
Abstract
Introduction:
The traditional method of blocking the ilioinguinal and iliohypogastric nerves may result in drug toxicity, block failure, and a significant amount of medication. Accurate needle placement made possible by the ultrasound-guided nerve block may lower the risk of medication toxicity, overdosage, and block failure.
Aim:
In this study, we examined the time to rescue analgesia, drug volume needed, and onset and duration of the motor and sensory nerve block between USG and conventional methods.
Settings and Design:
In this prospective study, 60 male patients with inguinal hernias between the ages of 18 and 60 who were the American Society of Anesthesiology I-II members and scheduled for repair were included in the study. They were randomly divided into two groups of 30 patients each using a computerized approach.
Materials and Methods:
Group A patients received hernia block by the conventional method using 0.75% ropivacaine 15 ml, and Group B patients were given the block guided by ultrasound using 0.75% ropivacaine, till the nerves were surrounded on all sides by the drug.
Statistical Analysis:
The data were analyzed using two independent sample t-tests for demographic and hemodynamic parameters. A nonparametric test (Mann–Whitney U-test) was used to find the significance between the Visual Analog Scale.
Results:
There was a significantly early onset of sensory block in Group B 14.03 ± 2.82 min as compared to Group A 15.57 ± 1.52 min (P = 0.047). The onset of motor block was also earlier in Group B 19.40 ± 2.85 min as compared to Group A 20.67 ± 1.90 min. The time to rescue analgesia was more in Group B 7.22 ± 0.97 h as compared to Group A 6.80 ± 0.70 h (P = 0.062). The volume of drug required was less with ultrasound-guided block.
Conclusions:
Ultrasound-guided hernia block thus has the advantage of early onset, less dose requirement, and increase in time to rescue analgesia.
Introduction
For surgeries including inguinal hernias, lower abdominal surgeries, and postoperative analgesia in cesarean sections, ilioinguinal (IIN) and iliohypogastric (IHN) blocks have been utilized as a standard anesthetic treatment.[1,2] In the plane between the transverse abdominis and internal oblique (IO), the IIN and IHN nerves are blocked during the nerve block.
The plane is found using PNS in the traditional block technique by monitoring twitches in the lower abdomen wall and inguinal region. By providing visual confirmation, properly putting the drug, and using less medicine, ultrasonographic-guided nerve blocks are beneficial.
Objective
The objective of this study was to compare the onset of sensory and motor block, the drug volume required, and the duration of the block in adult patients posted for elective inguinal hernia surgeries.
Materials and Methods
This randomized prospective study was carried out at the Konaseema Institute of Medical Sciences with 60 male patients after receiving institutional ethical committee approval. Using a computerized algorithm, the patients were divided into two groups of 30 each.
Ethical statement
Patients were informed about the study, the risks and their written consent was obtained. The study adheres to the guidelines of the Declaration of Helsinki.
Inclusion criteria
Male patients aged between 18 and 60 years
Patients can be classified under the American Society of Anesthesiology I-II
Posted for elective uncomplicated unilateral inguinal hernia repair.
Exclusion criteria
Large and irreducible hernias were excluded from the study. Body mass index ≥40 kg/m was not included in the study. Patients with a localized skin infection at the puncture site, allergy to local anesthetic agents, and chronic hepatic or renal failure were also excluded from the study.
After forming two different groups, regular investigations were conducted, and fitness was determined. Patients were given an oral ALPRAZOLAM 0.5 mg tablet the night before surgery. Patients were brought to the operating room on the day of the procedure, where monitors were affixed. All patients received injections of ondansetron 4 mg and midazolam 0.02 mg/kg as premedication.
Conventional technique
IIN and IHN nerve blocks were administered conventionally to all patients in Group A. The initial positioning of the patient was supine; later, the inguinal region was painted and draped. ASIS is 5 cm medial and 5 cm caudal from the point of injection.[3,6]
The block was made with a Stimuplex needle measuring 5 cm. The described landmark was where the needle was put. Once the needle passed through the IO fascia, we searched for twitches in the lower abdomen wall and the inguinal region. The nerve stimulator was set at 1 mA, 0.2 ms, and 2 Hz current. After that, the current was lowered to 0.5 mA and 15 ml of ROPIVACAINE (0.75%) was administered.
For the genital branch of the genitofemoral nerve (GFN) block, 4 ml of lignocaine with adrenaline was subcutaneously infiltrated just above the pubic tubercle, and the onset of sensory, motor block, and duration of the block were assessed.
