
Abstract
Objective:
To observe the hemodynamic effects of a single bolus dose of dexmedetomidine in patients undergoing elective laparoscopic surgeries.
Methods:
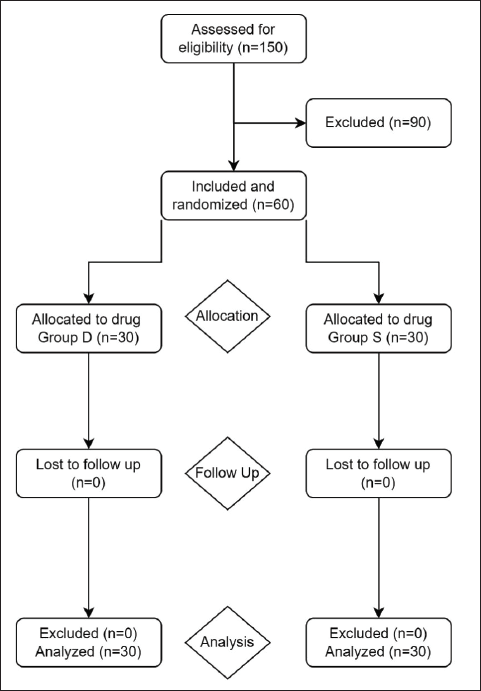
A total of 60 adult patients were randomized into two groups of 30 each. Group D patients were given 1 µg/kg dexmedetomidine in 50 mL of saline as a single-dose infusion over 10 min before induction. Group S patients were given a 50-mL 0.9% NS slow infusion over 10 min. Groups D and S patients were premedicated 10 min prior to surgery. Baseline vital and hemodynamic parameters were monitored during the perioperative period.
Conclusion:
Premedicating with a single bolus of 1 µg/kg IV dexmedetomidine has been proven safe and effective in maintaining perioperative hemodynamic stability, although few developed bradycardia and hypotension, which were managed without any adverse outcome. Furthermore, dexmedetomidine effectively reduced the incidence of shivering.
Introduction
Laparoscopic procedures have improved greatly over the past few years with advances in anesthesia and surgical techniques. They have revolutionized the field of surgery since their introduction in 1950. 1 Laparoscopic techniques offer significant patient benefits, such as trivial incision size with minimized postoperative discomfort, along with a low incidence of postoperative wound infection. 2 Although a large number of beneficial effects have been attributed to laparoscopy, it is known to induce specific pathophysiological changes that may be detrimental to different systems of the body with a variety of hemodynamic changes. 3 Laparoscopic surgeries are performed with added risks, either because of the risks associated with a laparoscopic approach or because of changes in physiology that result in the creation of pneumoperitoneum. Hence, one must anticipate that these differences and anesthetic techniques must be improved. 4 Various anesthetic techniques, such as regional anesthesia and other pharmacological agents, have been used to prevent the above-mentioned changes; however, owing to patients’ discomfort with a high requirement of sedatives, regional anesthesia as a sole anesthetic agent is discouraged. Dexmedetomidine, a selective α -2 adrenergic receptor (α 2-AR), agonist was chosen in this study as a premedicant for laparoscopic surgeries. On the contrary to most pharmacological drugs, dexmedetomidine produces not only a sedative–hypnotic effect, but in situations involving cardiac risk, it also produces analgesic effects and an autonomic blocking effect, by acting on a single type of receptor. Even though side effects, such as bradycardia and hypotension, are frequent, several studies have proven its safety use. Dexmedetomidine has also been proven that on its use, it consistently reduces the requirement of opioids, propofol, and benzodiazepines. 5 In recent years, its use has become an effective therapeutic tool in anesthetic treatment, offering benefits in perioperative management. 6
The current study looks at the effectiveness of 1 µg/kg IV dexmedetomidine in suppressing the pressor response that occurs during laryngoscopy and intubation, as well as the hemodynamic alterations caused by pneumoperitoneum and adverse effects if any.
