
Abstract
Background
Presently, competency-based medical (CBME) curriculum challenges the medical educators to provide continuing education with new approaches to make learning more stimulating, motivating, and entertaining, fostering excellence in clinical practice. To address these issues, educators have advocated the use of virtual reality and mannequins to teach clinical pharmacology.
Objectives
To study the effect, perception, and feedback of virtual reality high-fidelity adult mannequin-based (VHFM) simulation of real-life clinical scenarios over conventional tutorials in teaching clinical pharmacology to medical students.
Material and Methods
An interventional study was designed for 2nd year MBBS students for a period of 6 months. The enrolled students were randomly assigned to the test group (VHFM) or control group (tutorials). The CAE Healthcare Ltd. maestro, high-fidelity prehospital mannequin (APOLLO) was used in the test group. Three sessions consisting of six different cases were discussed, and multiple-choice questions (MCQs)-based pre-test, post–test, and retest after a month were conducted in both groups and compared. The perception and feedback of faculty and students were obtained by using a modified and revalidated questionnaire.
Results
The test group outperformed the control group (p <.001) in all sessions based on pre-test, post-test, and retest scores, and within-group comparisons revealed significant improvements in both groups. Students’ perceptions and feedback regarding VHFM were more enthusiastic and promising than in the tutorial group.
Conclusions
VHFM is student-centered, provides an active learning environment, and aids in skill development. We strongly suggest VHFM-based learning as a complement to traditional teaching strategies in pharmacology, especially for teaching clinical reasoning to medical students.
Introduction
Conventional review sessions (tutorials) in medical education typically involve instructor-based learning and offer a brief recap of previously taught and frequently poorly remembered information. 1 Tutorials are helpful for giving background information on subjects, followed by a round of questions and answers. However, there is little room for critical thought or the application of newly learned information to clinical practise.2, 3 Because medical knowledge is rapidly evolving, more effective teaching techniques are required to improve the application of the educational process. 4 Clinical reasoning is the cornerstone of medical practise for health professionals, and the application of preclinical knowledge in clinical settings should receive more attention in medical education. 5
The competency-based medical (CBME) curriculum states that an undergraduate medical student should have the necessary skills to logically prescribe medications after taking the Pharmacology course. (a) Use medicine that is economical. (b) Know when not to administer medication. (c) Possess a thorough understanding of the pharmacokinetics and pharmacodynamics of the medications being used. (d) Gather data from reliable, established books and periodicals. (e) Engage in self-directed learning and lifelong learning. (f) Be able to administer medications via a variety of methods and have effective communication skills. Use a "P" list of preferred or personal medications. 6 Unfortunately, these goals cannot be reasonably achieved by didactic lectures and tutorials that are mostly lecture-based. Early clinical exposure and supportive attitudes must be encouraged for students. 7
Medical educators today have the difficult task of providing continuing education that promotes competence in clinical practise while also coming up with fresh ideas on how to make learning more exciting, motivating, and enjoyable. Technology integration in the classroom holds out the possibility of finding novel solutions to educational problems. In the current era of digitization and pervasive internet connectivity, computer-based learning, or eLearning, is a rapidly developing field in medical education. The use of virtual patients is a developing area of online learning (VP). The use of VP in medical education has been promoted by educators. 8 A VP is defined as an “interactive computer simulation of real-life clinical scenarios for medical training, teaching, or assessment.” 9 Different learning demands in medical education are addressed by this definition. 10 The educational use is explained by the experiential learning paradigm. 11
The virtual patients expose students to simulated clinical situations and offer tools for gathering data and making therapeutic decisions in a secure setting. 12 Virtual patients are online instances where the learner assumes the position of the doctor, is required to make all judgments, and is given feedback on these decisions. 9 The purpose of virtual reality is to expose pupils to situations that would be challenging to locate or deal with in the actual world. 13 By exposing the student to a variety of simulated clinical scenarios, learning processes are supported, and students gradually acquire and apply knowledge in a secure simulation before using it in actual clinical practise.7, 14
In comparison to mannequin-based simulation, virtual reality simulation is more affordable and simpler to install.7, 15 When there are no suitable real patients accessible, mannequins offer students a safe learning environment where they can experiment, repeat the process, and gain clinical skills.8, 16 Life-size mannequins known as high-fidelity simulators are capable of simulating a variety of human processes, including breathing, producing a pulse, producing a heartbeat, changing pupil size, blinking, and more. Clinical training experiences are improved by adding virtual patients and high-fidelity mannequin-based (VHFM) simulations. When face-to-face instruction isn’t possible, virtual reality can help undergraduate medical students learn clinical reasoning skills in particular. 17
It is necessary to take into account the published research, most recent systematic reviews, and meta-analyses that support the positive impacts of virtual patients. The use of this method to teach pharmacology to medical students is the subject of very little published research and literature. Therefore, the goal of this study is to initially assess the appeal, drive, and mindset of medical students who are learning through an interactive computer simulation of real-world clinical scenarios based on VHFM.
