
Abstract
Background and Aims:
After robotic procedures, one of the most important things that helps patients recover quickly is postoperative pain control. When administered as a truncal block for postoperative analgesia in patients undergoing robotic prostatectomy, the quadratus lumborum block (QLB) can be quite successful. Our study aimed to evaluate the effectiveness of bilateral ultrasound-guided transversus abdominis plane block and bilateral ultrasound-guided QLB for postoperative pain relief following robotic prostatectomy.
Methods:
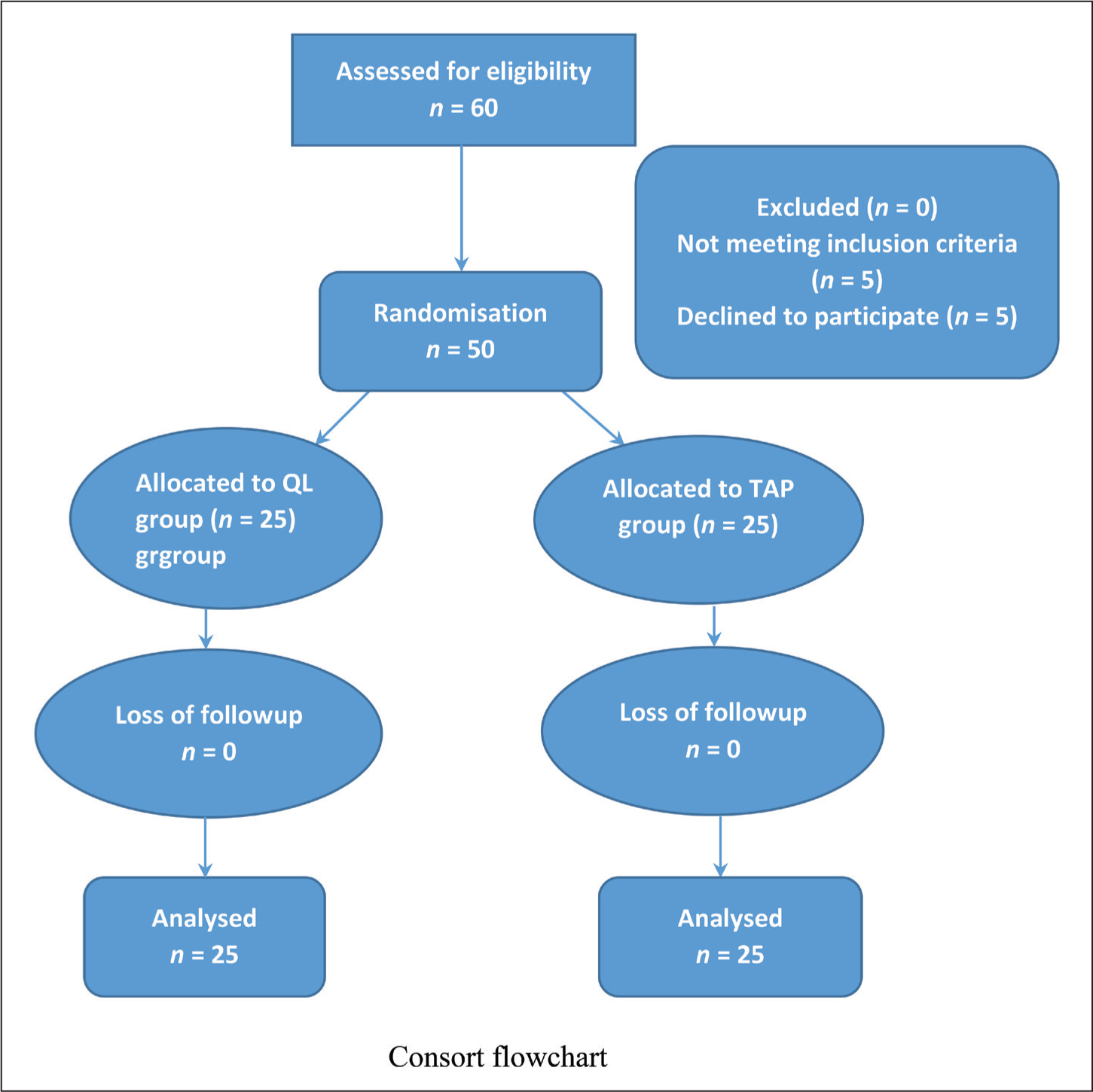
In this prospective randomised double-blinded study, 50 eligible patients were randomly divided into the QL group (n = 25) and transversus abdominis plane (TAP) group (n = 25). At the end of the surgery, for the QL group, an ultrasound-guided lateral QL block was performed with 20 mL of 0.375% ropivacaine on either side and for group TAP, an ultrasound-guided TAP block was performed with 20 mL of 0.375% ropivacaine on either side. The postoperative visual analogue scale (VAS) score at rest and movement over 12 hours at different intervals and the time to initiate the first rescue analgesia were the primary and secondary objectives, respectively.