Materials and Methods
Following the approval by the Ethical Committee, this randomized, prospective, double-blinded, single-hospital study was conducted in the Department of Anaesthesia, Dr. D.Y. Patil Medical College and Research Centre, from August 2019 to September 2021. This study has been registered in the National Clinical Trial Registry of India (
Dexmedetomidine
Dexmedetomidine hydrochloride is an S-enantiomer of medetomidine, and its empirical formula is C13H16N2HCl, with a molecular weight of 236.7. It is a relatively selective α 2-AR agonist, an imidazole derivative with analgesic, anxiolytic, and sedative properties. 7 Dexmedetomidine selectively inhibits the release of norepinepherine (NE) from synaptic vesicles in the brain by binding to α 2-AR found in the presynaptic terminal. The result is a decrease in adrenoceptor postsynaptic activity, which in turn inhibits sympathetic activity, resulting in sedation and anxiolysis. Analgesia is produced by the binding of this agent to α 2-AR in the spinal cord.
Doses of Study Drug
Dexmedetomidine has been used in various dose ranges through various routes in different studies. Lawrence et al. 8 found that the administration of a single bolus of high-dose dexmedetomidine, i.e., at 2 µg/kg, decreased the hemodynamic changes of tracheal intubation as well as extubation, but bradycardia was common during the initial 15 min postadministration of the drug. Geetanjali et al. 9 observed that analgesia requirements were significantly reduced within 24 h in patients who underwent laparoscopic surgeries, as well as pneumoperitoneum-induced hemodynamic changes were effectively reversed at an infusion dose of 0.5 µg/kg. As a high dose of dexmedetomidine, i.e., > 1µg/kg, is associated with more incidence of hypotension and bradycardia, we decided to conduct our study with 1µg/kg in 50-mL saline as a single-dose infusion over 10 min before induction. We enrolled 60 patients belonging to the ASA I and II category, of either sex, who belonged to the age group of 18 to 65 years, and who underwent elective laparoscopic surgeries. Institutional Ethics Committee clearance was obtained before the study was conducted.
Group D—30 cases (1 µg/kg in 50-mL saline as a single-dose slow infusion over 10 min) Group S—30 cases (50-mL 0.9% NS slow infusion over 10 min)
The drug preparation was done by an anesthesiologist, who was not involved in the administration of anesthesia and patient care. The monitoring and data collection were done by another doctor, who was not involved in drug administration. For all the patients undergoing elective laparoscopic surgeries selected for the study, a preoperative visit was conducted on the previous day of surgery and detailed history and complaints were noted. The cardiovascular, respiratory, and central nervous systems were examined in detail. Laboratory investigations, such as a hemogram, liver function tests (LFTs), renal function tests (RFTs), serum electrolytes, urine routine, and bleeding time and clotting time (BT–CT), were performed. Prior to surgery, patients were kept nil by mouth from midnight. Heart rate (HR), noninvasive blood pressure (NIBP), respiratory rate (RR), pulse oximetry (SpO2), and electrocardiography (ECG) were monitored. Peripheral venous access was established with a 20-gauge catheter, and intravenous fluids, such as Ringer’s Lactate, were given according to the Holiday–Segar formula. The study drugs were administered in a double-blind manner according to randomization. Patients were then preoxygenated for 3 min, premedicated with injection glycopyrrolate 0.2 mg, injection midazolam 1 mg, injection fentanyl 2 µg/kg, and then induced with propofol 2 mg/kg, injection vecuronium 0.1 mg/kg body weight. Patients were intubated with an appropriate-sized endotracheal tube, bilateral air entry was confirmed by auscultation, and the tube was then secured. Maintenance of anesthesia was done with air (60%), oxygen (40%), and sevoflurane as required using intermittent positive pressure ventilation. Vitals were monitored throughout the procedure.