Ultrasound-guided technique
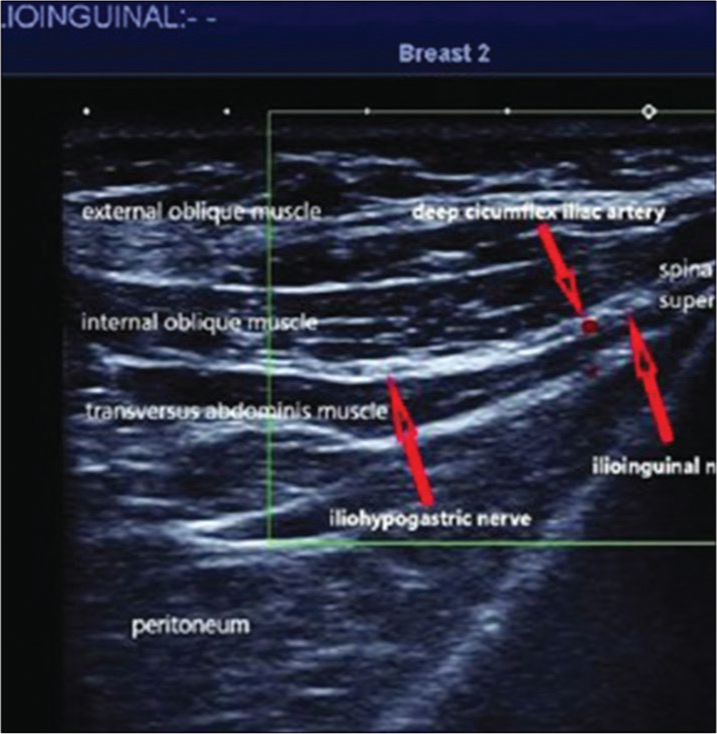
IIN and IHN blocks were performed on all of the patients in Group B using ultrasound guidance. The patient was initially positioned supine. A high-frequency linear probe was positioned between the iliac crest and costal margin in the painted inguinal area (more cephalad than the usual location for IIN block). The transversus abdominis and IO are located between the IIN and IHN nerves (Figure 1).[4,10] After visualization, the nerves were reached using an out-of-plane approach with a 22G 1.5-inch needle. Following aspiration, 0.75% injectable ropivacaine was infused until the drug completely encircled the nerves. The necessary volume was recorded. It was noted when the motor and sensory block started and how long it lasted.
Ultrasonographic view of the abdominal wall for ilioinguinal and iliohypogastric nerve block
Patients in both groups received surgical injections of 0.75% ropivacaine up to 5 ml for infiltration around the cord. Every 5 min up until the start of the action, which involves relaxing of the lower abdominal muscles and sensory block by pinprick, the quality of the sensory and motor blockade was evaluated. The block’s length was evaluated. Vital signs were checked every 15 min until the end of the 1st h and then hourly after that until the surgery was finished.
The Visual Analog Scale (VAS) was used to measure postoperative pain relief at the 1st, 2nd, 4th, 6th, and 8th h.[5] There was a notable time to rescue analgesia. When the patient reported their initial postoperative pain at a VAS score of III, we administered an intramuscular injection of diclofenac 1 mg/kg as a rescue analgesic.
Results
The 60 male patients in Group A underwent traditional IIN and IHN nerve blocks, and the 30 patients in Group B underwent ultrasonography-guided (USG) nerve blocks. Three members of Group A underwent general anesthesia as a result of their insufficient behavior.
