
Abstract
Previous studies have suggested that leukocyte telomere length is associated with risk of developing prostate cancer. Investigations of leukocyte telomere length as a prognostic factor in prostate cancer are, however, lacking. In this study, leukocyte telomere length was investigated both as a risk marker, comparing control subjects and patient risk groups (based on serum levels of prostate-specific antigen, tumor differentiation, and tumor stage), and as a prognostic marker for metastasis-free and cancer-specific survival. Relative telomere length was measured by a well-established quantitative polymerase chain reaction method in 415 consecutively sampled individuals. Statistical evaluation included 162 control subjects without cancer development during follow-up and 110 untreated patients with newly diagnosed localized prostate cancer at the time of blood draw. Leukocyte telomere length did not differ significantly between control subjects and patients, or between patient risk groups. Interestingly, however, and in line with our previous results in breast and kidney cancer patients, relative telomere length at diagnosis was an independent prognostic factor. Patients with long leukocyte telomeres (⩾median) had a significantly worse prostate cancer–specific and metastasis-free survival compared to patients with short telomere length. In contrast, for patients who died of other causes than prostate cancer, long relative telomere length was not coupled to shorter survival time. To our knowledge, these results are novel and give further strength to our hypothesis that leukocyte telomere length might be used as a prognostic marker in malignancy.
Introduction
Over the last decade, a large number of studies have investigated whether leukocyte telomere length (TL) could be used as a biomarker in malignancy, predominantly as a marker of cancer risk. However, the results have been inconsistent. Initially, a majority of mainly retrospective studies reported associations between short leukocyte TL and increased cancer risk, as summarized in Ma et al. 1 and Wentzensen et al. 2 However, an increasing number of studies, including several prospective, have found associations between long TL and risk of certain cancer types,3–8 and even a U-shaped association has been reported.9–12 In addition, several investigations have reported null association between leukocyte TL and cancer risk.1,2,13,14 For a recent review on the subject, see Barrett et al. 15 The discrepancy in results may be due to several factors, such as differences in study design (retrospective vs prospective), type of cancer, and laboratory protocols. The dynamic feature of leukocyte TL suggested by us is also likely a factor of relevance in this aspect. 16 Homeostasis of TL appears to be complex, involving a large number of intrinsic and extrinsic factors, such as heredity, epigenetics, aging, stress, immune components, and hormones. 17
The potential of leukocyte TL to act as a prognostic factor in cancer patients has been less explored. We previously reported that leukocyte TL, measured at diagnosis, was associated with cancer-specific survival in patients with breast cancer 3 and renal cell carcinoma. 18 In both patient groups, individuals with longer leukocyte TL had a worse outcome compared to those with shorter TL. Recently, we found the same pattern in patients with colorectal carcinoma. 19 Similar results have also been reported in patients with hepatocellular carcinoma. 20
Prostate cancer (PC) is the most common cancer among men. Investigations of leukocyte TL as a possible biomarker in PC are sparse. In a nested case–control study, Mirabello et al. 21 found that men with shorter TL had decreased risk of advanced PC. In another recent prospective study by Julin et al., 8 longer leukocyte TL was modestly associated with higher risk of PC.
In this study, we measured relative telomere length (RTL) in 415 individuals using a quantitative polymerase chain reaction (qPCR)-based telomere assay. Some individuals were later excluded from the main statistical analyses for various reasons, for example, control subjects with later diagnosis of PC, high-grade prostatic intraepithelial neoplasia (PIN), or other cancers. Therefore, 272 individuals were eventually included in the final statistical calculations: 162 control subjects and 110 untreated patients with newly diagnosed localized PC at the time of blood sampling. Leukocyte RTL was evaluated in relation to patient subgroups (low risk, intermediate risk, high risk, based on tumor differentiation and stage as well as serum levels of prostate-specific antigen (PSA)) and controls. In addition, survival analysis was performed to investigate whether leukocyte TL at the time of PC diagnosis carried prognostic information in relation to metastasis-free and cancer-specific survival times.