The following parameters were assessed by the attending anesthesiologist as signs of inadequate anesthesia and analgesia: increase in heart rate (HR) > 20% above baseline for >1 min and increase in mean arterial pressure (MAP) > 20% above baseline for >1 min. In the presence of two or more parameters, the depth of anesthesia was increased by increasing the flow of sevoflurane by 0.2% and analgesia was supplemented with injection diclofenac 75 mg IV. Atropine, 0.01 mg/kg, and mephenteramine, 6 mg, were administered intravenously to manage bradycardia, that is, HR < 50 bpm, and hypotension, that is, MAP < 60 mmHg. At 1 h into surgery, patients received injection paracetamol 1 g over 30 min IV. Injection ondansetron 4 mg IV was administered during closure. Injection glycopyrrolate 0.008 mg/kg and injection neostigmine 0.05 mg/kg were injected for reversal following suction at the end of surgery. Once patients’ breathing was deemed sufficient and they were able to obey commands, they were extubated. Any adverse events were recorded immediately after surgery, 15 min, 30 min, 45 min, and 60 min postoperatively.
A series of hemodynamic responses were recorded, including HR, systolic blood pressure (SBP), diastolic blood pressure (DBP), MAP at induction, 1 and 5 min after endotracheal intubation, and skin incision followed by pneumoperitoneum for 0 min, 15 min, 30 min, 45 min, and 60 min.
In order to display analytically, the following statistical method was adopted—Continuous variables, such as age, height, weight, HR, MAP, and SpO2, are expressed as Mean ± Standard Deviation and compared across the two groups using the student t-test. Categorical variables, such as adverse effects, are expressed as the number of patients and the percentage of patients having them and compared across the two groups using Pearson’s chi-square test for independence of attributes. The statistical software SPSS version 16 has been used for the analysis. An alpha level of 5% has been taken, i.e., if any P-value is less than 0.05, it is considered significant. The paired t-test is used to compare the two means.
Results
Demographic Profile of Patients
Changes in HRs in Two Groups
Changes in MAP in Two Groups
Discussion
In general surgery, the laparoscopic approach has gained popularity because of its small incisions, faster recovery, and reduced hospital expense. Various hemodynamic alterations are observed during pneumoperitoneum, such as an elevated MAP, a fall in cardiac output, an increase in systemic vascular resistance, which exhibits elevated blood pressure, raised HR, which may compromise the tissue perfusion and alter the acid–base balance. 11 All these factors entail the use of anesthetic drugs for maintaining hemodynamic parameters in order to maintain vital organ perfusion. Modified surgical techniques, such as gasless laparoscopic surgeries, with the use of abdominal elevators and low IAP have been tried with limited success in managing the intraoperative haemodynamics. 12 Various anesthetic techniques, such as regional anesthesia and other pharmacological agents, have been used to prevent the above-mentioned changes. Dexmedetomidine, a selective α 2-AR agonist, was chosen in this study as a premedicant for laparoscopic surgeries. On the contrary to most pharmacological drugs, dexmedetomidine produces not only a sedative–hypnotic effect but also, in situations involving cardiac risk, analgesic effects and an autonomic blocking effect by acting on a single type of receptor. Even though side effects, such as bradycardia and hypotension, are frequent, several studies have proven its safety use. Dexmedetomidine has been proven to consistently reduce the requirement of opioids, propofol, and benzodiazepines. 5 In recent years, its use has become an effective therapeutic tool in anesthetic treatment, offering benefits in perioperative management. 6
Each group of 30 patients was randomly assigned to one of two groups.
Group D—Patients were given injection dexmedetomidine 1 µg/kg 10 min before induction. Group S—Patients were given 0.9% normal saline 10 min before induction.