Result:
The group that received an ultrasound-guided QL block had a better VAS score both at rest and movement over 12 hours post-surgery. Additionally, the mean duration required to take the first rescue analgesic was 6.1 ± 0.7 hours in the TAP block, while in the QL block group, it was 10.6 ± 0.9 hours, which was statistically significant.
Conclusion:
According to our research, patients who received QL block experienced more effective pain management. Furthermore, the initial rescue analgesia time needed was delayed. Thus, QL block is a useful technique for relieving pain in patients having robotic prostatectomy.
Keywords
Introduction
The most widely used minimally invasive urologic surgical method nowadays is robotic surgery. Patients who undergo robotic surgery have less discomfort because there are fewer keyhole incisions, less tissue retraction and less straining of the muscle and fascia fibres.[1]
Pain is a part of every surgery. Pain from the inflated peritoneum caused by carbon dioxide, visceral pain, incisional port site pain and shoulder tip pain are all related to robotic surgery. Prompt carbon dioxide inhalation into the peritoneum ruptures blood vessels, traumatises nerves and releases inflammatory mediators.[2]
The most recent procedure specific postoperative pain management (PROSPECT) guidelines for procedure-specific post-operative management of pain advice transversus abdominis plane (TAP) blocks for laparoscopic and robotic prostatectomy. These methods work well to reduce pain in the abdominal wall, but they are unable to stop the visceral pain. The quadratus lumborum block (QLB) technique is thought to be more effective in blocking somatic pain, with the potential to reduce visceral pain. This is due to the local anaesthetic’s numbing effect on the sympathetic trunk as it moves toward the paravertebral region. Blanco first described the QLB technique as the most posterior modification of the TAP block in 2007.[3]
Regional anaesthesia has changed from landmark-based methods to regional blocks given under direct vision through the ultrasound machine with the advent of portable ultrasound machines in operating rooms.[4]
This prospective study aimed to compare the analgesic effectiveness of ultrasound-guided QL block with ultrasound-guided TAP block for postoperative pain in patients having robotic prostatectomy. The primary objective was the level of pain, as assessed by a visual analogue scale (VAS) score at rest and movement within the first 12 hours following surgery. The secondary objective was the time of request for first rescue analgesia following surgery.
Materials and Methods
Following institutional ethical committee permission, 50 eligible patients were randomly assigned into two equal groups, QL and TAP (25 patients in each group), using a computer-generated random number table. A sealed, opaque envelope containing the group allocation was kept secret until an agreement to participate in the study was received. At the end of the surgery, ultrasound-guided blocks were performed by an experienced anaesthesiologist in both groups. The patients and the investigator evaluating the patients were not aware of their group allocation.
Patients who were scheduled for robotic radical prostatectomy and had provided written informed consent between August 2023 and January 2024 were recruited for this study. Patients who were undergoing elective robotic radical prostatectomy between the ages of 40 and 70, who come under the American Society of Anesthesiologists (ASA) 1 to 3, were included in this study.
Patients with chronic opioid addiction or long-term usage of other analgesics, local anaesthetic allergies, patients suffering from a language barrier, severe dementia or end-stage illness that makes communication difficult, and any nerve block contraindication, such as a puncture site infection or significant coagulation disorders, were excluded.
Methodology
All patients underwent preoperative evaluation, which included a thorough history, a general physical and a systemic examination. Prior to surgery, all investigations required for the administration of anaesthesia were completed and optimised. Patients were kept on nil per oral starting at midnight before the day of the surgery. Baseline data were recorded with an electrocardiogram (ECG) monitor, a non-invasive blood pressure monitor and a pulse oximeter attached to the operation room. An intravenous (IV) cannula was used to secure IV access. Prior to inducing anaesthesia, a three-minute preoxygenation period was conducted using 100% oxygen. The patient received injections of propofol (2 mg/kg IV), fentanyl (2 μ/kg IV) and atracurium (0.5 mg/kg IV) to promote muscle relaxation, followed by an infusion at a rate of 0.3 mg/kg/hr. An endotracheal tube that was the right size was used to intubate the patient. Sevoflurane 1 minimum alveolar concentration (MAC) was used in conjunction with a 50% oxygen and 50% air combination to achieve maintenance. Toward the end of the surgery, paracetamol 1 gm IV was given to both groups and before extubation, blocks were performed according to the allotted group.