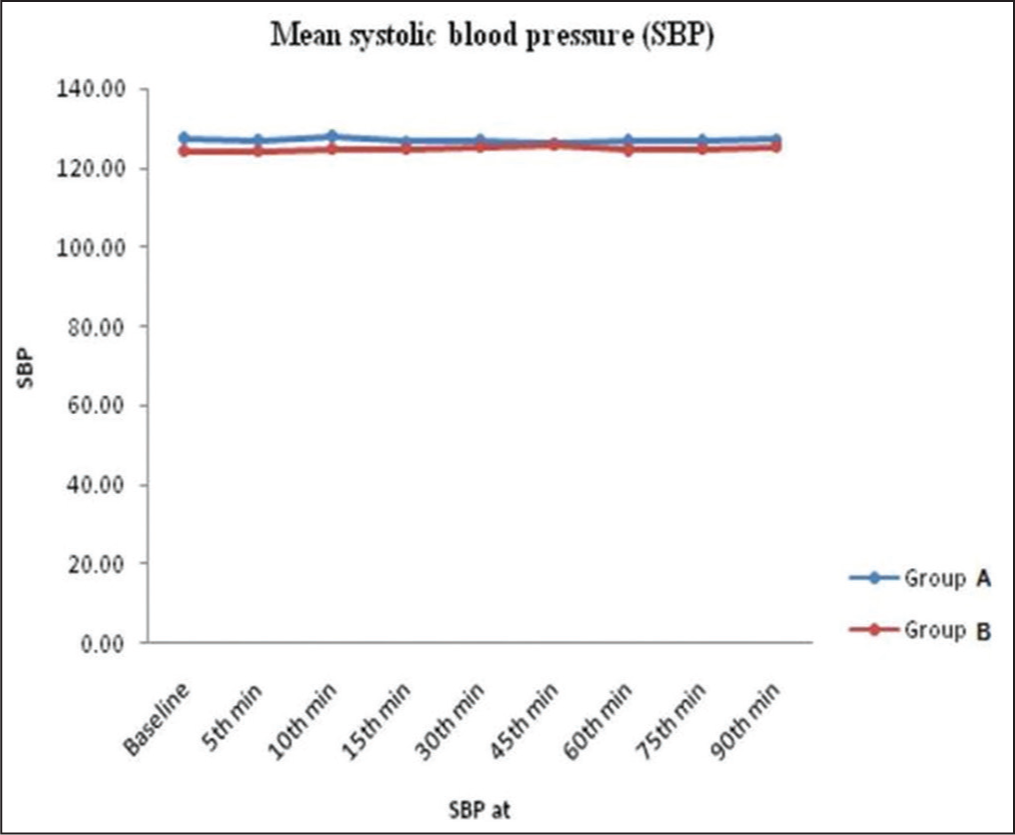
Patients in Group A were similar in age to those in Group B (42.03 11.68 vs. 40.07 11.07, P = NS). Figure 2 illustrates that throughout the study, with the exception of the 10th min, systolic blood pressure (SBP) mean baseline levels were equal. After the block, there was a statistically significant decrease in SBP (P = 0.05), although it had minimal clinical impact.
Depicting graph between mean systolic blood pressure and time
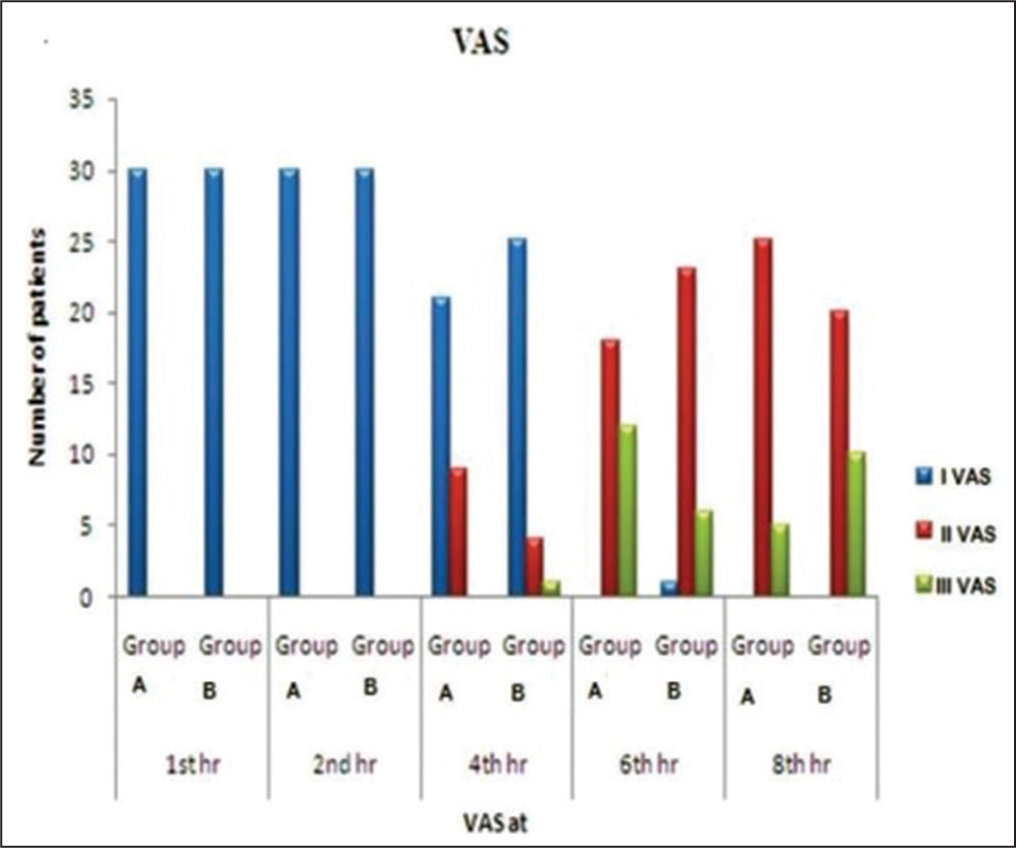
Comparing Visual Analog Scale between different groups
Diastolic blood pressure (DBP) and pulse rates (PR) were consistently comparable across the two groups (P = NS). We found that patients in Group B required a mean volume of 12.66 + or – 1.24 ml of ropivacaine for proper nerve encircling and action. The USG technique required a mean of 12.66 ml of medication to achieve block as opposed to the conventional method’s higher volume requirement.
