated with DNA copy number gains in HCC. 20 Previous studies demonstrated that knockdown of HDAC5 by shRNA or specific inhibitor evidently suppressed the proliferation and tumorigenicity of HCC cells through reducing the expressions of cell cycle–related proteins such as cyclin-dependent kinase (CDK)2/4/6 and cyclin D1 but promoted apoptosis via inducing apoptosis-related proteins such as p53, bcl-2, bax, cyto C, and caspases 3.6,21 Besides, HDAC5 was reported to boost HCC cell proliferation through upregulation of Six1 which could activate cyclin A1.22,23 In this study, we noticed that deprivation of HDAC5 impaired the hypoxia-induced migration and invasion of HCC cells; however, no obvious effect of HDAC5 knockdown was observed under normoxia. Meanwhile, HDAC5 overexpression enhanced the malignant phenotypes under hypoxia but not normoxia. To further verify the phenomenon, we examined the levels of several EMT biomarkers and MMPs. As expected, HDAC5 accelerated the hypoxia-induced EMT of HCC cells but failed to induce EMT under normoxia. Therefore, based on the above findings, we hypothesized that HDAC5 may promote the metastasis of HCC especially under hypoxia condition.
Next, to explore the molecular mechanism for the hypoxia-dependent role of HDAC5, we focused on a crucial transcription factor, HIF1. Rapid growth of liver cancer usually causes necrosis and hypoxia which lead to high HIF1α expression and eventually metastasis. Although oxygen-dependent degradation of HIF1α has been well illustrated as the mechanism underlying hypoxia-induced accumulation of HIF1α, 24 other regulatory pathways may also play a pivotal role in regulating the synthesis and activity of HIF1α. As reported, the epidermal growth factor (EGF)/phosphatidylinositol 3-kinase (PI3K)/PTEN/AKT/FRAP pathway upregulated the expression of HIF1α in human prostate cancer cells. 25 Moreover, previous studies demonstrated that HDAC5 facilitated the nuclear accumulation and transcriptional function of HIF1α.14,15 However, we observed that HDAC5 was necessary for the transcription of HIF1α under hypoxia and then conducive to maintaining the protein level of HIF1α in HCC cells. Further investigations showed that the recruitment of HDAC5 onto the HIF1α promoter was not affected by hypoxia, but the level of H3K9ac was upregulated. Considering the contribution of HDACs to tumor development by reversing chromatin acetylation and altering the transcription of numerous tumor suppressor genes, the transcription of HIF1α may be indirectly regulated by HDAC5. Strong evidences indicated that HIPK2 displayed as a co-suppressor of HIF1α and was degraded in hypoxic response.18,19 In this study, we found that hypoxia strengthened the interaction between HDAC5 and HIPK2 promoter. And then HDAC5 blocked the transcription of HIPK2 by histone deacetylation, which resulted in the accumulation of HIF1α. Notably, it was reported that a co-repressor complex between HIPK2 and HDAC1 leads to histone deacetylation and gene silence. 26 Therefore, hypoxia-induced reduction in HIPK2 may increase the H3K9ac level at HIF1α promoter, which is consistent with our observations. However, even though a slight increase in HDAC5 was observed after hypoxia treatment, it still could not explain why the recruitment of HDAC5 onto the promoter of HIPK2 was strongly enhanced in response to hypoxia. So the mechanisms for hypoxia-induced binding of HDAC5 to HIPK2 promoter should be deeply investigated in the future.
Since the transcriptional complex of HIF1 was found, numerous HIF1 target genes have been identified to be involved in angiogenesis, glucose metabolism, survival, invasion, and metastasis.27,28 During tumor development, HIF1 induces various cytokines, such as vascular endothelial growth factor (VEGF), insulin-like growth factor (IGF)-2, transforming growth factor alpha (TGF-α), and interleukin-6/8, which stimulate angiogenesis, proliferation, and invasion.29–32 Besides, under hypoxia condition, HIF1α was found to enhance the transcription of multi-drug resistance (MDR)–related genes in HepG2 cells, conferring chemoresistance. 33 In this study, our findings revealed that HIF1α conferred the role of HDAC5 in accelerating the EMT of HCC cells, as shown by increased N-cadherin and Vimentin but reduced E-cadherin. In addition, HDAC5 upregulated the levels of MM7 and MMP9 by HIF1α. Thus, the downstream effectors activated by HIF1α allow tumor cells to successfully spread during HCC metastasis.
By phenotype experiments, we demonstrated that HDAC5–HIPK2–HIF1α pathway promotes HCC cells’ migration and invasion, especially under hypoxia. However, we noticed that attenuation of HIPK2 by siRNA only partly rescued the migration and invasion disrupted by HDAC5 knockdown, which suggested that multiple pathways may be involved in the regulation of HIF1α by HDAC5. This is in line with evidence from the HIF1α expression. As described in previous studies, cytosolic deacetylase activity of HDAC5 was necessary for HIF1α stabilization and HDAC5 knockdown resulted in proteasome-dependent HIF1a degradation. 15
Taken together, our molecular and clinical evidences suggested a crosstalk between HDACs and hypoxia in promoting HCC metastasis (Figure 7). In HCC, hypoxia environment enhances the repression of HIPK2 by HDAC5 and thus activates the transcription of HIF1α. Meanwhile, increased stability of HIF1α accompanied with HIPK2 degradation contributes to a rapid accumulation of HIF1α in response to hypoxia. As a consequence, augmented HIF1α drives the EMT of HCC cells and also promotes angiogenesis, which facilitates the metastasis of HCC. Still, the mechanism behind dysregulated HIF1α in HCC has not been clearly described in this study. Further investigations of the relationship between HDACs and hypoxia may provide new strategies for HCC therapy.

Schema indicating the HDAC5–HIPK2–HIFα axis as an EMT driver in response to hypoxia. Under hypoxia condition, HDAC5 is recruited onto the promoter of HIPK2 and then inhibits the transcription by deacylation. After that, silence of HIPK2 relieves the transcriptional inhibition of HIF1α. At the same time, hypoxia and HDAC5-dependent stability of HIF1α accompanied with hypoxia-induced HIPK2 degradation facilitates the accumulation of HIF1α. As a result, upregulated HIF1α contributes to HCC progression by promoting the EMT.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Science and Technology Department of Zhejiang Province (2015c33262, 2012C23105) and Zhejiang Medical Association Clinical Research Fund (2013ZYC-B9).