Materials and methods
Patient and control subjects
Patients were recruited from the Urology section at the Department of Surgical and Perioperative Sciences at University Hospital of Umeå. Blood samples were collected at the time of diagnosis (mean time interval 0.30 months between date of blood draw and diagnosis) between the years of 2003 and 2006, and all samples were collected before any treatment. In all, 418 patient samples were originally included in the study, and 415 samples were successfully purified and analyzed. Through a thorough review of patient records and cancer registries (June–August 2014), the following groups were identified:
A total of 162 individuals qualified as control subjects. These patients were originally examined because of increased PSA levels and suspicion of PC, but no PC was detected at sampling and they were still cancer-free in August 2014.
Totally 119 individuals qualified as cases, with PC diagnosed at the time of blood sampling. Among these patients, nine patients had spread disease at diagnosis (N1 and/or M1) and were excluded from analysis. The other patients (n = 110) were classified as low risk (T1–2, Gleason score ⩽ 6, and PSA < 10; n = 44), intermediate risk (T1–2 and/or Gleason score 7, and/or PSA 10–20 ng/mL; n = 39), or high risk (T3–4 and/or Gleason score ⩾ 8, and/or PSA > 20; n = 27) patients.
In all, 121 individuals did not qualify as control subjects and were therefore excluded from the main statistical analyses. Among them were 71 individuals with no detected PC at the time of blood sampling, but who later developed PC according to patient records and cancer registries. A total of 50 individuals were found to have other cancers than PC at the time of blood sampling or were later diagnosed with high-grade PIN or another cancer. In addition, 13 patients did not qualify as cases. These PC patients were excluded due an additional cancer diagnosis (which had been diagnosed ±5 years from blood sampling).
Hence, the main statistical evaluation encompassed 162 controls with no detected PC and 110 individuals with PC but with no metastasis. At the time of the last follow-up (August 2014), 91 of these patients had still localized PC, whereas 17 patients had developed metastasis (N1 and/or M1) over the time-course (mean time interval, 65 months; range, 24–93 months). For two patients, no follow-up data were available regarding metastatic status since the participants had moved outside the study region at the time of follow-up. In all, 11 patients had died due to PC, whereas 10 patients had died of other causes at the time of the last follow-up. The causes of death for the latter 10 patients included aortic dissection, cerebrovascular disease, acute myocardial infarction, motor neuron disease, vascular dementia, and diabetes mellitus. Death-related data were missing for four patients.
Each patient participated after providing written informed consent at the time for blood donation. The study was approved by the ethical committee (dnr 2013-57-31M), Umeå University, Umeå, Sweden.
DNA extraction
DNA was extracted from buffy coat samples using the Qiagen BioRobot M48 workstation with MagAttract technology (Qiagen, Hilden, Germany), as described elsewhere. Three samples were excluded due to unsuccessful purification. The rest (n = 415) were included in the qPCR analysis for TL measurements.
TL measurements
TL was measured using qPCR, based on the method originally described by Richard Cawthon 22 in 2002. All qPCR assays were performed in 384-well plates, using the ABI Prism 7900HT sequence detection system (Applied Biosystems by Thermo Fisher Scientific, Waltham, Massachusetts, USA). For a detailed description of reagents, primers, and cycling conditions, see Nordfjäll et al. 23 (but with the following change: 2.5 mM MgCl2 in the HBG Master mix, Thermo Fisher Scientific). Prior to qPCR analysis, DNAs from the patient samples and from the reference cell line CCRF-CEM were diluted to 2.19 ng/µL in 1×TE (10 mM Tris, 1 mM EDTA, pH 8) buffer containing Escherichia coli DNA (Sigma–Aldrich), using Beckman Coulter Biomek 2000 Robot (Beckman Coulter, Brea, Kalifornien, USA). Samples were thereafter denatured at 95°C for 30 min, as described previously. 23 The reference DNA was also used to produce standard curves for each plate (range, 3.7–50 ng) to monitor the PCR efficiency. The diluted DNA samples were mixed with telomere or HBG Master mix, using the Biomek Robot. Each 20 µL reaction volume contained 12 µL master mix + 8 µL DNA (17.5 ng), and all samples were loaded as triplicates in each 384-well PCR plate. Telomere/single copy gene (T/S) values were calculated using the formula T/S = 2−ΔCt, where ΔCt = average Cttelomere − average CtHBG. Relative T/S values (i.e. RTL) were generated by dividing sample T/S values with the T/S value of the reference DNA. The mean intra-assay coefficient of variation (CV; calculated by comparing the T/S value of the 17.7 ng standard curve point with the T/S value of the reference sample of each plate) was 1.97%. The mean RTL value ± standard deviation (SD) for the 17.7 ng standard was 0.98 ± 0.035, giving an inter-assay CV of 3.57%. In addition, 15 patient samples were measured twice at separate occasions. The mean inter-assay CV for these samples was 2.60%.