The study’s goals were as follows:
To compare the effectiveness of virtual reality high-fidelity mannequin-based simulations of real-life clinical scenarios to traditional tutorials in teaching of pharmacology. To determine the perception and feedback of students and faculty toward VHFM-based learning.
Methods and Materials8, 18, 19
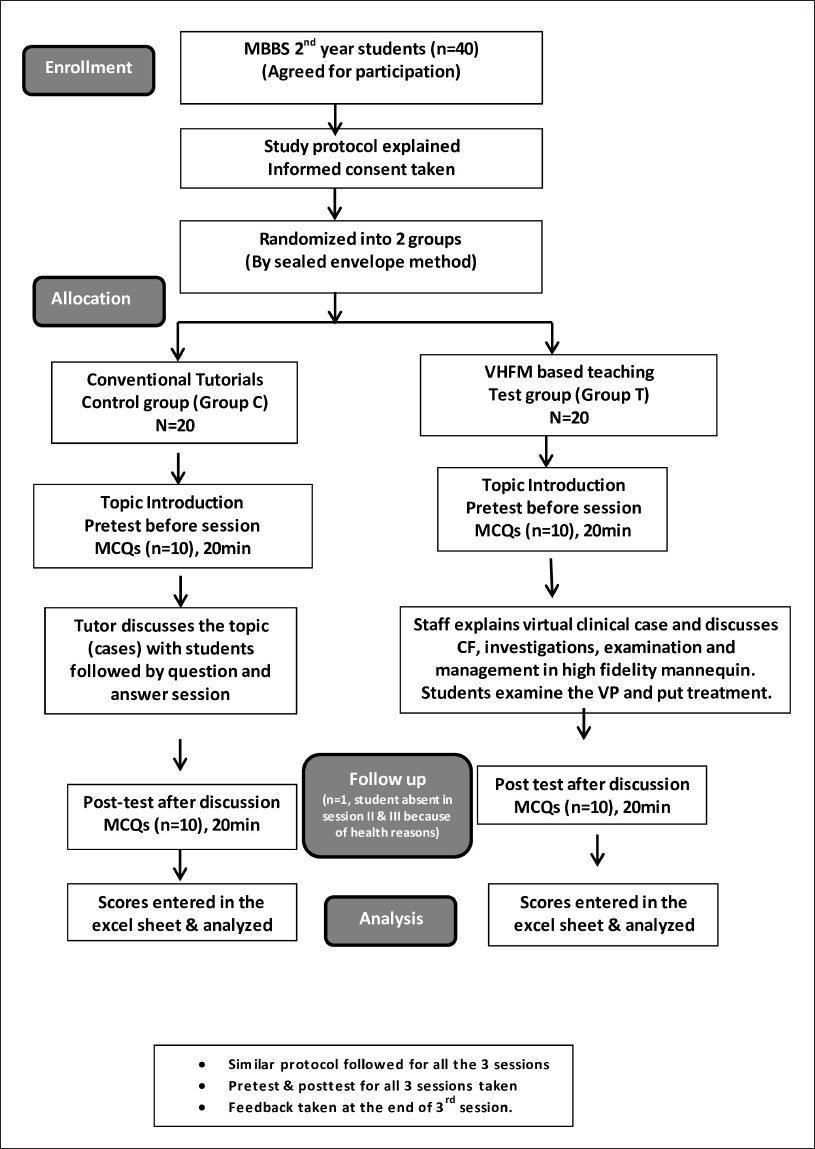
Ethical approval was obtained from the Institutional Ethical Committee (KAHER’s JN Medical College, Belagavi, Ref: MDC/DOME/321; dated: 02/03/2022), and the study was conducted over a period of 6 months (March 2022–August 2022) in the Department of Pharmacology, JN Medical College, KAHER, Belagavi, Karnataka, India. The interventional study, which examined a novel teaching strategy, was explained orally to the MBBS Phase II students. It was also made clear that participation was purely optional and that the findings would not affect their grades or final test scores. Using student identifying numbers (roll numbers or university registration numbers) rather than names allowed for the preservation of confidentiality throughout the investigation. Students were included in the study who willingly chose to take part. Each student provided written informed consent before being randomly assigned using the sealed envelope method into the control and test groups. With this approach, allocation information can be obtained rapidly and at a lower cost.
