
Abstract
Objectives:
To compare the serum vitamin D and serum cathelicidin antimicrobial peptide (CAMP) levels among tuberculosis patients and healthy subjects and to determine the association between serum vitamin D and cathelicidin in tuberculosis.
Materials and Methods:
This is a case-control study carried out at the pulmonary medicine and pediatrics departments of a tertiary care hospital in Chengalpattu. The study included 180 tuberculosis cases and 90 control subjects of both sexes between the age group of 1 to 80 years. Serum was used to estimate vitamin D and CAMP. The study was analyzed using SPSS version 21 (IBM Corp. Armonk, New York). The results were evaluated using the chi-square test at a 95% confidence interval, and P value <.05 was considered highly significant.
Results:
This study observed vitamin D deficiency, vitamin D insufficiency, and optimum vitamin D among 55%, 41%, and 3.89% tuberculosis cases, respectively. Similarly, vitamin D deficiency, vitamin D insufficiency, and optimum vitamin D were seen in 40%, 50%, and 10% healthy controls, respectively.
Conclusion:
This study found no association between serum vitamin D and serum CAMP levels in tuberculosis patients and healthy controls.
Introduction
Tuberculosis (TB) is the world’s deadliest chronic granulomatous disease and the second most important infectious killer disease. It mostly affects the lungs and can affect organs, such as the abdomen, urogenital system, glands, lymph nodes, bones, blood, and the central nervous system. The incidence of TB cases in India was 2.59 million cases, according to the WHO report 2021. 1 In 2020, India is first among eight high-burden TB countries, which account for two-thirds of the new TB cases. 2 Vitamin D is a sunshine vitamin, and its main role is associated with bone homeostasis. Recent research studies have reported the role of vitamin D in the prevention and treatment of a variety of disorders, like cancer, cardiovascular diseases, autoimmune diseases, infectious diseases, and diabetes mellitus. 3 Vitamin D is an immunomodulator that exerts innate and adaptive immunity and helps to combat TB.4–6 It produces cathelicidin antimicrobial peptides (CAMP) or LL-37, which are the first-line defensins against invading microorganisms, thereby protecting the body against TB.4, 7 They are expressed in epithelial cells of the testis, skin, the gastrointestinal tract, the respiratory tract, and in leukocytes, such as monocytes, neutrophils, T cells, NK cells, and B cells. 8 Increased CAMP expression is seen in macrophages by optimum levels of vitamin D, which causes damage to the tubercle bacilli and eventually results in autophagy.9–11 The antimicrobial and immunomodulatory properties of human LL-37 are dependent on vitamin D status. A decreased growth rate of Mtb was seen in the macrophages treated with vitamin D, proving that vitamin D has immunity against TB, which was proved way back in 1836. 12 In vitro studies have also shown that vitamin D deficiency acts as a risk factor for the development of TB by modifying immunomodulatory effects of vitamin D.4, 12–15 A study demonstrated that vitamin D insufficiency inhibits the induction of the CAMP gene, which subsequently leads to decreased LL-37 expression. 16 However, other studies have failed to demonstrate the association between vitamin D status and LL-37 in TB. In India, the association between serum vitamin D and serum CAMP levels among TB patients and control subjects has not been carried out till date. Thus, the objective of the present study is to compare serum vitamin D and CAMP levels among TB patients and controls and to determine the association between serum vitamin D and LL-37 among the two study groups.
Materials and Methods
Study Population
The present study screened 410 study subjects and after considering inclusion and exclusion criteria, the study included 180 TB cases and 90 control subjects of both sexes between the age group of 1 to 80 years. Patients from the Departments of Paediatrics and Pulmonology, SRM Medical College Hospital and Research Centre were enrolled as a case group, and adults working within SRM university campus were enrolled as an adult control group in the present study. Pediatric control subjects were chosen from in and around the Potheri and Kattankulathur areas. For each subject, all demographic and anthropometric details, sunlight exposure, monthly income, skin color, diet pattern, and living condition were collected using a preformed proforma. Acid fast staining for sputum, Mantoux test, chest X-ray, and other blood investigations were carried out to confirm the cause of TB.
Study participants were informed about the nature and purpose of the present study and written informed consent was obtained. The Scientific Committee and Institutional Ethical Committee clearance (913A/IEC/2015) was obtained before starting the study.
Inclusion Criteria
Patients of both genders aged between 1 and 80 yr and registered under DOTS at SRM MCH & RC were included. Subjects who were not having TB acted as control.
Exclusion Criteria
TB patients infected with HIV or with a history of seizures or taking drugs phenobarbitone, phenytoin, orlistat, corticosteroids, cholestyramine, statins, and thiazide diuretics were not included in the study. Pregnant patients were also excluded.
Study Design
The present study was a case-control study carried out at a tertiary care teaching hospital in Chengalpattu from January 2016 for a period of 15 months. About 3 mL of venous blood was collected from each subject, and serum was separated to estimate vitamin D and cathelicidin.
Estimation of Serum Vitamin D
It was done using the chemiluminescent microparticle immunoassay with an Architect 25-OH vitamin D assay kit.