Statistical analysis
Before performing statistical calculations, variables were checked for normality and ln-transformed when necessary, in order to achieve a normal distribution. Between-group differences were investigated by analysis of covariance (ANCOVA), including age as a covariate. Correlations were investigated using Pearson’s correlation coefficient or partial correlation with age adjustment. Survival analysis was performed using Kaplan–Meier survival curves, with the log-rank test for univariate comparison and Cox proportional hazard model for multivariate analysis. Survival was defined as the time in months between the date of diagnosis to the date of last follow-up (August 2014) or to the date of an event. Statistical significance refers to p ⩽0.05 (two-tailed).
Results
Basic cohort characteristics
As described in section “Materials and methods,” the main statistical evaluation encompassed 110 individuals with PC but with no metastasis at diagnosis. Basic patient characteristics for this group can be found in Table 1. In all, 162 individuals qualified as control subjects with no detected PC during follow-up. Pearson’s correlation analysis showed that RTL was negatively correlated with age as expected (the whole group: r = −0.221, p < 0.001, n = 272), with the strongest correlation found in the patient group (r = −0.346, p < 0.001, n = 110). No significant correlation was found between leukocyte RTL and PSA levels at diagnosis, when performing partial correlation analysis adjusting for age (r = −0.022, p = 0.821, n = 110). About 23% (6 out of 26) of the patients in the high-risk group developed metastasis (N1 and/or M1) over the time-course, as compared to 21% (8 out of 38) of the intermediate-risk patients and 7% (3 out of 44) of the low-risk patients. Almost all patients who later developed metastasis (14 out of 17) had an RTL value ⩾median.
Basic characteristics for patients with localized prostate cancer at diagnosis.

PSA: prostate-specific antigen.
Between-group comparisons of TL
Between-group differences were investigated with age as a covariate. Comparison of control subjects and patients showed no significant difference in mean RTL between the two groups (age-adjusted mean RTL with 95% confidence interval (CI); 0.95 (0.92–0.97) and 0.92 (0.90–0.95), respectively; p = 0.223). This is also illustrated in Figure 1, showing patient subgroups (low risk, intermediate risk, and high risk) versus controls. Although not included in the main statistical analysis, RTL comparison was also performed with the inclusion of the 71 individuals with no detected PC during the time of blood sampling, but who later developed PC. This group did not differ significantly in mean RTL compared to controls (p = 0.715) or the patient group with localized PC at blood sampling (p = 0.520; not shown in figure).

Comparison of relative telomere lengths (RTLs) between controls (n = 162) and patient subgroups, according to risk; low (n = 44), intermediate (n = 39), and high (n = 27). p-values represent age-adjusted values. Group comparisons were performed using ANCOVA with age as a covariate.
Univariate and multivariate survival analysis
Kaplan–Meier analysis with the log-rank test was performed to investigate whether leukocyte RTL carried any prognostic information. The patients were subdivided into two groups, with the median RTL value (0.92) as the cut-off and with PC-specific death as the event. Patients with long RTL (⩾median) had a significantly shorter cancer-specific survival (p = 0.039) compared to the patients with short telomeres (Figure 2(a)). Leukocyte RTL was also analyzed in relation to metastasis-free survival, using disease relapse with metastasis as the event. As mentioned above, 17 patients had developed metastasis over the time-course. Again, patients with long RTL (>median) had a significantly worse outcome compared to patients with shorter RTL (p = 0.010; Figure 2(b)). Finally, analysis was performed with “death by other causes than PC” as the event. Here, the opposite pattern was found with a trend to a worse survival for patients with shorter leukocyte RTL, but with a non-significant p-value (0.199; Figure 2(c)).