A total of 20 students made up the control group (Group C), which used the tutorials’ current traditional approach and was carried out by a faculty member in the tutorial room. A total of 20 students made up the test group (Group T), which used a VHFM-based simulation and carried it out in the Advanced Simulation Centre and Clinical Skill Lab (Figure 1). The pre-hospital high-idelity mannequin (Apollo), the most recent version of patient simulation software created by CAE Healthcare, was used by faculty members to accomplish the goals. The CAE Apollo adult patient simulator is wireless and offers a variety of features. 20
KLE Advanced Simulation Center − Apollo, High Fidelity Mannequin (CAE Maestro).

Based on the simulation software’s design, six themes (cases) from systematic pharmacology were chosen for the investigation. The sessions’ chosen themes were case of hyperthermia, myocardial infarction (cases of angina/STEMI), and other cardiovascular system (CVS) cases [hypertensive emergency, left heart failure, and arrhythmias (ventricular tachycardia (VT) and paroxysmal supraventricular tachycardia (PSVT))]. Case studies were created by consulting the clinical examination book and the standard medical textbook. 21 The pupils received the necessary information at the start of each session to ensure a successful study. The team first talks about the VP clinical case scenario’s introduction and history parts. Online audio and video were employed in this clinical vignette to introduce the user to the subject at hand.
Then the Apollo’s examination component was exhibited, and the investigation component’s essential lab tests were addressed. By contrasting the diagnosis component with an expert’s explanation, teachers were able to show students how to keep an eye on their own thinking (such as differential diagnoses