
Abstract
Background:
Virtual reality (VR) experiences (through games and virtual environments) are increasingly being used in physical, cognitive, and psychological interventions. However, the impact of VR as an approach to rehabilitation is not fully understood, and its advantages over traditional rehabilitation techniques are yet to be established.
Method:
We present a systematic review which was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). During February and March of 2018, we conducted searches on PubMed (Medline), Virtual Health Library Search Portal databases (BVS), Web of Science (WOS), and Embase for all VR-related publications in the past 4 years (2015, 2016, 2017, and 2018). The keywords used in the search were “neurorehabilitation” AND “Virtual Reality” AND “devices.”
Results:
We summarize the literature which highlights that a range of effective VR approaches are available. Studies identified were conducted with poststroke patients, patients with cerebral palsy, spinal cord injuries, and other pathologies. Healthy populations have been used in the development and testing of VR approaches meant to be used in the future by people with neurological disorders. A range of benefits were associated with VR interventions, including improvement in motor functions, greater community participation, and improved psychological and cognitive function.
Conclusions:
The results from this review provide support for the use of VR as part of a neurorehabilitation program in maximizing recovery.
Introduction
Neurological disorders (characterized by impaired function) affect a significant amount of people worldwide. 1 Such disorders are typically associated with reduced daily function, and a negative impact on quality of life is common. 2
A range of rehabilitation programs may be offered to individuals with such difficulties, to improve abilities in activities of daily living and increase social participation. 3 Such programs are frequently delivered to patients with a range of conditions including patients recovering from stroke, 4 living with cerebral palsy (CP), 5 or spinal cord injury (SCI). 6
It has been suggested that traditional therapy is not without limitations in aiding recovery, and that more radical approaches are much needed. 7 Stasieńko and Sarzyńska-Długosz, 8 for example, report that constant repetition of the same movements will result in the patient being less engaged and resistant to treatment, which will affect involvement in exercise and ultimately reduce effectiveness of the therapy. The success of many conventional therapy treatment plans requires both attendance at treatment sessions and adherence to exercises that are to be completed. The majority of activity required is unsupervised and in the individual’s own time. A paucity of studies has sought to establish how therapists can optimize on adherence to prescribed exercises and physical activity guidelines. 9
It is reasonably well-established that the rehabilitation process can become unnecessarily prolonged if the patient loses interest and if there is a paucity of human and technological resources. 3 In this context, combining traditional rehabilitation techniques with the use of new technologies (eg, robotics, brain-computer interfaces, noninvasive brain stimulators, neuroprostheses, and wearable devices for movement analysis) may positively impact on rehabilitation of cognitive and motor functions.3,10 However, there may be obvious barriers in terms of additional costs, access, and usability of such technology which means that rehabilitation teams may not ultimately adopt such approaches.
An intriguing (emerging) and novel possibility for rehabilitation of neurological disorders in individuals may lie in the use of virtual reality (VR).
Virtual reality is essentially a way for humans to visually connect with, manipulate, and interact with computers.11,12 Virtual reality can be seen as an advanced form of human-computer interaction that allows users to become immersed within synthetic computer-generated virtual environments. 13 The creation of an engaged VR user experience can be accomplished using combinations of a wide variety of interaction devices, sensory display systems, and content presented in the virtual environment.
Virtual reality can be a totally immersive experience in computer-generated environments with 3-dimensional (3D) images or objects. In VR paradigms, participants can explore with a perception of reality. 14 We therefore note that the demand characteristics of such VR settings can facilitate the activities required by rehabilitation programs, but as part of a more engaging experience. 15 The VR-based experimental approaches have been found to offer advantages for individuals with severe motor impairment, 16 and studies have demonstrated improved motivation. 17
In considering the VR characteristics of current systems and how these systems may be useful in engaging patients, studies have indicated that VR provides the possibility of creating real 3D environments capable of eliciting realistic perceptions and reactions in the patient, whereas the observer may monitor and record the performance of the proposed task, allowing the progress of the patient to be tracked and further developed. 3
A number of systematic reviews provide evidence of the positive benefits of such systems. Smith, 18 for example, provides a summary of the positive effects on physical functioning and motivational aspects in older adults. Benefits have also been reported in reviews with patients poststroke, in terms of functional recovery of the upper extremities,19–21 and in increasing mobility and quality of life in individuals living with Parkinson disease (PD). 22 However, the impact of VR-based approaches on recovery is not fully understood and its advantages compared with traditional neurorehabilitation methods have not yet been established.20,23
With the above literature in mind, our group conducted review studies using VR with focus on (1) which mechanism of injury, illness, or disease has been most commonly used/sampled in investigating VR treatment; (2) how VR has been applied; (3) potential benefits; and (4) limits of the procedures available in the use of VR in neurorehabilitation programs.
