
Abstract
The matrix metalloproteinase-9, E-cadherin, and vascular endothelial growth factor play an important role in behavior of tumor cell growth, invasion, and metastasis. In this study, we investigated the relationships of matrix metalloproteinase-9, E-cadherin, and vascular endothelial growth factor expression with clinicopathological features and results of chemosensitivity tested by collagen gel droplet–embedded culture–drug sensitivity test in gastric cancer. Fresh specimens were used for collagen gel droplet–embedded culture–drug sensitivity test and paired fixed specimens were used for immunohistochemistry. Positive expression of matrix metalloproteinase-9 was associated with poorly differentiated carcinoma (p = 0.032), lymph node metastasis (p = 0.022), and tumor stage (p = 0.023). Negative expression of E-cadherin was associated with poorly differentiated carcinoma (p = 0.007), lymph node metastasis (p = 0.012), and tumor stage (p = 0.007). Positive expression of vascular endothelial growth factor was associated with tumor size (p = 0.040) and stage (p = 0.007). Collagen gel droplet–embedded culture–drug sensitivity test was successfully evaluated in 56 patients. Among them, 29 (51.7%) patients were resistant to TS-1 and 31 (55.3%) patients were resistant to L-OHP. The L-OHP resistance rate in vascular endothelial growth factor positive patients was significantly higher than that in negative patients (p = 0.031). The L-OHP resistance rate in E-cadherin negative patients was significantly higher than that in positive patients (p = 0.014). In conclusion, matrix metalloproteinase-9, E-cadherin, and vascular endothelial growth factor were involved in tumor invasion and metastasis. Positive expression of matrix metalloproteinase-9 and vascular endothelial growth factor and negative expression of E-cadherin were malignant markers for gastric cancer. Positive expression of vascular endothelial growth factor and negative expression of E-cadherin were associated with L-OHP resistance.
Keywords
Introduction
Although the incidence and mortality are decreasing, gastric cancer is still one of the most common cancers and the second leading cancer-related death worldwide.1,2 Now, despite the standard surgical resection, adjuvant and neoadjuvant chemotherapy combined with targeted therapy, the outcome of gastric cancer is still poor.3,4 The extracellular matrix (ECM) in which a variety of cytokines, vasculature-related cells, immune cells, and fibroblasts embedded play a key role in tumor migration and invasion. 5
The cell-adhesion molecule E-cadherin which mediates cell–cell and cell–matrix adhesion plays an important role in establishment and maintenance of the epithelial integrity of ECM, and downregulation of E-cadherin is the first step of tumor cell migration and metastasis.6,7 The loss of E-cadherin is associated with tumor grade and clinical outcome in several types of tumors.8,9
The migration and invasion of cancer cells are depended on the degradation of ECM. 10 Matrix metalloproteinase-9 (MMP-9) is a member of zinc-containing endopeptidases family that plays an important role in degradation of ECM and involved in angiogenesis and invasion mechanism.11,12
Tumor growth depends on the formation of new blood vessels for supplying of oxygen and nutrients. 13 The vascular endothelial growth factor (VEGF) plays an essential role in sprouting of angiogenesis. VEGF is essential for tumor growth and metastasis by promoting angiogenesis and lymphangiogenesis. 14 It also confers resistance to chemotherapy by enhancing Bcl-2 expression. 15 As a target for anti-cancer treatment, bevacizumab and tyrosine kinase inhibitors which are binding to vascular endothelial growth factor receptors (VEGFRs) are clinically used. 16
Collagen gel droplet–embedded culture–drug sensitivity test (CD-DST) is a novel developed chemosensitivity test, in which tumor cells are dispersed and embedded in three-dimensional collagen gel, a similar in vivo condition exists, the original growth characteristics of tumor cells are maintained, and the results were assessed using physiological concentrations of anti-cancer drugs.17,18 CD-DST is widely applied for the evaluation of individualized treatment for patients with ovarian cancer, uterine cancer, gastric cancer, colorectal cancer, lung cancer, breast cancer, and pancreatic cancer.17–22
In this study, we examined MMP-9, E-cadherin, and VEGF expression in patients with gastric cancer by immunohistochemistry. The relationships of MMP-9, E-cadherin, and VEGF expression with clinicopathological features and response to chemosensitivity tested by CD-DST were also analyzed.