and tests done). After that, the therapy component was discussed with the intention of getting the student involved in therapy by choosing the proper drug(s), dose, and route, as well as backing up the patient’s recommended management. Students evaluate their performance in the computer-based performance feedback in comparison to that of a professional, the VP author.
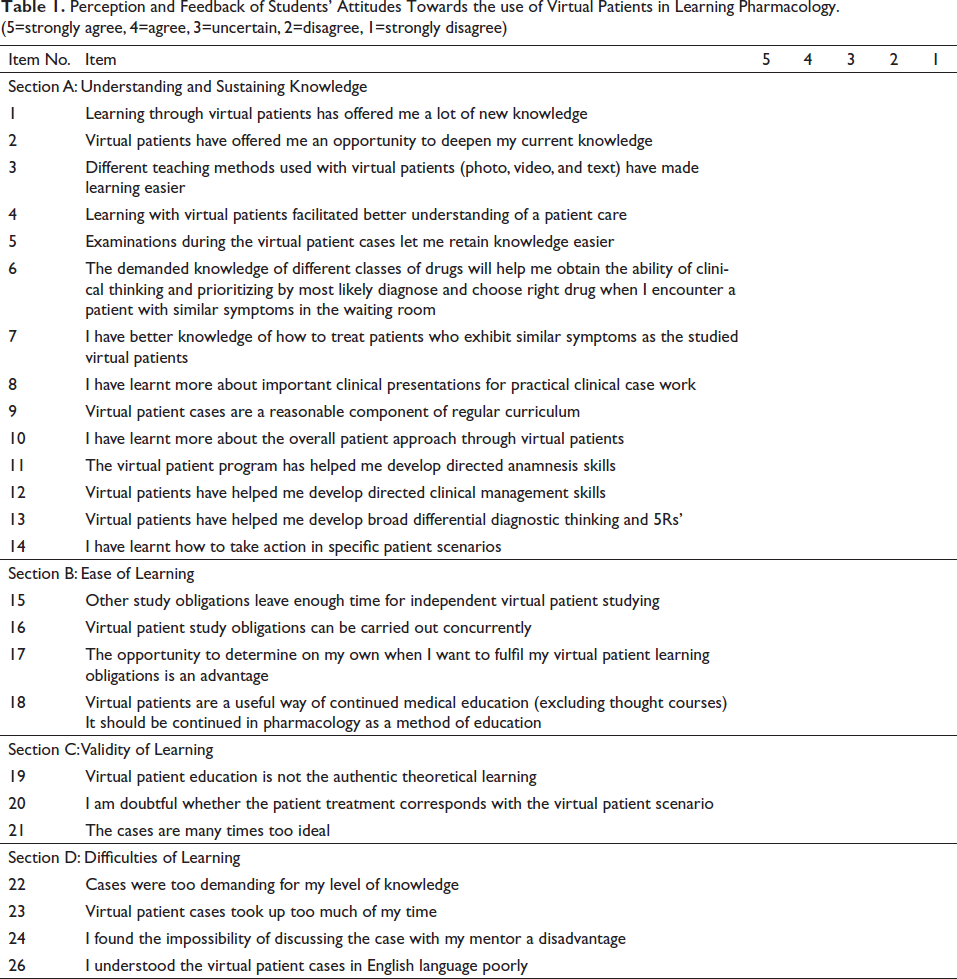
A paper-based pre-test and post-test were administered for each of the three sessions, consisting of 10 multiple-choice questions (MCQs) for each session, with the correct response receiving a “1” mark and the incorrect response receiving a “0” mark for both groups (Figure 2). An updated and revalidated feedback form with four sections and a 5-point Likert scale was also received from members of each group after all three sessions. Understanding and maintaining knowledge are covered in Section A, whereas learning ease, learning validity, and learning challenges are covered in Sections B, C, and D, respectively (Table 1). Each item’s response rate and total number of students were noted. Each item’s mean rating was computed. Observations and ideas from the students were also recorded.
Flowchart of Study.
Perception and Feedback of Students’ Attitudes Towards the use of Virtual Patients in Learning Pharmacology. (5=strongly agree, 4=agree, 3=uncertain, 2=disagree, 1=strongly disagree)
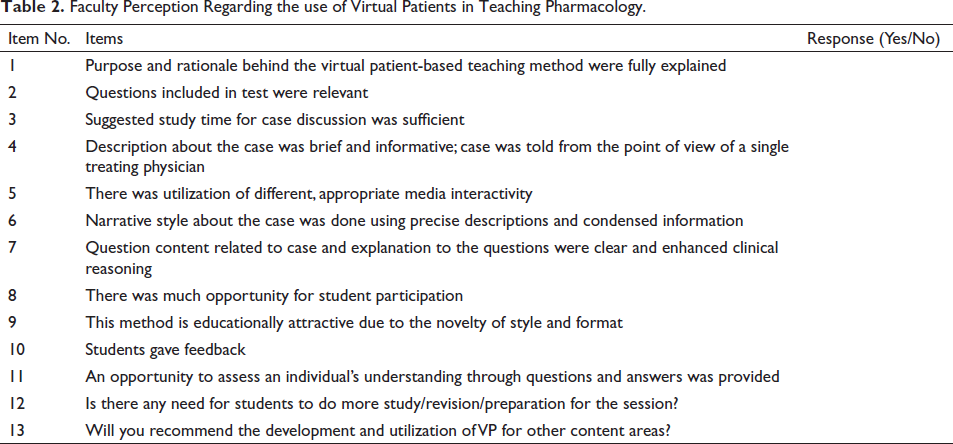
A revamped and revalidated questionnaire with 13 dichotomous items was used to determine how department staff and postgraduate students felt about VHFM. “Yes” responses received a score of “1,” while “No” responses received a score of “0” (Table 2). One month after the third session ended, a second exam with 25 MCQs was given to see how well both groups could retain the information.