Table 1 demonstrates that Group B experienced the onset of sensory block much earlier than Group A (15.57 1.52 min vs. 14.03 2.82 min; P = 0.047). Furthermore, Group B observed the start of the motor block 19.40 2.85 min before Group A did 20.67 1.90 min. Group B’s time to rescue analgesia was longer (7.22 0.97 h) than Group A’s (6.80 0.70 h) (P = 0.062).
Comparison of block profile
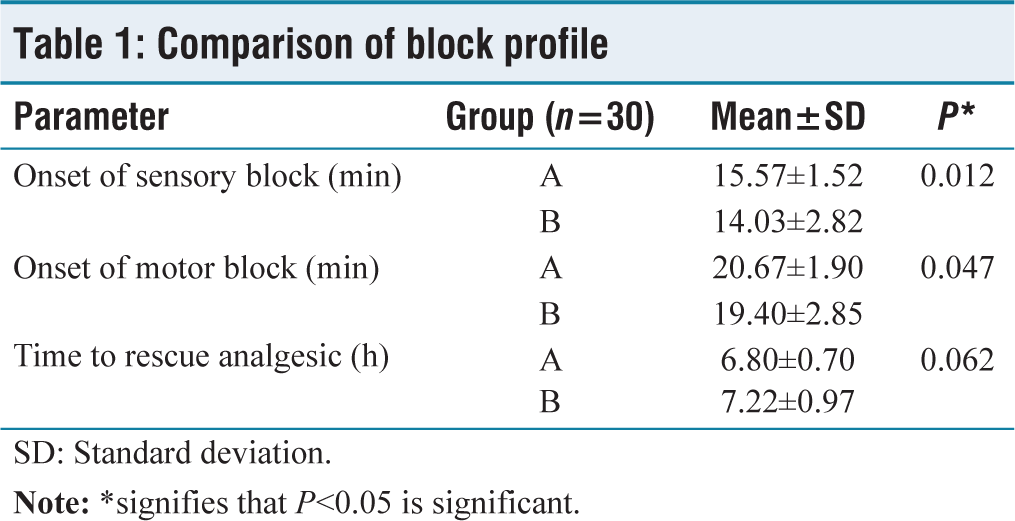
SD: Standard deviation
Both groups’ VAS scores were comparable, as shown in Figure 3. Twelve patients in Group A and six in Group B had VAS scores III at 6 h. At VAS III, we gave rescue analgesia. We found that Group B took longer than Group A (6.80 ± 0.70 h; P = 0.062) to regain analgesia (7.22 ± 0.97 h).
Power analysis
The research was done from March to August of 2022. Sixty individuals underwent surgery during this time. Using a population-based formula, the patient sample size was determined. We used straightforward computerized randomization to divide the patients into two separate groups based on inclusion and exclusion criteria as well as loss to follow-up. The test’s power for detecting the beginning of the motor block is 0.74. The test’s power for detecting the beginning of a sensory block is 0.83.
Statistical analysis
Data analysis was done using SPSS (Statistical Package for Social Science) version 17.0 (SPSS Inc., Chicago, IL, USA). We have used two independent sample t-tests to find the significance between the two groups for age, onset of sensory, onset of motor block, time to rescue analgesia, PR, SBP, and DBP.