Materials and methods
Patients and samples
After obtained approval from Medical Ethics Committee of the Affiliated Tumor Hospital of Harbin Medical University and consent from patients, fresh and formalin-fixed, paraffin-embedded gastric cancer tissues and adjacent normal tissues were obtained from 64 patients with primary advanced gastric cancer at Department of Gastroenterology Surgery, the Affiliated Tumor Hospital of Harbin Medical University from November 2014 to March 2015.
All patients underwent radical resection and histologically confirmed adenocarcinoma. The median age was 56 years (range from 18 to 70 years). The Eastern Cooperative Oncology Group (ECOG) performance status score was ≤2, and Karnofsky performance status score was ≥70 and the predicted survival time was more than 6 months. Patients with previous adjuvant chemotherapy, immunotherapy or radiotherapy, anti-cancer drug allergy, sever bone marrow, and heart, liver, and kidney functional deficit were excluded. Tumor stage and histological classification were classified according to the seventh edition of Union for International Cancer Control/American Joint Committee on Cancer (UICC/AJCC) tumor–node–metastasis (TNM) classification.
Immunohistochemical staining and evaluation
Following the manufacturer’s protocols, immunohistochemical staining for VEGF, MMP-9, and E-cadherin was performed on each gastric cancer sample using the Two-Step IHC Detection Reagent Kit (Zhong Shan Golden Bridge Biological Technology Inc., Beijing, China). Sections of 4 µm thick were baked, deparaffinized, and rehydrated. Slides were then incubated for 10 min with 3% H2O2 to remove endogenous peroxidase. After being pretreated with 0.01 mol/L citrate buffer (pH 6.0) and autoclaved for 5 min, the sections were incubated with MMP-9 (1:200 dilution; Abcam, Cambridge, MA), E-cadherin (1:50 dilution, Neomarkers), and VEGF (1:100 dilution, Abcam, Cambridge, MA) overnight at 4°C. After incubated with secondary antibody (Zhong Shan Golden Bridge Biological Technology Inc.) at room temperature for 20 min, each section was then counterstained with hematoxylin.
Cytoplasmic staining of VEGF and E-cadherin in tumor cells with moderate or strong staining was considered as positive staining. Nuclear staining of MMP-9 in tumor cells with moderate or strong staining was considered as positive staining. We counted 400 tumor cells and calculate the percentage of positively stained cells. MMP-9, E-cadherin, and VEGF were defined as positive expression when a specimen shows >10% of stained cancer cells.
The staining on each slide was evaluated by two independent pathologists who were blinded with the clinicopathological information, and a final consensus was reached.
CD-DST procedure
The CD-DST was performed as described previously.20,23 Briefly, CD-DST was performed by using a CD-DST kit provided by Nitta Gelatin (Osaka, Japan). Fresh specimens were obtained immediately after tumor resection, and tumor cells were collected after mincing, digestion, centrifugation, and filtration. Collagen gel was prepared by type I collagen (Cellmatrix Type CD; Nitta Gelatin), 10 × F-12 medium, and reconstitution buffer mixed together in a ratio of 8:1:1. Adjust the collected viable cells, which were added to the collagen solution with a final cell density of 2–5 × 105 mL−1 (about 3 × 103 cells/collagen gel droplet). Three drops of the collagen–cell mixture were placed in each well of a six-well culture plate and incubated in a CO2 incubator at 37°C for 1 h to make sure the collagen gel complete coagulation. After the overnight (12–24 h) incubation, the anti-cancer drugs were added at a final concentration of TS-1 (Tegafur Gimeracil and Oteracil Porassium Capsules, 1.0 µg/mL) for 144 h and L-OHP (oxaliplatin, 0.5 µg/mL) for 24 h according to human quotient of the area under the concentration–time curve.
At the end of incubation, collagen droplets were stained by 50 µg/mL of neutral red solution, fixed with 10% formalin buffered at neutral pH, washed in water, air dried, and then subjected to evaluation by imaging analysis. The collagen droplet in the 60 mm dish (control) was stained on the first day. The CD-DST results were represented as the T/C ratio (total volume of the treated group/total volume of the control group), and 60% or less was regarded as sensitive. When a growth rate was 0.8 or less, the assay was judged as unsuccessful irrespective of the volume of the control group (judged as low growth rate).