Faculty Perception Regarding the use of Virtual Patients in Teaching Pharmacology.
Statistical Analysis
SPSS version 25.0 was used for the statistical analysis (IBM Corporation, Chicago, IL, United States). An independent sample t-test is used to compare between groups, and a paired t-test is used to compare within groups. The partial eta squared technique was used to calculate the effect size. The impact of the intervention was evaluated using the pre-test and post-test results from each of the three sessions. The following criteria were used to interpret the effect size measurements: Effect sizes range from 0 to 0.2 as mild, 0.2 to 0.5 as small, 0.5 to 0.8 as medium, and above 0.8 as large. Scores from the retest were also examined. The test’s average scores were presented as means with standard deviations. p <.05 was considered statistically significant.
Results
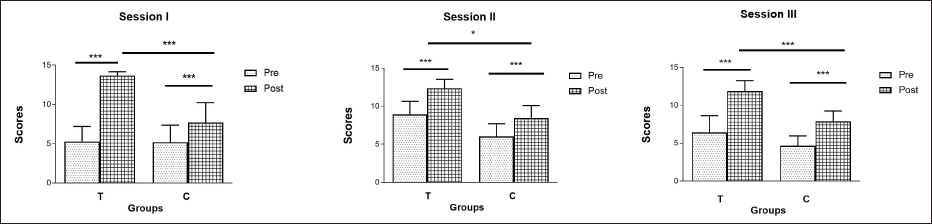
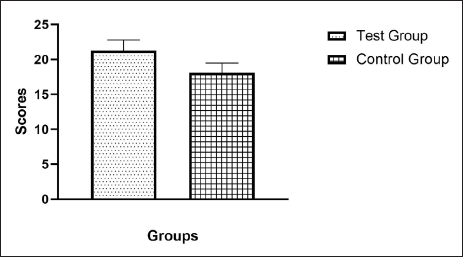
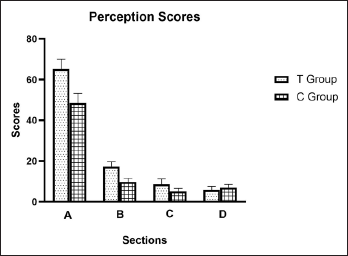
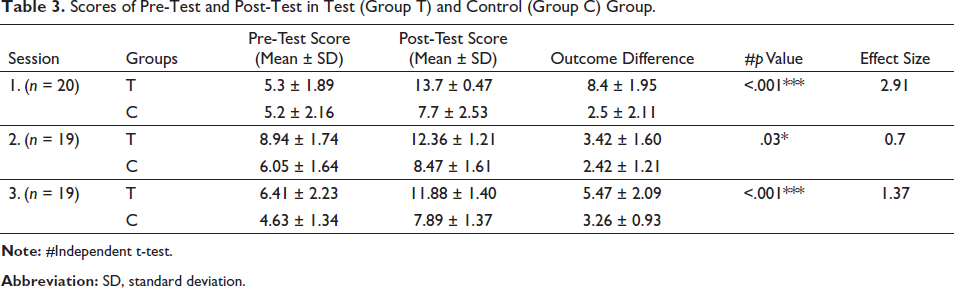
Pre-test and post-test results had a normal distribution of scores. A comparison of the groups’ results revealed that group T outperformed group C in each of the three sessions. There was a highly significant difference favouring group T in sessions 1 (p <.001), 2 (p <.03), and 3 (p <.001). In comparison to the control group, the effect magnitude was larger in Sessions I and III and medium in Session II. In the retest, group T performed better than group C (p <.001) (see Table 3 and Figure 3). Nevertheless, a comparison among groups revealed that both groups had significantly improved on each exam (p <.05) (Figure 4). Feedback from students and their opinions of VHFM-based learning are shown in (Table 4 and Figure 5). On the basis of a questionnaire with four sections and a 5-point Likert scale, the students’ perceptions of and satisfaction with the educational experience were assessed. Overall, the test group students were pleased with the sessions since they made learning more engaging and collaborative and gave them a sense of confidence.