Estimation of Serum CAMP Level
It was estimated using quantitative sandwich enzyme immunoassay technique with a Blue gene kit.
Sample Size Calculation
Sample size was calculated using PS power and sample size calculation software version 3.1. Keeping α = 0.05, power = 0.8, the probability of exposure in controls = 0.82, m = the ratio of control to cases 0.5, and β = 3.1 showed a sample size of 183 cases and 91 controls obtained from a pilot study.
Statistical Analysis
In the present study, serum vitamin D and serum cathelicidin anti-microbial levels were expressed in numbers and percentage. Serum vitamin D levels and serum CAMP levels were compared among TB patients and controls using the chi-square test at a 95% confidence interval, and a P value <.05 was considered statistically significant. SPSS version 21 was used for the statistical analysis.
Results
In this study, mean vitamin D levels in TB cases and healthy controls were 16.56 ng/mL and 21.59 ng/mL, respectively. In the present study, vitamin D deficiency, vitamin D insufficiency, and optimum vitamin D levels were seen in 55%, 41%, and 3.89% of cases, respectively. Among healthy controls, 40%, 50%, and 10% had vitamin D deficiency, vitamin D insufficiency, and normal levels of vitamin D in the serum, respectively. Among TB cases, 96% had below optimum vitamin D levels compared to 90% in healthy controls. Both mean vitamin D levels and optimum serum vitamin D levels were lower in TB cases compared to controls.
Comparison of Vitamin D Status and Serum CAMP Among Study Population.
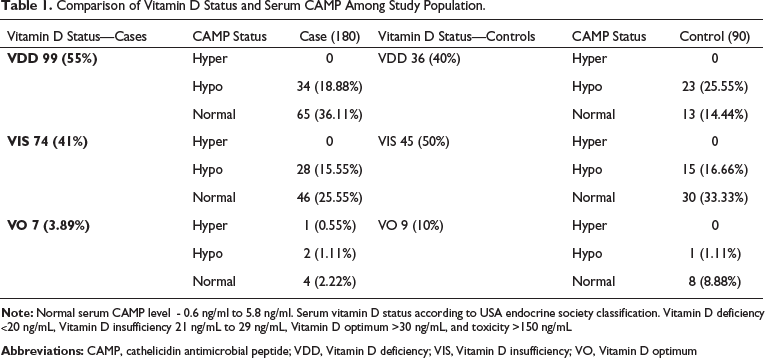
Among 55% vitamin-D-deficient cases, 36.11% had optimum cathelicidin levels when compared to 40% vitamin-D-deficient controls, who had 14.44% normal cathelicidin levels. Among 41% vitamin-D-insufficient cases, 25.55% had normal cathelicidin levels compared to 50% vitamin-D-insufficient controls, who had 33.33% normal cathelicidin levels. Among 3.89% optimum vitamin D cases, 2.22% had normal cathelicidin levels, and among 10% optimum vitamin D controls, 8.88% had normal vitamin D levels. This study showed that even though there was vitamin D deficiency and insufficiency among cases and controls, normal cathelicidin levels were observed.
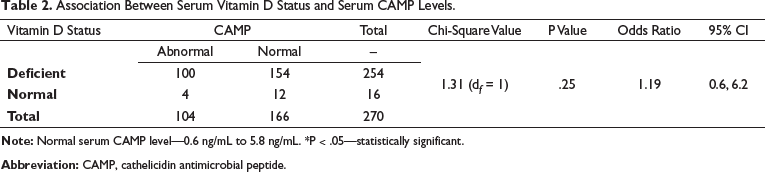
Association Between Serum Vitamin D Status and Serum CAMP Levels
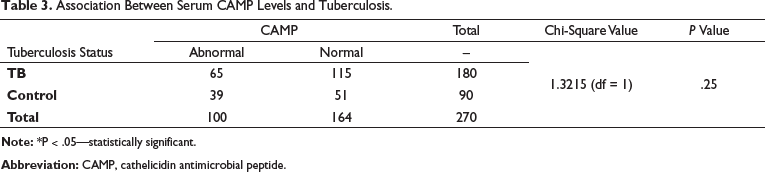
Association Between Serum CAMP Levels and Tuberculosis.