Statistical analysis
All statistical analyses were performed using SPSS 17.0 software (SPSS, Chicago, IL, USA). The relationships of MMP-9, E-cadherin, and VEGF expression with clinicopathological factors and results of CD-DST were tested by χ 2 test. The growth rate and T/C% ratio of CD-DST was tested by Student’s t-test. Two-tailed p value of 0.05 was statistically significant.
Results
In this study, 8 patients were excluded due the failure in CD-DST evaluation, and 56 patients were enrolled at last. The clinicopathological features of patients are shown in Table 1. The median age was 56 years (ranges from 23 to 69 years), and most of the patients were male (73.2%) with poorly differentiated carcinoma (69.6%) and lymph node metastasis (75%). There were 29 (51.7%) patients with a tumor size more than 5 cm. The expression of MMP-9, E-cadherin, and VEGF in gastric cancer tissues is displayed in Figure 1.
The clinicopathological features of patients.

TNM: tumor–node–metastasis; G1: well; G2: moderate; G3: poor; G4: undifferentiated.

Representative immunohistochemical staining of MMP-9, E-cadherin, and VEGF in gastric cancer tissues. (a) Positive expression of MMP-9, (b) negative expression of MMP-9, (c) positive expression of E-cadherin, (d) negative expression of E-cadherin, (e) positive expression of VEGF, and (f) negative expression of VEGF.
The relationships of MMP-9, E-cadherin, and VEGF expression with clinicopathological factors were shown in Table 2. The positive expression of MMP-9 was found in 36 (64.3%) patients and positive expression of MMP-9 was associated with poorly differentiated carcinoma (p = 0.032), lymph node metastasis (p = 0.022), and tumor stage (p = 0.023). The positive expression of E-cadherin was found in 23 (41.1%) patients and negative expression of E-cadherin was associated with poorly differentiated carcinoma (p = 0.007), lymph node metastasis (p = 0.012), and tumor stage (p = 0.007). The positive expression of VEGF was found in 26 (46.4%) patients and positive expression of VEGF was associated with tumor size (p = 0.040) and stage (p = 0.007).
The relationships of MMP-9, E-cadherin, and VEGF expression with clinicopathological factors.

TNM: tumor–node–metastasis; G1: well; G2: moderate; G3: poor; G4: undifferentiated; MMP-9: matrix metalloproteinase-9.
The relationships of MMP-9, E-cadherin, and VEGF expression are shown in Table 3. The positive expression of MMP-9 was associated with negative expression of E-cadherin (p = 0.002), and negative expression of E-cadherin was associated with positive expression of VEGF (p = 0.015). Although the positive rate of VEGF in MMP-9-positive patients (55.6%) was higher than in MMP-9-negative patients (30%), it was not statistically significant (p = 0.095).
The relationships between the expression of MMP-9, E-cadherin, and VEGF.

MMP-9: matrix metalloproteinase-9; VEGF: vascular endothelial growth factor.
In this study, we totally have 56 patients with successful CD-DST evaluation and 8 patients with unsuccessful evaluation because of insufficient number of viable tumor cells, poor growth rate in collagen gel droplets (growth rate less than 0.8), and fibroblast and bacterial contamination. The median growth rate of cancer cells over 7 days of incubation was 1.3 (ranges from 0.80 to 4.95). The median T/C values were 59.58% and 59.72% for TS-1 and L-OHP, respectively. In all, 29 (51.7%) patients were resistant to TS-1 (T/C ≥ 60%) and 31 (55.3%) patients were resistant to L-OHP (T/C ≥ 60%). The morphology of gastric cancer cells grown in collagen gel droplets is shown in Figure 2.