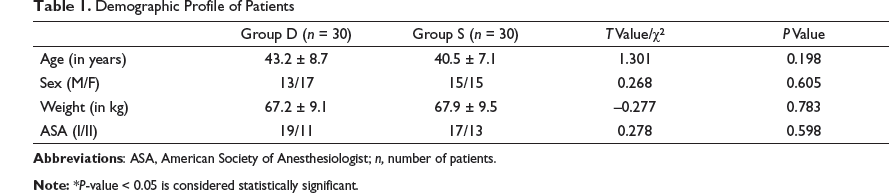
The mean age in group D was 43.2 years, whereas in group S, it was 40.5 years, the P-value was 0.198, and the difference was nonsignificant, as observed from Table 1. The study was female predominant with 17 females in Group D and 15 females in Group S, whereas males were 13 and 15 in Groups D and S, respectively. The comparison between the groups was nonsignificant with a P-value of 0.605, as observed from Table 1. The mean weight in Group D was 67.2 kg, whereas it was 67.9 kg in Group S, the P-value was 0.783, and the difference was nonsignificant, as observed from Table 1. There were 19 and 17 patients with ASA grade I in Group D and Group S, respectively, and 11 and 13 patients with ASA grade II in Group D and Group S, respectively. In 2010, a similar study by Bhattacharjee et al. 13 evaluated the effect of dexmedetomidine on hemodynamics in patients undergoing laparoscopic cholecystectomy, and nonsignificant differences were observed with regards to age, gender, and ASA grading, similar to our study. It is essential to match these factors to determine any confounding factors that can arise and affect the hemodynamic factors. As noted from the above-mentioned data, our study is comparable concerning parameters such as age, gender, weight, and ASA grading, which was similar to studies conducted by other authors, such as Bhattacharjee et al. 13 and Kumar et al. 14
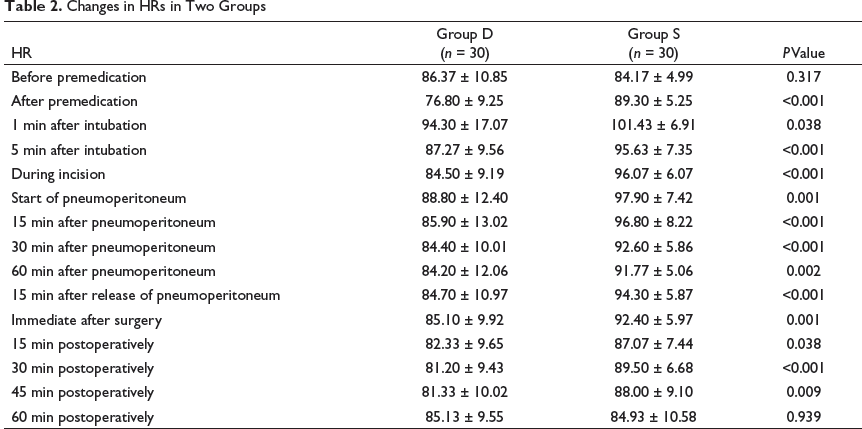
The HR, SBP, DBP, and MAP were measured before premedication, after premedication, 1 min after intubation, 5 min after intubation, during incision, at the start of pneumoperitoneum, 15 min after pneumoperitoneum, 30 min after pneumoperitoneum, 60 min after pneumoperitoneum, 15 min after the release of pneumoperitoneum, immediately after surgery, 15 min postoperatively, 30 min postoperatively, 45 min postoperatively, and 60 min postoperatively. Fall in HR after premedication was observed in Group D and was continued to be on the lower side when compared to Group S, throughout pneumoperitoneum. In 2014, Hazra et al. 15 observed the hemodynamic responses to laparoscopic cholecystectomy by administering 1 µg/kg dexmedetomidine, and they observed that there was a fall in HR and hypotension after administration because of a decrease in plasma catecholamine concentration. Similar findings were noted in a study done by Kumar et al.14 wherein a similar dose of dexmedetomidine was used. In 2019, Indira et al. 10 noted similar effects on HR after administration of a similar dose of dexmedetomidine. Concerning the above-mentioned studies and our findings, dexmedetomidine provides stable HR (Table 2) during the perioperative period when compared with Group S, which is statistically significant. In our study, only six patients in Group D developed bradycardia (P-value = 0.009) and responded to a single dose of atropine, 0.6 mg.