TAP Block Group
In the TAP block group, the patient is positioned in a supine position. The high-frequency linear probe is positioned in a transverse plane on the anterior axillary line between the 12th rib and the iliac crest. Once the external oblique, internal oblique and transversus abdominis were visualised, using the in-plane approach, 20 mL of 0.375% ropivacaine was deposited in the plane between the internal oblique and transversus abdominis muscle under ultrasound guidance on either side.
QL Block Group
In order to provide adequate ultrasound vision of the desired posterolateral abdominal wall area, the patient is placed in a supine position with their hips elevated with a light roll under the hip of the side to be blocked and slightly tilted contralaterally with the side to be injected uppermost. The linear probe was positioned at the mid-axillary line on the crista iliaca for the lateral QL block. Once the three layers of the abdominal wall muscles were identified, the probe was pushed posteriorly to see the QL muscle, the thoracolumbar fascia (TLF) and the transversal fascia. Then, the in-plane approach was used to advance the needle between the QL muscle and the middle layer of the TLF. Following hydro-dissection to establish its position, 20 mL of 0.375% bupivacaine was administered on each side.
In both groups, pain was assessed using the VAS scale at 0.5, 1, 2, 6, 8 and 12 hours postoperatively, both at rest and movement. A VAS score ranged from 0 (no pain) to 10 (worst pain ever). Analgesics were given when the VAS score was greater than 3. The time required for the first rescue analgesic in the postoperative period was also noted. Inj tramadol 1mg/kg IV was used as rescue analgesic.
Sample Size Calculation
According to the Fargaly et al.[5] study, QL block required more time for the first analgesic requirement. Based on this information, considering the median difference as 9, the standard deviation (SD) as 13.3 from the interquartile range (IQR), power as 0.24, and a 95% confidence interval would require a minimum of 35 cases. However, we allocated 50 cases to ensure data loss was balanced. Formula used was
Statistical Analysis
Descriptive statistics were presented with frequency (percentage) and mean (SD) for the categorical and continuous factors respectively. Median (IQR) was presented for the skewed data. The normality of the data was checked by using the Shapiro–Wilk test. Student’s t-test/Mann–Whitney U test was used to determine the significant difference between QL and TAP. Friedman test was used to determine the significant changes over the time period, and the Wilcoxon signed rank was performed post-hoc to compare the changes pair-wise. P value < .05 considered as statistical significance. All the statistical analysis was carried out by using SPSS (IBM, 28.0).