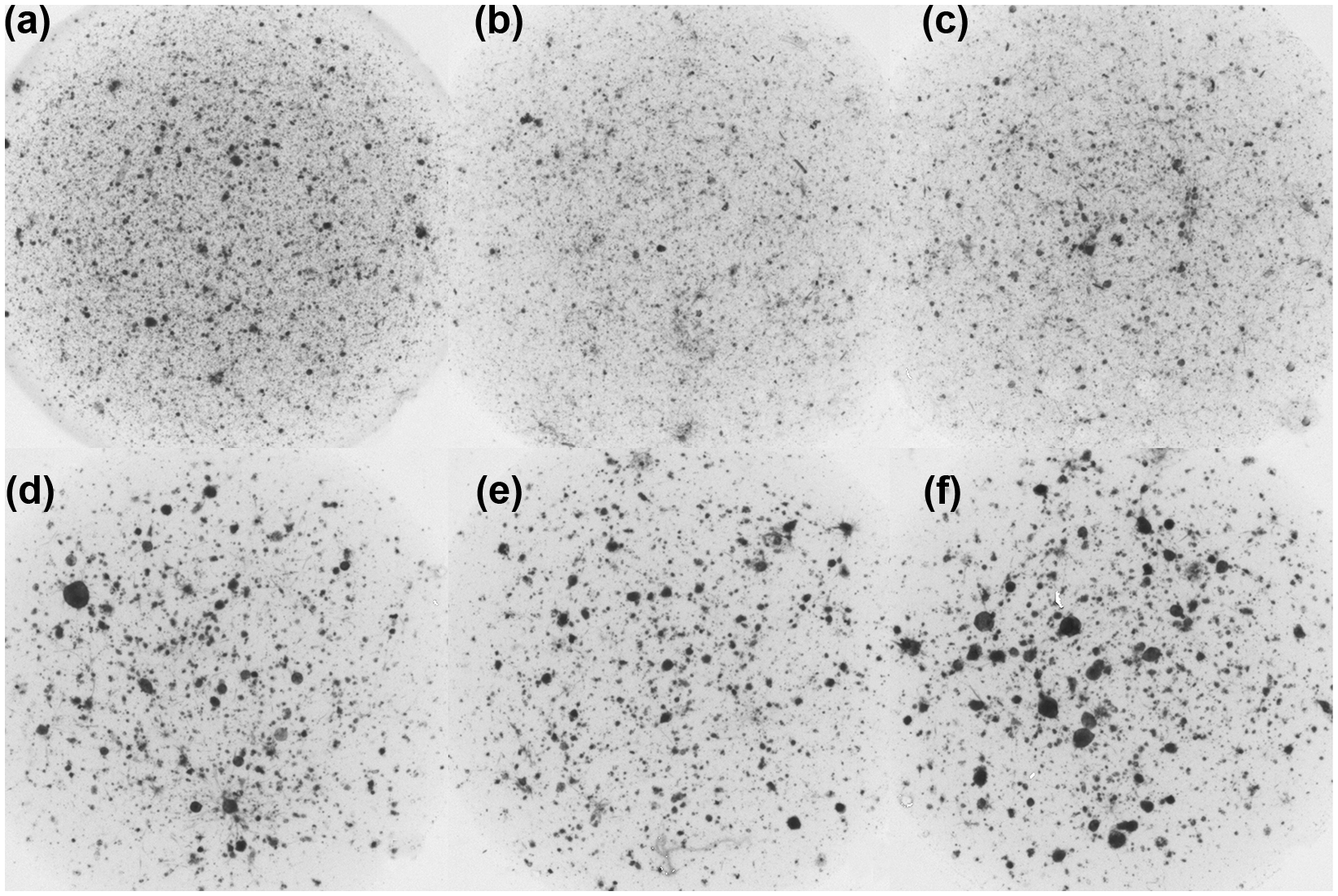
Representative results of CD-DST. The sensitivity was expressed as T/C ratio (T was the total volume of the treated group and C was the total volume of the control group). (a) Control for (b) and (c). Growth rate = 1.23. The morphology of gastric cancer cells grown in collagen gel droplets on day 7. (b) Sensitive to TS-1 (Tegafur Gimeracil and Oteracil Porassium Capsules). T/C ratio = 22.51% in gastric cancer at a concentration of 1.0 mg/mL. (c) Sensitive to L-OHP (Oxaliplatin). T/C ratio = 29.92% in gastric cancer at a concentration of 0.5 µg/mL. (d) Control for (d) and (e). Growth rate = 1.53. The morphology of gastric cancer cells grown in collagen gel droplets on day 7. (e) Resistance to TS-1. T/C ratio = 64.95% in gastric cancer at a concentration of 1.0 µg/mL. (f) Resistance to L-OHP. T/C ratio = 75.87% in gastric cancer at a concentration of 0.5 µg/mL.