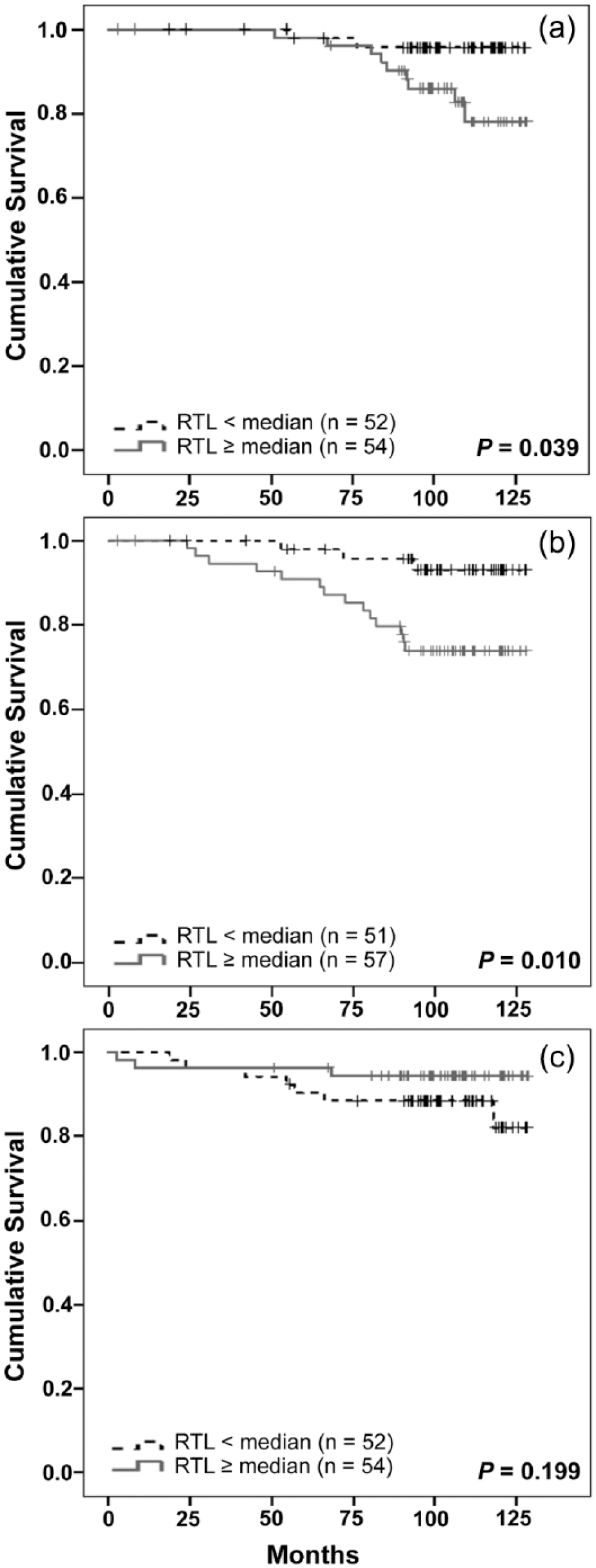
Kaplan–Meier survival analysis with the log-rank test, comparing patients with long versus short leukocyte RTL: (a) prostate cancer–specific survival, (b) metastasis-free survival, and (c) survival analysis where event was defined as death due to other causes than PC.
Importantly, multivariate Cox regression analysis, including age, leukocyte RTL, and patient risk groups (based on Gleason score, PSA, and T stage as described above), could verify long leukocyte RTL as an independent negative prognostic factor in relation to PC-specific death (Table 2) and disease progression with metastasis (Table 3). In accordance, leukocyte RTL also remained as an independent factor when Gleason score, T stage, and PSA were included as individual parameters in separate Cox analyses (data not shown).
Multivariable Cox regression analysis for prostate cancer–specific survival.

HR: hazard ratio; RTL: relative telomere length.
Patient risk groups as specified in section “Materials and methods.”
Multivariable Cox regression analysis for metastasis-free survival.

HR: hazard ratio; RTL: relative telomere length.
Patient risk groups as defined in section “Materials and methods.”
Discussion
In this study, we report novel findings showing that leukocyte TL, measured in newly diagnosed patients with localized PC, was associated with prognosis. Importantly, long TL remained as an independent negative factor for both metastasis-free survival and PC-specific death when evaluated together with established risk factors (tumor stage, Gleason score, and serum PSA). These results support previous findings in breast, kidney, colorectal, and hepatocellular carcinoma patients,3,18,19,20 where patients with long leukocyte TL had a poorer outcome.