Results
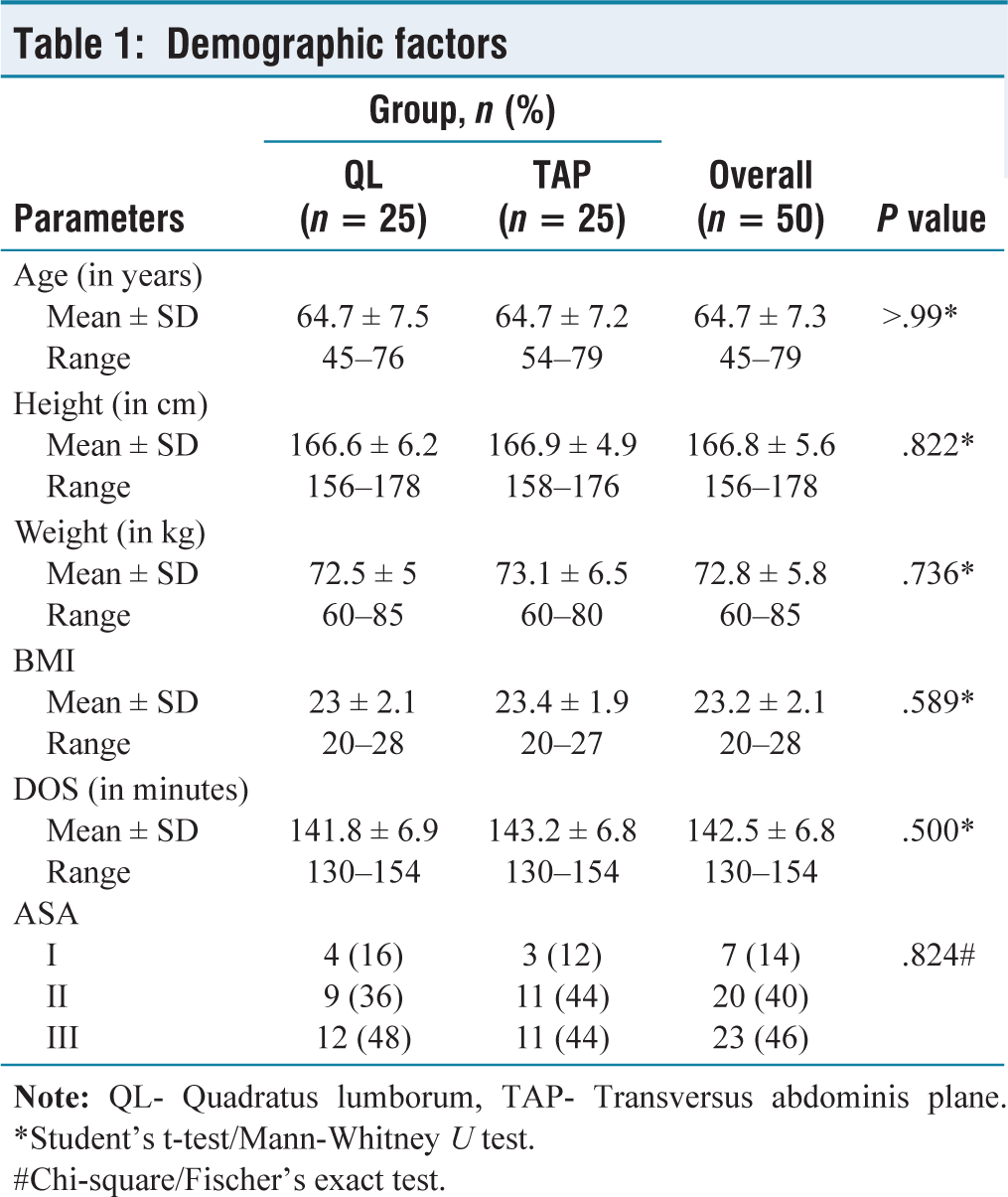
In this study, age, height, weight, body mass index (BMI), duration of surgery and ASA class were comparable between the two groups. Out of the 50 participants, 25 patients were in Group TAP block, and 25 patients were in Group QL. The mean age of Group QL was 64.7 ± 7.5 years, whereas the mean age of Group TAP was 64.7 ± 7.2 years. Group QL’s mean height was 166.6 6.2 cm, whereas Group TAP’s mean height was 166.9 4.9 cm and the mean weight was 73.1 6.5 kg [Table 1].
Demographic factors
#Chi-square/Fischer’s exact test.
The VAS score at movement was statistically significant between QL and TAP for each time (P value < .001; Table 2).
VAS score at movement
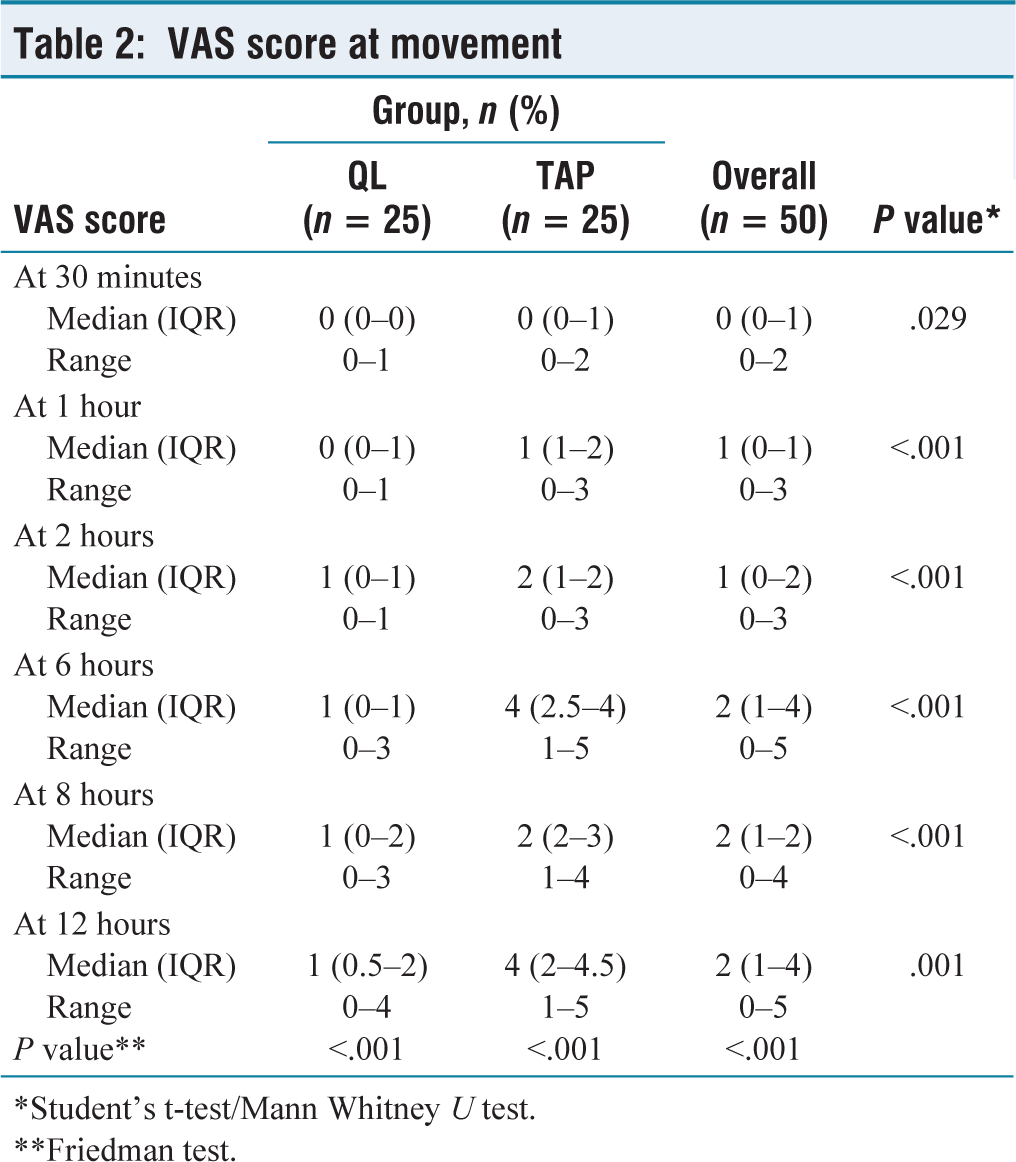
*Student’s t-test/Mann Whitney U test.
**Friedman test.
The VAS score at rest was significantly different between QL and TAP after 30 minutes (P value < .05). In the QL group, the VAS score significantly differed over the time (except 30 mins vs. 1 hour, 30 mins vs. 2 hours, 2 vs. 6 hours, 2 vs. 8 hours, 6 vs. 8 hours, 6 vs. 12 hours and 8 vs. 12 hours). In the TAP group, the VAS score significantly differed over time (except 1 hour vs. 2 hours, 6 vs. 8 hours and 6 vs. 12 hours; Table 3).
VAS score at rest
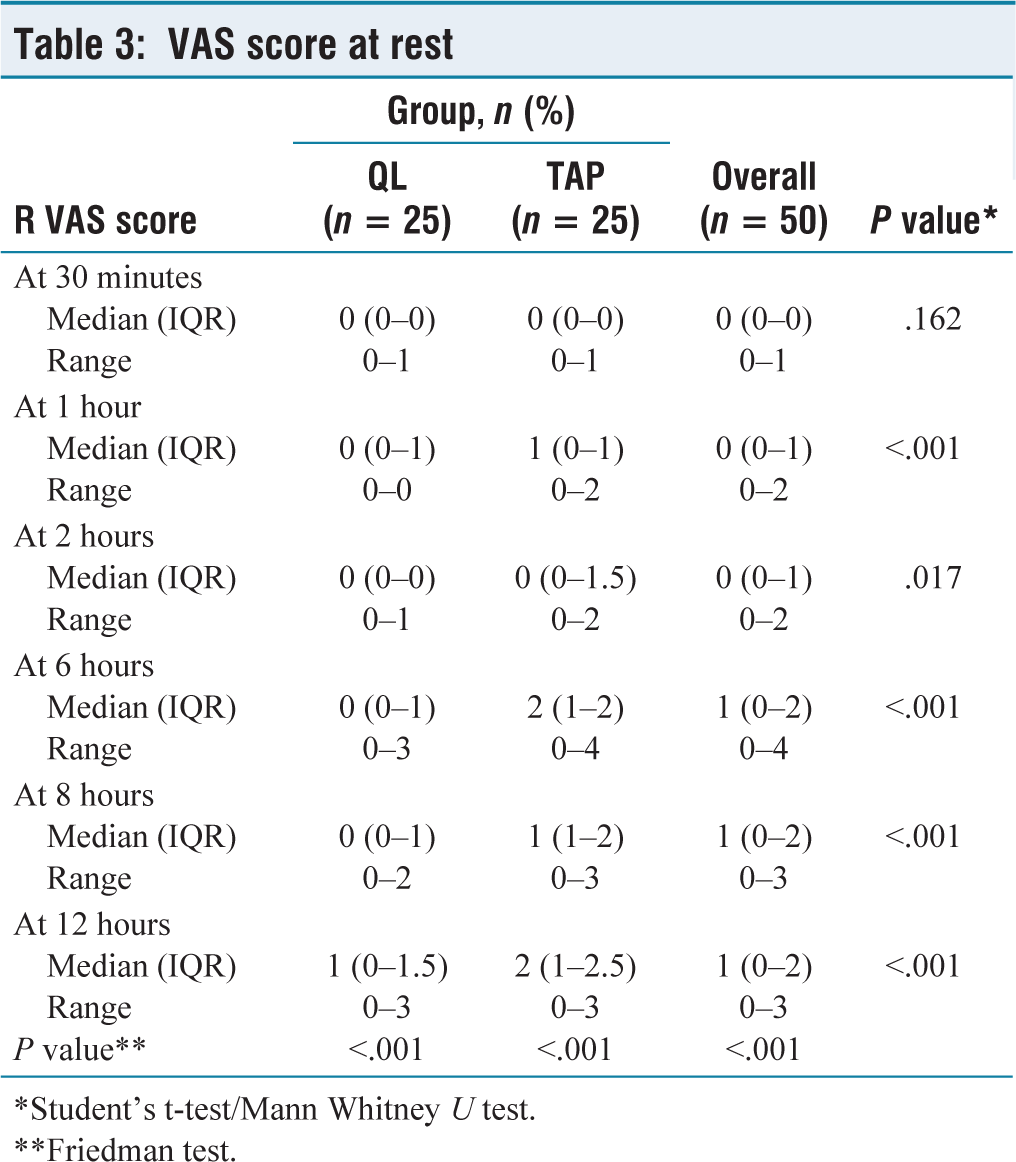
*Student’s t-test/Mann Whitney U test.