Methods
Search strategy
A systematic search was conducted in March 2018 of published articles available on PubMed (Medline), Virtual Health Library Search Portal databases (BVS), Web of Science (WOS), and Embase.
Virtual reality is a rapidly developing and novel field. To maintain focus on more recent studies, we limited searches to studies published in the past 4 years (2015, 2016, 2017, and 2018). The review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 24 The use of checklists of the kind offered in PRISMA improves the reporting quality of systematic reviews and provides substantial transparency in the article selection process.25–27 The search was undertaken using the keywords “neurorehabilitation” AND “Virtual Reality” AND “devices” (Table 1). Applicable articles were identified through screening reference lists of relevant articles.
Search methods for identification of studies in databases.

To select the articles, we used 3 steps. The first step was looking for articles in databases and reading the titles and abstracts. The second step was the exclusion of works using the title or abstract and inclusion criteria analysis. The third and final step was to analyze the full text of the eligible works.23,27,28
Inclusion criteria
Studies were eligible for inclusion if they were written in English. Only studies that included technology devices for evaluation or rehabilitation were accepted.
Exclusion criteria
Review articles, meta-analyses, and editorials were excluded, and published clinical trial protocols were also excluded as they do not provide data for analysis.
Study selection
Studies published in English were eligible if they met the following criteria: (1) analysis of VR devices and (2) discussion of/ evaluation of neurorehabilitation treatments. There were no restrictions regarding sample size. Articles were excluded if they (1) were not databased (eg, books, theoretical papers, or secondary reviews), (2) were not in the English language, (3) studies that did not explicitly identify neurorehabilitation, (4) did not emphasize VR devices as therapeutic intervention, or (5) the studies were not published in the past 4 years (2015, 2016, 2017, and 2018). We pooled statistical data from quantitative studies within meta-analyses.
After the removal of duplicates, 3 authors evaluated titles, abstracts, and the inclusion criteria independently. All identified studies were collected in EndNote Web (Thomson Reuters).
Results
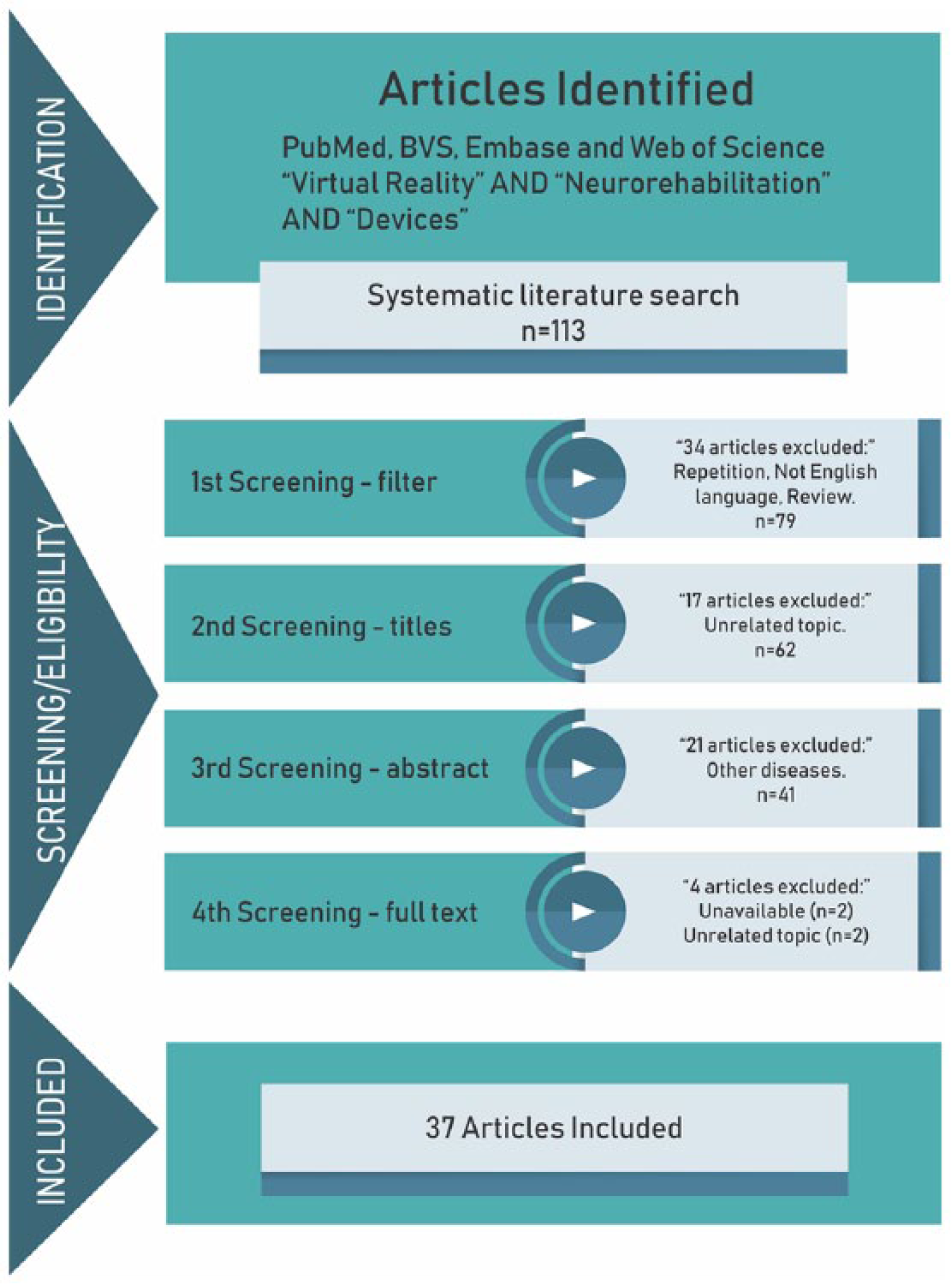
The initial search strategy yielded 113 references (including duplicates) from the 4 electronic databases. After duplicates were removed, 79 references were assessed by 2 authors. Based on titles and abstracts, 41 manuscripts were considered relevant and the full texts were analyzed. The search results are shown in Figure 1.
Procedures for determination of eligibility.
A summary of characteristics of included studies is presented in Tables 2 and 3.
Characteristics of included studies ordered by pathology most investigated.

Abbreviations: BCI, Brain Computer Interface, EEG, electroencephalography, PD, Parkinson disease; VR, virtual reality.