Pre-Test and Post-Test Scores.
Retest Scores.
Students Perception and Feedback.
Scores of Pre-Test and Post-Test in Test (Group T) and Control (Group C) Group.
Feedback and Perception Scores of Sections A to D in Test (Group T) and Control (Group C).
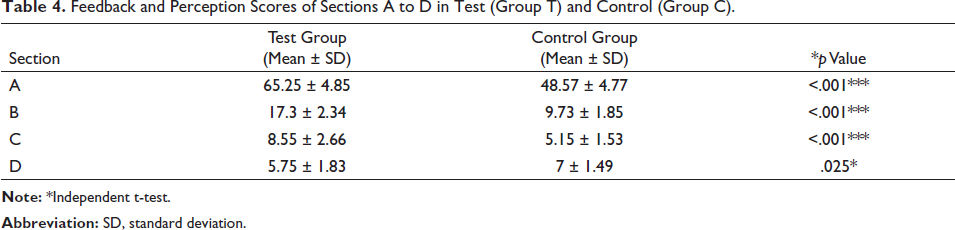
Students in the test group said learning from virtual patients and remembering new information was easier, according to Section A (Understanding and Sustaining Knowledge). The correct medicine selection and upkeep of pharmacological knowledge were made easier by VHFM. Additionally, they firmly agreed that they knew more about how to treat patients than the students in the control group. The VHFM group outperformed the tutorial group in terms of patient learning methodology, clinical management abilities, and actions to be implemented in various clinical settings (p <.001).
Section B (Ease of Learning): Students noticed that using virtual reality and mannequin-based learning significantly and effectively facilitated their learning. The majority of respondents said that VHFM were a good tool to continue medical education and that they should be used to teach pharmacology as well (p <.001).
Students preferred VHFM-based learning over tutorials for theoretical learning and portrayal of instances they are likely to meet in clinical practise, according to Section C (Validity of Learning). Compared to actual patients in clinical practise, less than one-third of students believed that virtual cases were too ideal and had doubts about the therapy (p <.001).
Students in the tutorial group judged the instances to be less intelligible and time-consuming than those in the VHFM group in Section D (Learning Difficulties). Students in both groups might also talk to the staff about their issues. The VHFM-based learning is generally more motivating and less challenging (p <.05).
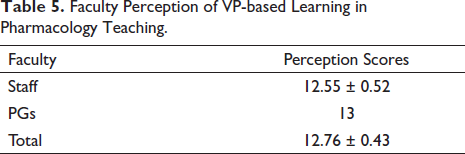
The faculty firmly believed that VHFM-based learning is more motivating, provided several opportunities for student participation, and allotted enough time for debate. Four staff members disagreed that students should study or revise prior to the sessions. Students should prepare for the sessions, according to all postgraduate students. Faculty are strongly encouraged to adopt VHFM-based learning in the pharmacology department in the future, in addition to more conventional teaching-learning techniques (Table 5).
Faculty Perception of VP-based Learning in Pharmacology Teaching.
Discussion
The goal of the current study was to determine how medical students would respond to the addition of virtual reality and high-fidelity mannequin-based learning to regular classroom instruction during pharmacology courses. This intervention’s effects on learning results, student satisfaction, and attitudes were examined and contrasted with those of conventional tutorials. The MCQs on the pre-test and post-test were designed to gauge knowledge analysis and application rather than just simple recall. The questions were specifically designed with a lead-in question, four homogenous options, and a clinical scenario to contextualise the information. By administering another test a month following the final session, the effect of the intervention was also investigated. The superior performance on all post-tests and retest scores is evidence that using VHFM has positive impacts on the acquisition and application of knowledge, according to the results of the current study.