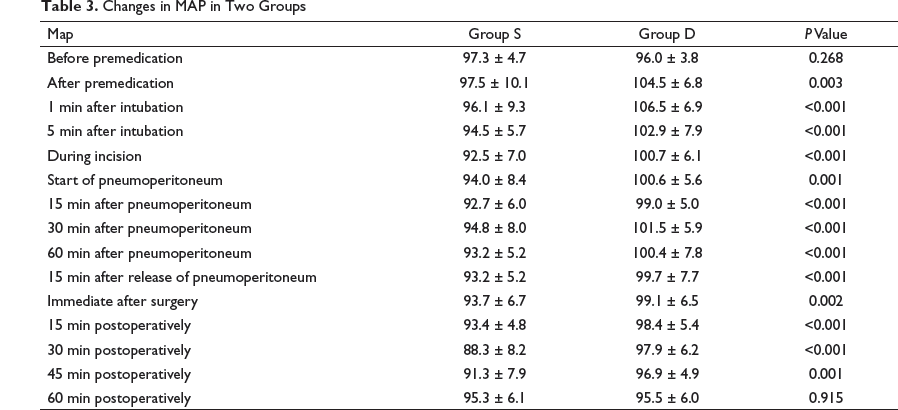
The baseline MAP values were insignificant, with a P-value of 0.268 (Table 3). At the rest of the time points, these were significantly lower in Group D.
The extent of variation of MAP from the baseline value in Group D was more controlled during pneumoperitoneum, which was statistically significant (P < 0.05).
Identical results have been obtained in various studies conducted by Shobharani et al. 16 and Indira et al. 10 wherein a similar dose of dexmedetomidine was compared to placebo. Similar results were found by Hazra et al. 15 and Kumar et al. 14 when 1 µg/kg of dexmedetomidine was compared with clonidine and normal saline.
During CO2 insufflation, the maximum rise in MAP in Group D was less when compared to Group S. CO2 insufflation into the peritoneum is known to cause changes in hemodynamics, which are measured as MAP, SVR, pulmonary vascular resistance, and a fall in cardiac output. 9
In several study reports, various infusion doses of dexmedetomidine have been tried, ranging from 0.1 to 10 µg/kg/h. Studies with higher infusion rates had adverse events, such as hypotension and bradycardia. In our study, we used dexmedetomidine as a single bolus dose of 1 µg/kg over 10 min as a premedication before induction, although few patients had bradycardia and hypotension, which were managed without any adverse outcome.
Limitations
As a result of its limited sample size, the study’s conclusions cannot be generalized, as we conducted the study on ASA I and II class patients. More studies are required on elderly and compromised cardiac status patients in order to recommend its use in such high-risk patients. Another limitation of this study was that BIS monitoring was not used to monitor intraoperative awareness and to establish its role in ensuring hemodynamic stability. The hemodynamic effects of different position variations on patients were not assessed. Furthermore, postoperative pain, sedation, and total analgesic score were not assessed.
Conclusion
In today’s era, open surgeries have been replaced by laparoscopic surgeries, which have been a boon. However, creating pneumoperitoneum during laparoscopy causes marked sympathetic activation, causing it to alter the hemodynamics.
Premedicating with a single bolus dose of 1 µg/kg IV dexmedetomidine over 10 min in ASA I and II patients has been proven safe and effective in maintaining the perioperative hemodynamic stability, although a few patients had bradycardia and hypotension, which were managed without any adverse outcome. Furthermore, dexmedetomidine effectively reduced the incidence of shivering.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.