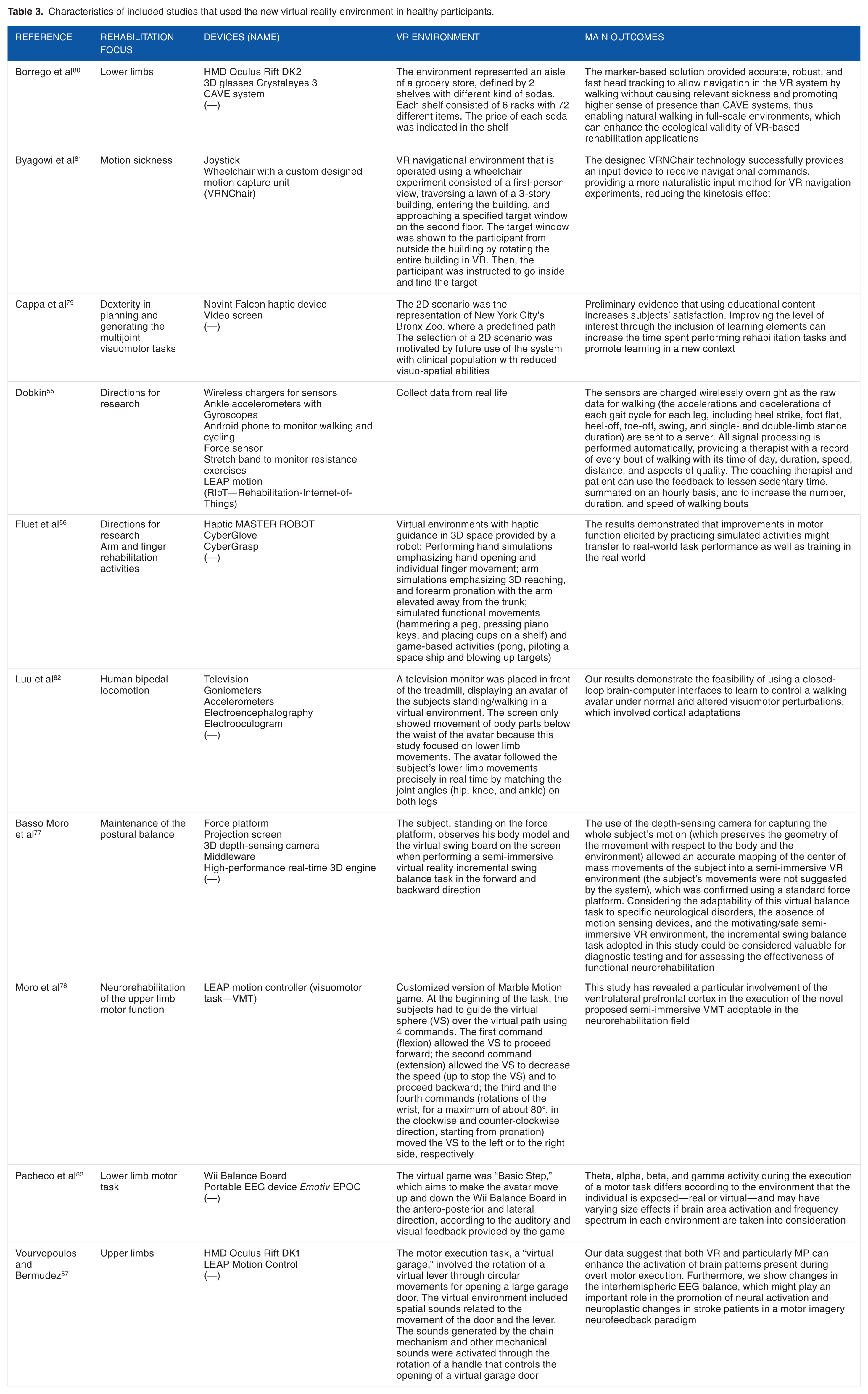
Characteristics of included studies that used the new virtual reality environment in healthy participants.
Discussion
Rehabilitation programs are increasingly using VR environments to simulate natural events and social interactions. Bohil et al 58 show that VR creates interactive, multimodal sensory stimuli that offer unique advantages over other approaches in research and clinical practice. Our results show that several studies have demonstrated the effectiveness of VR in therapeutic interventions even considering 8 studies that selected healthy participants to explore the efficacy of innovative devices to contribute toward the neurorehabilitation field. To understand how practices using VR are being implemented and their contributions to the neurorehabilitation field, we present our discussion focussed on in the available studies according to (1) which mechanism of injury, illness, or disease has been most commonly used/sampled in investigating VR treatment-(populations investigated); (2) how VR has been applied; (3) potential benefits; and (4) limits of the procedures available in the use of VR in neurorehabilitation programs.
Populations investigated
Studies have investigated populations with stroke, CP, and SCI, among other diseases. Most of the studies presented were performed with poststroke patients.14,29–36,38–42,46,56,57,59 We hypothesize that stroke has been predominantly investigated due to the high incidence of this disease in developed countries (affecting 1/500 individuals every year). Most of the studies which explore the use of VR evaluated its effectiveness in facilitating improvement of upper-limb function.