Discussion
Vitamin D is a fat-soluble vitamin that acts as an immune modulator against infectious diseases. Vitamin D inhibits the growth of microorganisms, like Staphylococcus aureus, Streptococcus pyogenes, Klebsiella pneumonia, and E. coli, as reported in some of the in vitro studies. 17 Cod liver oil has a large amount of vitamin D and was used as a treatment for TB before antibiotic usage. 18 It is evident from previous studies that there is a definite link between vitamin D and TB disease. Literature review says that vitamin D deficiency poses a risk for the development of TB infection and disease. The present study showed lower levels of mean serum vitamin D among TB cases compared to controls. It also showed that hypovitaminosis D was observed in 96% of TB cases and 90% of healthy controls. A study conducted in Australia among African immigrants also showed that mean vitamin D levels were lower in latent TB patients compared to the control group. 19 A meta-analysis of vitamin D in TB also revealed that vitamin D levels were low in TB patients compared to controls. 10 A cross-sectional study on TB also showed that hypovitaminosis is more among TB cases compared to controls, and it adds to a greater rate of sputum smear positivity, severe clinical symptoms, and larger lesions in the chest X-ray among cases.20, 21 A cohort follow-up study conducted in Pakistan among healthy household contacts reported an association of vitamin D deficiency with TB. 22 A study conducted in Vietnam stressed that hypovitaminosis could be a possible cause of TB. 23 In the present study, vitamin D deficiency was not only predominant among cases, but it was also common in control subjects. Recently, vitamin D deficiency has become very common worldwide. Tropical areas, like Chennai, where there is scorching sun throughout the year, make it very surprising to observe the vitamin D deficiency in this part of the country. Because of an ultramodern lifestyle, indoor stay during the daytime, using sunscreen lotions, lack of vitamin D supplementation, and fortification of food items could be the reasons for vitamin D deficiency. Vitamin D is an immune modulator. It combats Mtb by the production of LL-37, which causes the formation of phagolysosomes. It is clear that vitamin D levels are proportional to CAMP to protect the body against infections. In our study, vitamin-D-deficient and vitamin-insufficient study subjects showed normal serum cathelicidin levels. When study subjects had serum vitamin D levels within the normal range, there was a deficiency of CAMP levels in the serum. It shows that the present study could not find a statistically significant association between serum vitamin D levels and serum CAMP levels among study subjects (Table 3). A study conducted among HIV-positive patients showed a positive correlation between vitamin D and LL-37. 24 A study conducted among healthy subjects showed that serum vitamin D levels ≤ 32 ng/mL had a positive correlation with serum cathelicidin, and when serum vitamin D levels exceeded 32 ng/mL, there was a fall in serum cathelicidin levels. 25 A study conducted among the elderly showed a decreased serum vitamin D and an associated fall in serum cathelicidin levels. 26 A study on neonates and mothers could not find an association between serum vitamin D and LL-37 in the cord blood, which supports the present study. 27 Among critically ill patients with sepsis, there was a positive correlation between serum levels of vitamin D and LL-37 compared to healthy subjects. 28 Some studies have shown that vitamin D considerably increases serum cathelicidin levels and helps to improve the clinical outcomes of TB, which is contradictory to the present study.29, 30 The present study found no association between serum CAMP levels and TB (Table 3). Our study could not find an association between serum vitamin D levels and serum cathelicidin or between serum cathelicidin and TB. There was no association between serum vitamin D levels, serum cathelicidin levels, and TB. A meta-analysis and systematic review reported hypovitaminosis D in TB cases with raised circulatory cathelicidin levels. 31 A prospective Canadian study found an association between serum concentrations of 25 hydroxyvitamin D levels (25(OH)D) and LL-37, and the study also revealed that there was a decrease in LL-37 concentrations following vitamin D supplementation. Also, this study could not find any association between serum 25(OH)D and LL-37, which is in agreement with our study results in TB patients. 32 A meta-analysis reported that serum vitamin D levels ≤25 nmol/L are associated with a high risk for TB disease. 33 In a cross-sectional study conducted in Pondicherry, there was an inverse relation between serum vitamin D levels and bacterial load among active pulmonary TB cases. 34 A systematic review and meta-analysis reported that hypovitaminosis D is a risk factor for developing TB. 35 A South Korean study showed vitamin-D3-induced colocalization of mycobacterial phagosomes with autophagosomes of macrophages mediated through cathelicidin and observed the direct antimycobacterial activity of cathelicidin in TB. 36 A case-control study conducted among pediatric TB patients could not find a correlation between LL-37 and 25(OH)D levels, which is in accordance with the present study. 5 Our findings are in line with a USA study conducted in 95 TB patients, which failed to find an association between vitamin D and serum LL-37 concentrations, similar to the present study results. 37
Strength of the Study
The present study confirms a high percentage of vitamin D deficiency among the study population. It stresses the protective role of vitamin D in various diseases. It is the first study to confirm no association between serum vitamin D levels and serum cathelicidin levels among TB patients in comparison to healthy controls.
Limitations of the Study
In the present study, we evaluated vitamin D status after the diagnosis of active TB disease and were unable to find out the effect of prior vitamin D levels on the probability of TB disease. TB can cause severe metabolic defects, and it is ambiguous whether vitamin D deficiency (VDD) increases the TB disease risk or whether underlying TB infection or disease leads to decreased serum 25(OH)D levels. Hence, it was challenging to come to a conclusion about whether individuals with vitamin D deficiency are at a high risk of TB disease. The smaller sample size of 180 cases and 90 controls was one more limitation in the present study. Future studies designed to be randomized controlled trials with a larger sample size and vitamin D supplementation following will be very much helpful in finding out the association between vitamin D and TB via cathelicidins.
Conclusion
Our findings reveal that there is no association between serum CAMP levels and serum vitamin D levels or TB infection. It has been reported in the literature that cathelicidin is an integral part of innate immunity during infection and the entry of the pathogen into the body causes the synthesis of cathelicidin as a first-line defense mechanism.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.