We have previously presented an “immunohypothesis” where we suggest that a subgroup of patients with longer TL might have a less active/more suppressed immune system, with fewer cell divisions and less telomere shortening. To test this hypothesis, we previously measured peripheral levels of immunosuppressive regulatory T cells (Tregs) in kidney cancer patients and found a significant positive correlation between leukocyte TL and Treg-levels. 24 Similar results have been reported in patients with hepatocellular carcinoma. 20 In the latter study by Liu et al., long leukocyte TL was associated with a worse survival, and patients with long TL had a significantly increased percentage of Tregs. In our recent study on colorectal carcinoma patients, 19 patients with the highest degree of lymphocyte tumor infiltration had significantly shorter leukocyte TL compared to patients with the lowest degree of infiltration. Those with a higher degree of immune cell infiltration had a significantly better survival, which may reflect a more active immune system and hence fits with our immunohypothesis. This hypothesis is further supported by recent data showing that single-nucleotide polymorphisms (SNPs) associated with immunity were coupled to survival in patients with PC. 25
In order to explore our hypothesis further, we are currently conducting a prospective PC study, where we intend to investigate leukocyte TL in relation to the immune profile of peripheral blood, as well as to clinical characteristics, treatment response, and TL changes over time.
In this study, TL did not differ between patient subgroups at diagnosis or between patients and control subjects. Also, the 71 individuals with no detected PC at the time of blood sampling but who later developed PC did not differ in mean leukocyte TL compared to controls and cases. Hence, TL did not predict risk of developing PC in our cohort. In a recent and larger (922 cases and 935 controls) prospective study by Julin et al., 8 where blood samples were collected several years prior to diagnosis (mean time, 5.5 years), longer TL was modestly associated with higher risk of developing PC. Our cohort was considerably smaller and it is possible that larger sample size is needed to detect possible between-group differences. When evaluating TL as a potential risk marker for cancer, retrospective studies have the disadvantage that a detected association may reflect reverse causation bias, that is, the presence of a tumor and the time to diagnosis could have influenced leukocyte TL. This was shown by Hou et al. 26 in a recent study and further discussed by Gu. 27 Thus, leukocyte TL appears to be a dynamic feature influenced by the presence of a tumor26,27 and with fluctuations over time,16,28,29 and measuring TL many years before diagnosis may therefore be of limited use. On the other hand, investigating TL as a prognostic marker might provide useful information, if samples are collected around the time of diagnosis and before any therapy initiation (as was done in this study). Our present and previous results indicate that leukocyte TL could be a prognostic marker for several different cancer types. This is of interest, since there is a need for easily accessible and reliable prognostic markers at diagnosis, with the ability to differentiate patient subgroups with good and poor prognosis and thus aid in the choice of treatment strategies.
For patients who died of other causes than PC (mainly cardiovascular disease), long TL was not associated with significantly shorter survival time. Instead, the pattern was rather the opposite, although not statistically significant. Interestingly, in our recent colorectal carcinoma study, we found short RTL to be associated with significantly shorter survival time for M0 patients who died of other causes than colorectal cancer. These results lend support to previous reports showing that short leukocyte TL could be coupled to prospective mortality due to, for example, cardiovascular-related cause of death, as summarized in Sanders and Newman. 30 It also highlights the importance of using “cancer-specific survival” instead of “overall survival,” when investigating TL as a prognostic marker, since important survival patterns could otherwise be masked.
In summary, we here show that long leukocyte TL at the time of diagnosis was an independent negative marker for metastasis-free and PC-specific survival in patients with PC. Our results support the hypothesis that leukocyte TL carries prognostic information in malignancy. However, conclusions from this study are limited by the small study cohort and few events during follow-up and therefore need to be verified in larger studies. Based on previous results, we believe that immune-related factors are of importance for leukocyte TL in cancer patients and we aim to explore this matter further in an ongoing prospective PC study.
Footnotes
Acknowledgements
The authors want to thank Kerstin Almroth and Susann Haraldsson for skillful technical experience and Prof. Pär Stattin for contributing with clinical expertise.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was financially supported by the Swedish Cancer Society (CAN 2014/0558 and CAN 2013/845), the Swedish Research Council (2015-02393), the Cancer Research Foundation in Northern Sweden, and the County of Västerbotten.