After stroke, CP was the most studied neurological disorder in VR rehabilitation. Four studies identified in our review have explored the effectiveness of VR in individuals with CP using immersive VR, 44 nonimmersive VR, 43 and dedicated devices, such as robotics.45,46 Similarly, to its use with stroke patients, VR was used only for upper limbs rehabilitation, demonstrating positive results for individuals with CP, promoting motor learning and improvement in performance for both immersive and nonimmersive environments. However, we note here the work of Zoccolillo et al 43 who found that although the VR improved the quantity of movements of upper limbs, the quality of hands and finger movements improved more in the real environment, ie, using conventional rehabilitation.
de Mello Monteiro et al 60 similarly report findings from a cross-sectional randomized study evaluating transfer of motor learning from virtual to natural environments in individuals with CP. The authors showed that these individuals improved performance in virtual and natural environments; however, there was no transfer of learning between environments and their performance was less accurate in an abstract task than in the more real task, thus a rehabilitation team should be careful in implementing virtual environments when attempting to enhance motor functioning of individuals with CP.
Not all studies align in these findings however. A recent meta-analysis 61 showed that VR rehabilitation programs focused on motor control, balance, gait, and strength are, overall, more effective than traditional rehabilitation programs. The authors speculated that this may be due to the excitement, physical fidelity, and cognitive fidelity provided by the virtual environment. Moreover, another review and meta-analysis that assessed the effectiveness of VR in children with CP demonstrated that VR is a viable intervention in improving arm function, gait, and postural control. The authors also emphasize that the repetition of therapeutic exercises should be performed in the VR home environment to maximize the positive benefits of intervention. 62
The third neurological disease most studied was SCI. Two studies have focused on this population. One of the studies demonstrated a new and interesting approach in reproducing lower-limb somatosensory feedback in paraplegics, in restoring a full lower-limb perceptual experience in patients with SCI. They provide feedback integrated with an immersive VR environment where a 3D human avatar was simulated. The authors reported some positive sensation from participants. The second study looked at the patient’s functional performance through the use of a glove, with a training based on functional range movements in a virtual environment. 48 Training of people with SCI is demonstrated based on functional reaching movements in a virtual environment using a data glove.
Among the remaining studies of VR in neurorehabilitation, some pathologies are only recently being explored, probably due to the lower incidence of these pathologies and greater difficulty in recruiting populations given the heterogeneous nature of impairments these groups present with.
In relation to multiple sclerosis, the study we identified focused on the performance of this population walking in complex conditions. The participants walked on a treadmill while watching a VR environment representing a wooded trail. The subjects were encouraged to pass obstacles (puddles and trunks) appearing on the trail. The authors concluded that the treadmill training program is feasible and safe for training of gait with obstacles in individuals with multiple sclerosis. 52
In PD, independence related to gait in individuals with PD was focused on and the authors demonstrated that the patients with PD were able to use the immersive VR during the walk successfully and without adverse effects. 49
Participants with ataxia were evaluated with a VR tool developed for assessing impaired coordination and monitoring progression over time. 53 In another study of coordination disorders, the participants performed rehabilitation sessions focused on grasping and reaching tasks with pronation/supination of the hand. The authors report positive results in a prolonged rehabilitation treatment, which usually is necessary in this population. 44 Four further studies are addressed: autosomal recessive spastic ataxia of Charlevoix-Saguenay, focal epilepsy, attention deficit hyperactivity disorder (ADHD), and dyslexia. These studies focused on the cognitive aspects of neurorehabilitation and have indicated the effectiveness of devices used during the VR interventions for evaluating and monitoring upper limb impairment, in particular impaired coordination, 53 for training cognitive abilities 54 and for promoting attention in a motivating and engaging environment.50,51
How VR has been applied
From our review, we note that VR can be considered a computer technology that provides 3D artificial sensory feedback, whereby the user engages in experiences similar to real-life activities and events. Commercial games have some limitations, for example, the calibration of a game’s difficulty is conducted with healthy players and does not consider individuals with disabilities. In studies of the commercial games currently available, a rehabilitation team might often rely on adapted versions of the game to improve performance. 63 In considering the work by Crocetta et al, 63 we advocate that the development of platforms with tasks that are adapted to the needs of people with disabilities is the future of the use of VR in rehabilitation. It is certainly the case that research involving specific platforms for rehabilitation should be developed that would consider user experience (the kind of experience the games create for the individual who uses it how virtual experience then informs specific skill sets in the real world). 64 Indeed, engagement with online communities, including a community of people with neurological diseases, would depend on the usability and adaptability of platforms for games (see the work by Crossley et al 64 ). We therefore consider that the factors that can influence user experience should be carefully observed when designing games.