The cornerstone of medical education has historically included both didactic instruction in the classroom and practical training in a clinical setting. By integrating the learner in challenging and engaging tasks that aid in the resolution of clinical problems, case-based learning and problem-based learning are recently gaining popularity. Right now, the VP and mannequin-based simulation approach is used in the most cutting-edge and effective computer-assisted learning techniques.7, 15 This type of simulation is becoming more popular since it makes the learning process easier by providing a safe and regulated setting that helps increase the trainee’s confidence in their clinical skills. A restriction with real-life patients is that it cannot be repeated more than a few times without injuring the patient, but it can offer an immersive learning environment. 23 Numerous studies have demonstrated that students believe virtual patients are useful in facilitating their learning.24–27
Despite the small number of experimental research looking at the efficacy of VPs, the results of this study are similar to those from earlier virtual reality investigations. These results are both encouraging and favourable. The virtual reality studies showed larger effects than lectures, group discussions, and hands-on training with low fidelity mannequins.23, 28, 29 The combination of virtual patients and traditional education was preferred over traditional education alone, according to a meta-analysis. It demonstrated that knowledge and skills like clinical reasoning, procedures, and team skills may be improved more successfully when using virtual patients.8, 23 Lower-achieving students gain more from virtual patients than high achievers, according to Qayumi et al. 30 Oliven et al. discovered that the dependability of the virtual patient OSCE was consistently higher than that of the traditional OSCE, supporting the idea that the VP system can be ued as a practise tool for both training and OSCE examination. 31
A study carried out by Dalfi et al. investigated how professors and students felt about VP. The study indicated that although virtual reality experiences are more engaging than traditional ones and aid in the practise of clinical decision-making, they cannot be compared to training with actual patients. 32 Rather than replacing current medical education, real patient contact should be supplemented by the use of virtual patients. 33 Similar outcomes were observed in our study, where faculty unanimously acknowledged that VHFM-based education is more effective. According to the results of our retest, visual presentation of the content improved knowledge retention more than passive learning did. These findings are consistent with those of a recent study. 34 Therefore, it is crucial to include cutting-edge teaching techniques that support long-term memory retention, like active and integrated learning.
On the contrary, a study raised questions about how using virtual patients in class could make students less empathic learners. 35 Additionally, creating a virtual design takes time and effort and requires even the most basic IT support and knowledge. 32 Most importantly, their design, authenticity, and implementation must be satisfactory. It is more expensive than traditional schooling to develop a virtual curriculum, acquire mannequin hardware and software, acquire high-resolution monitors, and so on, as well as to maintain and set aside room for high-fidelity mannequin and software technologies. The cost increases with increasing fidelity. 36 The fact that this study only looked at one cohort of Phase 2 medical students means that its findings might not apply to other students. Some students may have more favourable opinions about VHFM than others because they volunteered to take part in the study. The inclusion of medical professors from different specializations raises the possibility of selection bias and makes it challenging to compare the results. We limited our research to the pharmacology division. Additionally, the pupils’ empathy wasn’t assessed.
Conclusion
The findings of our study suggest that employing virtual reality high-fidelity mannequin-based simulation as a teaching technique for pharmacology can help students learn at a greater level than traditional teaching due to its active learning engagement, interest, and teamwork. A practical method for clinical simulation and training is virtual reality. They provide a synthetic setting that closely reflects actual circumstances. Therefore, as VHFM learning uses active learning techniques, is student-centered, and offers an interactive learning environment to foster interpersonal, communication, and problem-solving abilities, we would advise implementing it. We strongly advise combining traditional learning methodologies with virtual and mannequin-based simulation in pharmacology training, particularly for clinical reasoning for medical students.
Footnotes
Acknowledgment
The authors acknowledge the support of all faculties and postgraduates of the Department of Pharmacology, KAHER’s JN Medical College, Belagavi, Karnataka, India for the conduct of this study, as well as the staff of the KLE Advanced Simulation Center and Clinical Skill Lab, Belagavi, Karnataka, India for the smooth conduct of this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Ethical Committee (KAHER’s JN Medical College, Belagavi, Ref: MDC/DOME/321; dated: 02/03/2022) Karnataka, India.
Funding
The author received no financial support for the research, authorship and/or publication of this article.
Informed Consent
The participant has consented to the submission of the article to the journal.