**Friedman test.
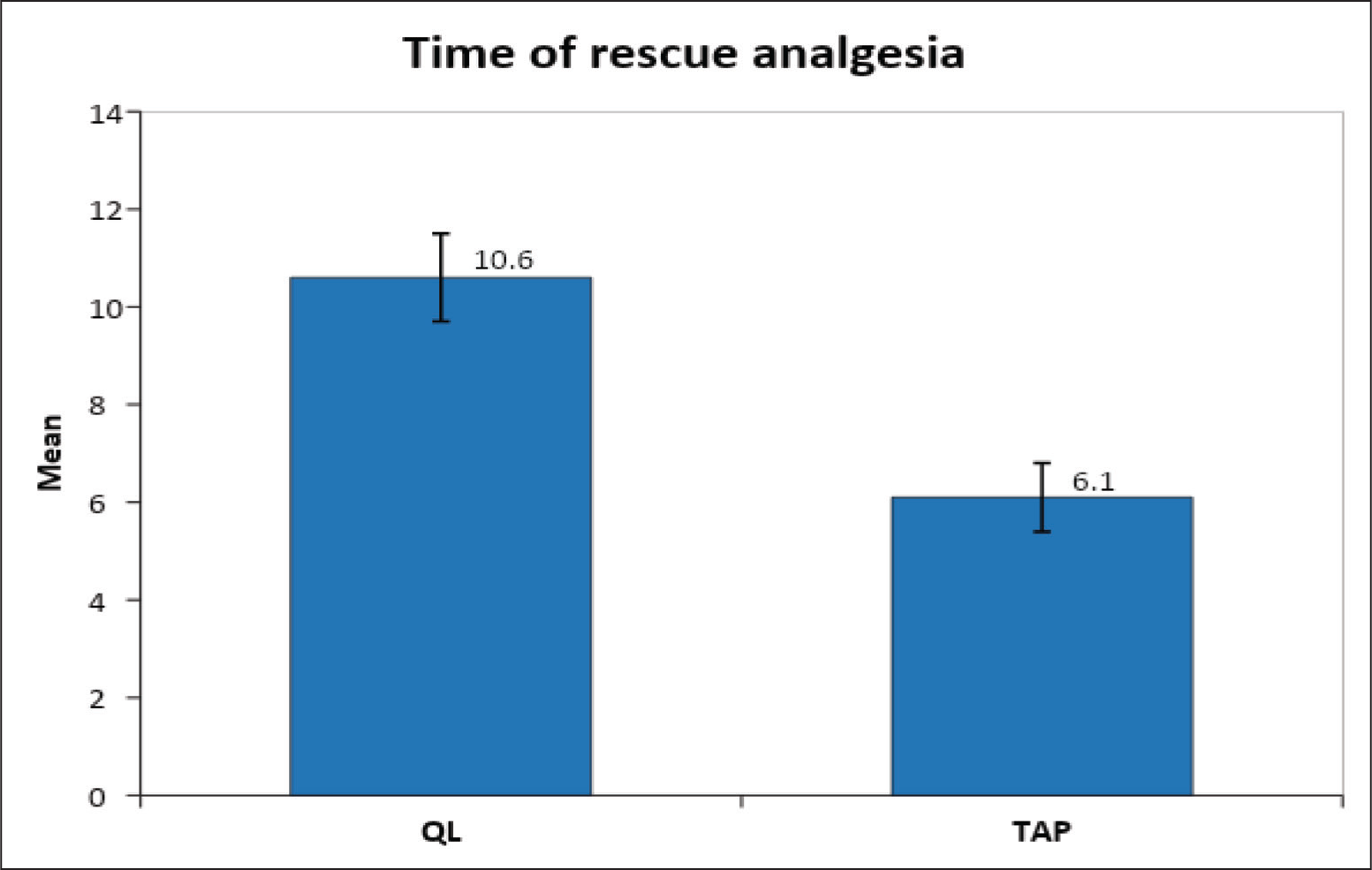
In the TAP group, the mean time required to take the first rescue analgesic was 6.1 ± 0.7 hours, while in the QL block group, it was 10.6 ± 0.9 hours. Thus, QL block postpones the need for first-rescue analgesia (P <.001; Table 4; Figure 1).