It is difficult to extrapolate directions that innovative hardware of the future may take for people with neurological disorders. Virtual reality is an emergent technology that is still being constructed and expanded on by science and research. However, this work has given an overview of how scientists and researchers are working toward development of new devices that address the needs of this population. Studies have pointed out relevant and strategic approaches that attest to how future advances may support the development of innovative devices that are more specifically effective for this population.
In considering the work by Pichierri et al, 65 VR can result in an optimal solution for the rehabilitation of cognitive and motor functions and we note that VR interactive devices are precious tools in the process of inclusion and actual interfacing with people with some type of disability.
The potential benefits reported in the current literature are commonly noted in a context where VR devices have been customized for people with neurological disabilities. To this extent, we advocate that it would be important to increase accessibility to this technology through developing and maintaining low-cost products on the market. According to Crocetta et al, 63 there are different VR devices that can be efficiently used to provide the user with greater control over the VR experience and associated actions through a remote input device, such as a keyboard or a mouse,32,63 or by more advanced VR devices such as a Kinect sensor, special gloves, 66 and new hardware that may be adapted to provide a patient-compatible controller that supports arm movements in different game scenarios with an integrated audiovisual interface. 46 It is important to emphasize that because each VR device has a potential function, a multidisciplinary evaluation of each person’s needs is important to provide a functional interaction and identify the best bespoke device. 55
Potential benefits
Several benefits were widely reported in relation to motor function: upper limb and postacute treatment beyond the initial period of hospitalization and rehabilitation, improvement in balance and gait,31,42 neuromotor monitoring of recovery, 39 improvement of strength fitness, 67 skills, 68 improvement in the range of movement of shoulder and reduction in spasticity, 38 and also the improvement of the levels of participation in both domestic and community environments. 38 Furthermore, there were psychological and cognitive benefits reported when the VR device is adapted to the patient, such as improvement in attention, or memory stimulation and decrease in depression symptomology in elderly participants. This was evident even several years after stroke.14,29,33,36 Therefore, VR devices could be used as effective tool to motivate patients during rehabilitation sessions, 41 to improve spatial orientation and attention in daily life activities, 59 and to improve pain relief scores and emotional aspects related to functionality. 36
Additional benefits of using VR environments in neurological rehabilitation were also reported, such as safety/security, multitask possibilities, patient’s adherence, and lower cost. According to Lange et al, 69 a real and safe VR training environment will provide subjects with task-specific training, accurate sensory and tactile feedback, and motivation. Furthermore, to develop an individualized rehabilitation program targeted to different dysfunctions, and to keep patient’s interests, an active participation can be achieved using telerehabilitation, which can be remotely controlled by the therapist and can cost significantly less compared with traditional face-to-face interventions.29,32,55
Moreover, Saposnik et al, 37 comparing real intervention (simple recreational activities, eg, play cards and ball game) and nonimmersive VR intervention (Nintendo Wii gaming system) in a randomized, multicenter, single-blind, controlled trial with poststroke patients, reported that both interventions provide improvement and benefits to participants. However, they emphasized that combined therapy (real and VR) presented better outcomes. These results align with Aminov et al 70 who also emphasized that the use of combined therapy is effective in patients with neurological disorders.
Regarding children, more research is clearly needed, and we are yet to understand whether VR holds any implications for brain development. Keller et al 46 report that VR is an excellent way of offering optimal challenges to children and adolescents with severe-to-moderate arm motor function difficulties. Pulay 71 demonstrate that eye-tracking and EMG-supported 3D VR combination devices worked well in terms of efficiency in children with spastic tetraparesis. Again, the accessible environment that is motivating will reportedly empower children with disabilities to take an active role in their rehabilitation. 72 It is important to also highlight (as in Table 2) the use of eye trackers, which are expected to become popular in near future. 47 The manufacturers are hoping to be able to create high-resolution, foveated (level-of-detail) rendering, thus increasing the realism of VR environments with less hardware power. This general trend is expected to increase utility in increasing medical applications with development of pervasive eye-tracking VR headsets, expanding the number of developers available who may be familiar with integrating eye tracking with VR.