Discussion
The process of blocking the sensory and motor IIN and IHN nerves can be straightforward with the aid of surface anatomy. However, challenges may arise due to anatomical variations. By closely monitoring for muscular twitches, peripheral nerve stimulation peripheral nerve stimulator (PNS) can be employed to effectively block these nerves. In this study, SKS built on the cadaveric study conducted by Eichenberger et al., which serves as a foundational reference.[4]
Situated 5 cm medial and 5 cm caudal to the anterior superior iliac spine (ASIS), the IIN and IHN nerves are nestled between the IO and transversus abdominis muscles. This landmark, as identified in our research, has been instrumental in the application of PNS for hernia blocking.
Although the IIN nerve is positioned beneath the external oblique fascia, medial, and anterior to the ASIS, this remains the recommended landmark for this block. However, relying solely on a “blind” technique at this location, combined with 15 ml of local anesthetic, proves inadequate in fully blocking these two nerves due to their ungrouped placement. This likely accounts for the notable failure rates (45%–72%) reported in the literature.[9] Success rates significantly improve when both nerves occupy the same layer of the abdominal wall, a point emphasized by Eichenberger et al.[4] He further contends that no nerves lie medial or caudal to the ASIS.
In our study, only 8% of participants experienced a block failure. Such failures are to be expected given the variable anatomy of the IIN and IHN.[7] Not every individual may exhibit a response to PNS due to these potential variances or even the absence of certain nerves.
Our method, derived from Eichenberger’s studies, demonstrates that blocking IIN and IHN within a single compartment (the transversus abdominis plane) before their division is feasible with a high probability of success, approximately 90%.
Both IIN and IHN are notably thick at the injection site, making them amenable to stimulation through a peripheral nerve stimulator (PNS). In addition, the GFN must be blocked to ensure complete analgesia and anesthesia during the inguinal repair.[11-13]
Through ultrasonography-guided (USG) block techniques, anatomical variances can be identified, leading to potential adjustments in the block approach. In our study, which included 60 patients split evenly between two groups, we compared the traditional IIN and IHN nerve block method with the ultrasonographically guided approach. Ropivacaine 0.75% was administered for the blocks in both groups. Among adult patients scheduled for elective hernia procedures, we assessed the efficacy of the block, its onset time, the volume of medication required, and the duration of the block for each technique.
Notably, the average volume of ropivacaine needed to encircle the nerve in Group B patients was 12.66 ± 1.24 ml. In contrast to the prior method, which demanded a higher volume, the USG technique proved more efficient with this reduced capacity. We directly observed, under ultrasonography, the precise amount of medication necessary to encircle the nerves and meticulously recorded these data. This approach effectively mitigates the risk of using excessive medication volume associated with potential toxicity. However, it is crucial to acknowledge that administering a smaller volume may increase the likelihood of block failure, leading to the need for early rescue analgesia. In our trial, one in four patients in Group B, who received 11 ml of medication, encountered inadequate analgesia, possibly attributed to the reduced volume. This might also be attributed to a learning curve associated with the new technique.
Willschke et al. recently introduced an unselective USG method for IIN and IHN blocks in pediatric patients, just medial to the ASIS.[8] In comparison to the conventional “blind” fascia click method, the authors were able to significantly reduce the amount of local anesthetic required to achieve an effective block. This translated to a noteworthy reduction in the need for supplementary analgesics both pre- and postsurgery in the USG nerve block group.
Conclusions
It was discovered that ultrasound-guided IIN and IHN nerve blocks had an earlier onset of sensory and motor block and required lesser dosage. When compared to the typical procedure, the time it took to restore analgesia was likewise extended. For inguinal procedures, the PNS-guided IIN and IHN block is a better approach. Utilizing PNS greatly improves safety, success rates, and aids in finding the nerves in the TAP.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Equipment and drugs required for the Research were provided by the Konaseema Institute of Medical Sciences and Research Federation.
Institutional Ethical Committee Approval Number
34/17.10.2021 - IEC number
CRediT Author Statement
Conceptualization: Yarramsetti V. Rao.
Manuscript writing: Yarramsetti V. Rao, Hari Kiran Nadimpalli, Dathrika Vagdevi K, Joel Ratnakar Kasapogu, Veda Sri Nimmaka
Manuscript revision: Yarramsetti V. Rao, Joel Ratnakar Kasapogu
Proof reading: Hari Kiran Nadimpalli, Yarramsetti V. Rao.
Data Availability
Data available - open access.
Use of Artificial Intelligence
No artificial intelligence used.