Time for rescue analgesia
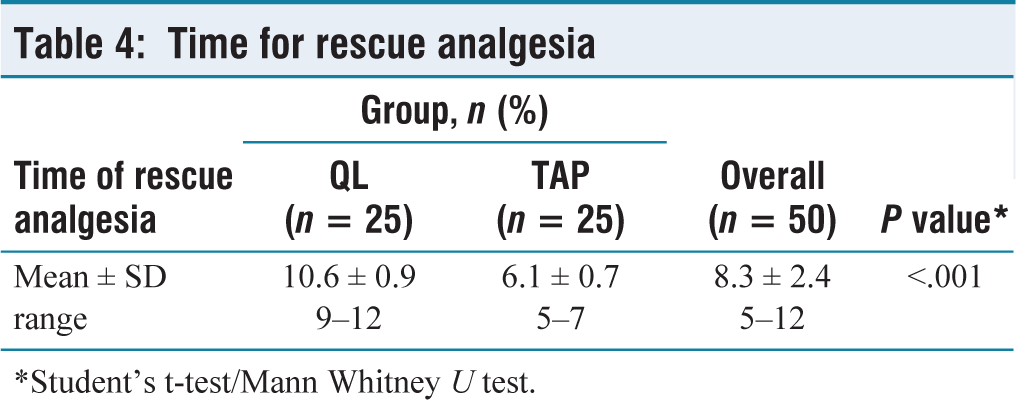
*Student’s t-test/Mann Whitney U test.
Bar graph representing time of rescue analgesia
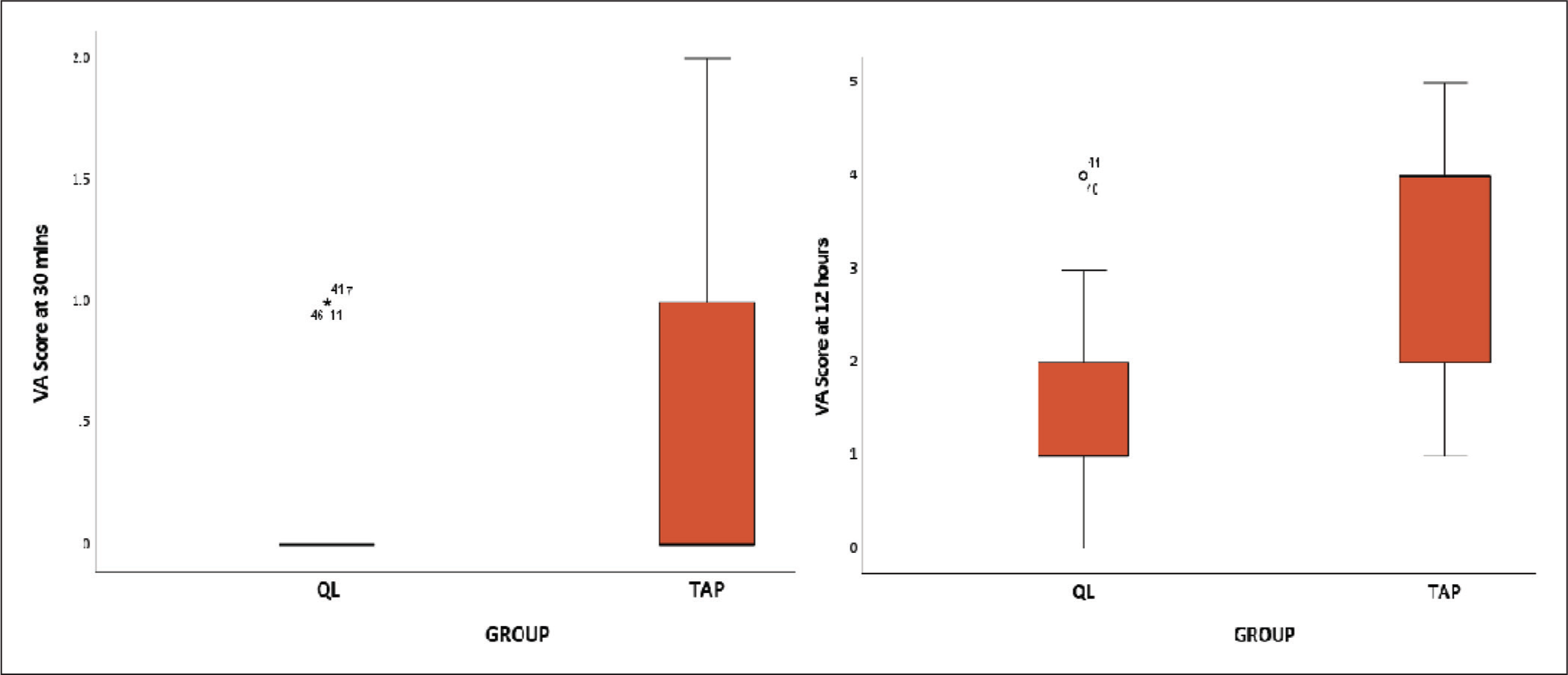
In both groups, compared to 30 minutes, the VAS score at movement increased in 12 hours [Figure 2].