It is also important to note how the use of VR applications in the future may benefit from larger pooled automated data and artificial intelligence. For example, if eye trackers become a standard feature of VR in every headset, this could generate data from healthy controls and individuals with disability. This may be to the effect that results may allow for equality of performance, where people with disabilities could interact competitively with people with typical development—we advocate that this should be further explored in future studies.
Limitations
Despite the increasing enthusiasm for VR, and evidence of its use in clinical applications, the recent literature has highlighted some limitations:
In the work by Lin et al, 34 preliminary tests were conducted to assess the feasibility of the developed haptic rehabilitation system and they identified design concerns that should be considered regarding the practical use in future clinical testing.
In addition, the use of immersive and semi-immersive VR can and does cause unwanted effects, and typical symptoms such as sickness, dizziness, headache, nausea, and vomiting are frequently reported. 73 From our own VR experience, we consider that it could be due to the visual perception of movement and motion while the person is still. The mixed messages on the brain can cause a “motion sickness” effect. This needs careful consideration where there may be vestibular effects of injury. We have found that computers with increased processing capacity that enable smoother visual experiences can minimize such motion sickness effects, but more research is needed here. This paired with the fact that some devices are already considered expensive and may need some specific training to use 74 and can be considered as a technology or marked limitation.
There are many elements to be considered in discussing limiting factors that prevent mainstream VR applications being sufficient for neurorehabilitation purposes. The literature has highlighted that VR for neurorehabilitation can provide modern tools for increasing efficiency. However, despite the full potential of VR approaches, the technology is in early development and there is further development needed before this technology can be fully integrated into the routine rehabilitation. 75 We consider that VR should be used only as a tool in the hands of neurorehabilitation teams or therapists in the framework of a rehabilitative program and not as a rehabilitative approach per se. Therefore, VR should be used to boost certain specific aspects of rehabilitation such us intensity, participation, engagement, and feedback, but here we recognize that we need more studies to establish generalizability of benefits.
New technological devices and some applications for computers and mobile phone (different start-ups created specific tasks) have been commercialized despite the lack of a clear proof of their effectiveness and/or a clear definition of user guidelines. 76 Public policies that ensure scientific scrutiny of this new technology should be in place to protect the interests of individuals with disability. According to Morone et al, 76 it is important to establish proof of the effectiveness of VR and to generate clearly defined user guidelines before new devices are made available commercially.
From a financial perspective, the high cost of new VR technology needs to be considered as a limitation. For this reason, video game–based therapy and nonimmersive VR systems are playing an important role in cost-effective rehabilitation. Cost-saving approaches include using commercial gaming systems and augmenting the involvement of patients’ attention and participation to the exercise/game. 75
As a limitation of this review, it is important to acknowledge that our interpretation of the studies was directed at VR use in rehabilitation team settings, and so our specific interpretation focused on the development and technological engineering and software development that may be developed in future work.
Final considerations
The results from this review provide evidence that VR can and does have beneficial effects on rehabilitation of patients with neurological disorders. In our view, future developments in VR will lead to improved motor, psychological, and cognitive functions in this population and are likely to be an increasingly important option to complement traditional therapies. Based on our findings, we advocate for the relevance of innovative, functional, and interactive VR devices and the importance of availability and accessibility for individuals with neurological disorders. Moreover, we emphasize the need for studies that prove the effectiveness of existing technologies and greater scientific support for future proposals.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/ or publication of this article: This work was supported by the Brazilian agency CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico) process number 442456/2016-6 and 8887.091039/2014-01.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
TM structured the script and directed the work; TM, TDS and TBC performed the data collection and organized the data; RG and BLF performed the data collection and organized the data; The PBL structured the method and data analysis; SW and JT structured the discussion and conclusion; TM and TDS performed the data analysis and assembled the results work; PBL and JT adapted the work to the English language; SW and TM helped build the discussion; The CBMM reviewed and organized the manuscript in general.