The relationships between MMP-9, E-cadherin, and VEGF expression and results of CD-DST are shown in Table 4. The L-OHP resistance rate in VEGF-positive patients was significantly higher than that in VEGF-negative patients (73.1% vs 40%, p = 0.031). The L-OHP resistance rate in E-cadherin-negative patients was significantly higher than that in E-cadherin-positive patients (69.7% vs 34.7%, p = 0.014). The L-OHP resistance rate in the combination of VEGF-positive and E-cadherin-negative patients was 85% (17/20), it was higher than that in single VEGF-positive or E-cadherin-negative patients.
The relationships of MMP-9, E-cadherin, and VEGF expression with the results of CD-DST.

CD-DST: collagen gel droplet–embedded culture–drug sensitivity test; TS-1: Tegafur Gimeracil and Oteracil Porassium Capsules; L-OHP: Oxaliplatin; MMP-9: matrix metalloproteinase-9; VEGF: vascular endothelial growth factor.
Discussion
ECM and basement membrane play an important role in maintaining the integrity of ECM. 13 It is the first step to pass the ECM and penetrate through the basement membrane for tumor cell invasion and metastasis. 24 So, the decreased expression of E-cadherin (which maintains the integrity of ECM) and overexpression of MMP (degradation of ECM and basement membrane) play an important role in tumor cell invasion and metastasis. 23
The inhibition of MMP influenced tumor cell proliferation, migration, and invasion through downregulation of the expression of transforming growth factor-β (TGF-β), epidermal growth factor (EGF), nuclear factor-κB (NF-κB), VEGF, matrix metalloproteinase-2 (MMP-2), and MMP-9 and upregulation of the expression of E-cadherin.25,26 The overexpression of MMP-9 and loss of E-cadherin were associated with tumor stage, histopathological grade, tumor depth of invasion, lymph node metastasis, lymphatic vessels, vascular invasion, and poor survival. 27 Further studies demonstrated that upregulation of MMP-9 accompanied by downregulation of E-cadherin was a better survival predictor than single factor. 28
The E-cadherin played an important role in tumor angiogenesis. Studies found that the downregulation of E-cadherin regulated by miR-9 could promote upregulation of VEGF, 29 and E-cadherin could also mediate VEGF expression through extracellular signal–regulated protein kinase (ERK)/AKT pathways. 30
In this study, the positive expression of MMP-9 and negative expression of E-cadherin were associated with tumor stage, histopathological grade, and lymph node metastasis. The positive expression of VEGF was associated with tumor size and stage. The positive expression of MMP-9 was associated negative expression of E-cadherin, and negative expression of E-cadherin was correlated with positive expression of VEGF. These indicated that MMP-9, E-cadherin, and VEGF were involved in tumor invasion and metastasis and there was interaction between MMP-9, E-cadherin, and VEGF expression.
CD-DST was a novel developed chemosensitivity test, and it had some advantages compared with other traditional in vitro chemosensitivity tests. First, it needs a small number of tumor cells (3 × 103); second, it has high success rate in primary cell culture; third, it is examined by actual physiological concentrations of drugs; and finally, it eliminates the contamination of fibroblasts by neutral red solution staining and the results are evaluated by computer image analysis system.19,22,23
In this study, CD-DST was successfully performed in 56 (87.5%) patients, and 27 (48.2%) patients were sensitive to TS-1 and 25 (44.6%) patients were sensitive to L-OHP. As we know, this result was very similar to the actual response to chemotherapy. 31 In addition, this also demonstrated a good correlation between CD-DST and clinical therapeutics. The relationships between MMP-9, E-cadherin, and VEGF expression and the results of CD-DST indicated that the positive expression of VEGF and negative expression of E-cadherin were associated with L-OHP resistance. The combination of positive expression of VEGF positive and negative expression of E-cadherin negative was a sensitive predictor for L-OHP resistance.
In conclusion, MMP-9, E-cadherin, and VEGF were involved in tumor invasion and metastasis. Positive expression of MMP-9 and VEGF and negative expression of E-cadherin were malignant markers for gastric cancer. MMP-9 was associated with degradation of E-cadherin, and loss of E-cadherin was involved in angiogenesis. Positive expression of VEGF and negative expression of E-cadherin were associated with L-OHP resistance.
Footnotes
Acknowledgements
The authors thank Jingyu Chen and Xuesong Ding for help in CD-DST assistance. The authors also thank Qi Huang and Xiang Ban for immunohistochemistry assistance. H.G. and X.L. contributed equally to this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received no financial support for the research, authorship, and/or publication of this article.