Box plot representing VAS score at 30 minutes and 12 hours
Discussion
TLF plays a critical role in the analgesic impact of a QL block. The TLF is a complex connective tissue-based tubular structure. Local anaesthetics have the ability to cause an indirect paraspinal block by passing through the TLF and into the paravertebral space. Thus, it influences pain from abdominal incisions as well as visceral pain.[6]
According to our study, the pain scores at 30 minutes, 1, 2, 6, 8 and 12 postoperative hours were considerably lower in the QL group than in the TAP group, and the difference was statistically significant.
Liu et al.[6] also showed that 2, 6 and 12 hours following lower abdominal operations, patients in the TAP block group had pain scores greater than those of patients in the QL block group, which was similar to our results.
Our results are in agreement with a study conducted by Anju et al.[7] for lower-segment caesarean patients. In their study, they found out that for the first 12 hours, the QL group’s VAS scores were considerably lower than those of the TAP group at every observation period.
Additionally, our results are consistent with those of Alansary et al.,[8] who found that QLB was a better postoperative analgesic and had a better VAS score than TAP in patients undergoing total abdominal hysterectomy.
Our study shows that the time taken to initiate the first analgesic request in the TAP group was faster than QL group.
According to the Jadon et al.[9] study, the median (IQR) time to the initial analgesic request for the QL group was 12 (9.25, 13) hours, while for the TAP group, it was 9 (8.25, 11.37) hours. This indicates that there was a significant difference in the two groups’ median (IQR) time to the initial analgesic request.
The results of our investigation supported those of Alansary et al.,[8] who found that the QLB produces analgesia that lasts longer than the TAP block in their study of patients undergoing total abdominal hysterectomy.
The mean duration of analgesia for the QL block was 16.5 hours (9–24 hours), and for the TAP block, it was 8.5 hours (6–12 hours), with a statistically significant difference shown by a P value <.001 in the Anju et al.,7 study, which is similar to our study.
The VAS score was lower in the QL group than in the TAP block group, taking into consideration VAS at rest and movement, which is similar to our study.[10]
Apart from its deep analgesic effects, QL block also has the advantage of a relatively safer injection because there is a lower chance of an intraperitoneal injection and bowel damage since the QL muscle keeps the needle point away from the peritoneum.[10]
There are certain limitations in our study. The study could have been multicentre. The sample size in our study was 50. A larger sample size might yield more reliable results.
Conclusion
Our research indicates that throughout the first 12 hours following surgery, QL block improves VAS scores both during movement as well as during rest. Additionally, the QL group experienced a delay in the initial rescue analgesia needed time. Therefore, patients undergoing robotic prostatectomies have more pain alleviation from QL block as opposed to tap block.
Footnotes
Acknowledgements
Thanks to the Research Department, Apollo Main Hospital, Chennai, Tamil Nadu.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Institutional ethical committee approval number
Approval was obtained from the Institutional Ethical Committee on 25.07.2023. NO: AMH-C-S-046/07-23.
Informed consent
Informed consent has been obtained from the patients who met the eligible criteria.
Credit author statement
V participated in conceptualisation, methodology, data collection, data analysis and manuscript preparation.
AG was involved in conceptualisation, literature search and manuscript revision.
PC was involved in conceptualisation, validation, supervision and manuscript revision. All the authors have reviewed and approved the manuscript.
Data availability
The datasets used and/or analysed during the current study are available from the corresponding author upon request.
Use of artificial intelligence
Not used.