
Abstract
Introduction
Obesity is a well-established risk factor for the development, recurrence, and postoperative complications of ventral hernia repair. However, the relationship between obesity and inguinal hernia repair is less well defined, with limited evidence on how body mass index (BMI) influences operative approach and outcomes.
Methods
A retrospective review of the 2022-2023 ACS-NSQIP database was performed including all adult patients who underwent inguinal and femoral hernia repairs identified using CPT codes. Bivariate and multivariable regression analyses were used to examine the impact of obesity and BMI on operative approach, case acuity, operative time, and short-term outcomes after inguinal hernia repair.
Results
A total of 73 456 adult patients were identified with a mean age of 61 years. Higher BMI was associated with greater operative complexity, including longer operative times and increased use of robotic and combined approaches. Surgical site occurrences (SSOs) were uncommon overall (0.7%) but increased progressively with higher BMI. In multivariable analysis, the association between BMI and operative characteristics, SSOs, and major complications varied across BMI levels. Higher BMI was independently associated with increased odds of SSOs and major complications, while laparoscopic and robotic approaches were consistently associated with lower odds of adverse outcomes compared with open or combined approaches.
Conclusion
Higher BMI is associated with increased operative complexity and worse short-term postoperative outcomes following inguinal hernia repair, while minimally invasive approaches were associated with lower odds of obesity-related adverse outcomes. These findings highlight the importance of individualized risk stratification and preoperative optimization in inguinal hernia repairs.
Key Takeaways
• BMI is nonlinearly associated with perioperative risk in inguinal hernia repair, with clinically meaningful increases in surgical site occurrences, and major complications. • Higher BMI independently predicts greater operative complexity, including longer operative times and increased use of robotic and combined approaches. • Minimally invasive approaches are associated with lower odds of short-term adverse outcomes compared with open or combined approaches across BMI strata, potentially reflecting both patient selection and the technical advantages of minimally invasive techniques.
Introduction
Obesity is a growing health concern affecting over 40% of adults in the United States 1 and is widely associated with increased perioperative morbidity in abdominal surgery. Specifically, obesity is a well-established risk factor for the development of ventral hernias as well as postoperative complications after hernia repair.2,3 However, the relationship between obesity and inguinal hernia disease and postoperative outcomes is less clearly defined.
Epidemiologic studies suggest a paradox: higher BMI has been associated with a lower incidence of inguinal hernia, potentially due to increased preperitoneal adiposity and diagnostic challenges in patients with obesity.2,4 However, among patients who undergo inguinal hernia repair, obesity has been linked to higher rates of recurrence and postoperative complications, including wound morbidity. 5 These observations reveal a knowledge gap regarding how BMI influences the perioperative risk profile in inguinal hernia surgery.
At the same time, inguinal hernia repair is undergoing rapid evolution in operative technique, including a marked increase in the use of robotic platforms and techniques. Although minimally invasive approaches may offer advantages in selected patients, the comparative benefits of robotic repair over laparoscopy remain uncertain, and evidence is limited regarding how BMI influences operative approach selection and short-term outcomes across open, laparoscopic, and robotic repairs.
In this study, we aimed to examine the impact of obesity (BMI ≥30) and BMI on operative approach, case acuity, operative time, and 30-day postoperative outcomes after inguinal hernia repair using the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database. We hypothesize that higher BMI would be associated with greater operative complexity, including longer operative times and greater use of robotic approach, as well as worse 30-day postoperative outcomes, including surgical site occurrences and other complications. We also hypothesize that minimally invasive approaches would be associated with lower odds of adverse outcomes compared to open repair.
Methods
Data Collection
Institutional Review Board approval was obtained from the University of Southern California prior to study initiation. We conducted a retrospective analysis of the 2022-2023 American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) database, which includes patient demographics, comorbidities, operative characteristics, and 30-day postoperative outcomes from over 600 U.S. hospitals. The years 2022 and 2023 were selected because robotic surgical approach was added as a variable to the NSQIP database starting in 2022. Adult patients (≥18 years) undergoing inguinal or femoral hernia repair were identified using primary CPT codes for open and laparoscopic inguinal and femoral hernia repairs (49505, 49507, 49520, 49521, 49525, 49650, 49651, 49550, 49553, 49555, 49557).
Patients were stratified by BMI category (<30, 30-35, 35-40, and >40). Patients with missing height or weight data or an undefined operative approach were excluded. Surgical site occurrence (SSO) was the primary outcome of interest, which is a composite outcome variable including superficial surgical site infection (SSI), deep SSI, organ space SSI, and wound disruption. Additional covariates and outcomes examined included operative characteristics stratified by BMI, length of total hospital stay, unplanned reoperations, readmissions, mortality, and other major complications, including pulmonary embolism, unplanned intubation, ventilator >48 hours, post-op renal insufficiency, post-op dialysis, cerebrovascular accident/stroke with neurological deficit, cardiac arrest requiring CPR, myocardial infarction, sepsis, and septic shock.
Statistical Analysis
Categorical variables are reported as frequencies and proportions (%) and continuous variables as means with standard deviations (SDs) or median with range. Demographics and outcome distribution across BMI groups were compared using Pearson chi-square test for categorical variables. One-way analysis of variance (ANOVA) was used to compare continuous variables. Multivariable regression modeling was used to adjust for potential confounders (sex, smoking, COPD, operative approach, age as quartiles, and diabetes). Logistic regression was performed for surgical site occurrence (SSO) and complications, and linear regression with log transformation was used for operative time. To characterize the relationship between BMI and urgency of surgical presentation, case acuity (elective vs urgent/emergent) was modeled as the dependent variable in an exploratory multivariable logistic regression. This analysis was intended to identify patient-level factors associated with urgent vs elective hernia presentation and does not represent a postoperative outcome model. BMI was modeled as a continuous variable in all analyses.
Nonlinearity between BMI and outcomes was assessed using locally estimated scatterplot smoothing (LOESS) plots, fractional polynomial models, and spline regression. Model selection was guided by Akaike and Bayesian Information Criteria. Final models included spline terms for BMI for SSO (≤23, 23-47, >47) and complications (≤30, >30), and a spline model (≤23, >23) for case acuity for interpretability. Model diagnostics included residual plots for linear regression and the Hosmer-Lemeshow test for logistic models. Statistical significance was defined as two-sided α < 0.05. All analyses were performed using SAS version 9.4 (SAS Institute Inc, Cary, NC).
Results
Patient Demographics
Patient Demographics Stratified by Body Mass Index (BMI)
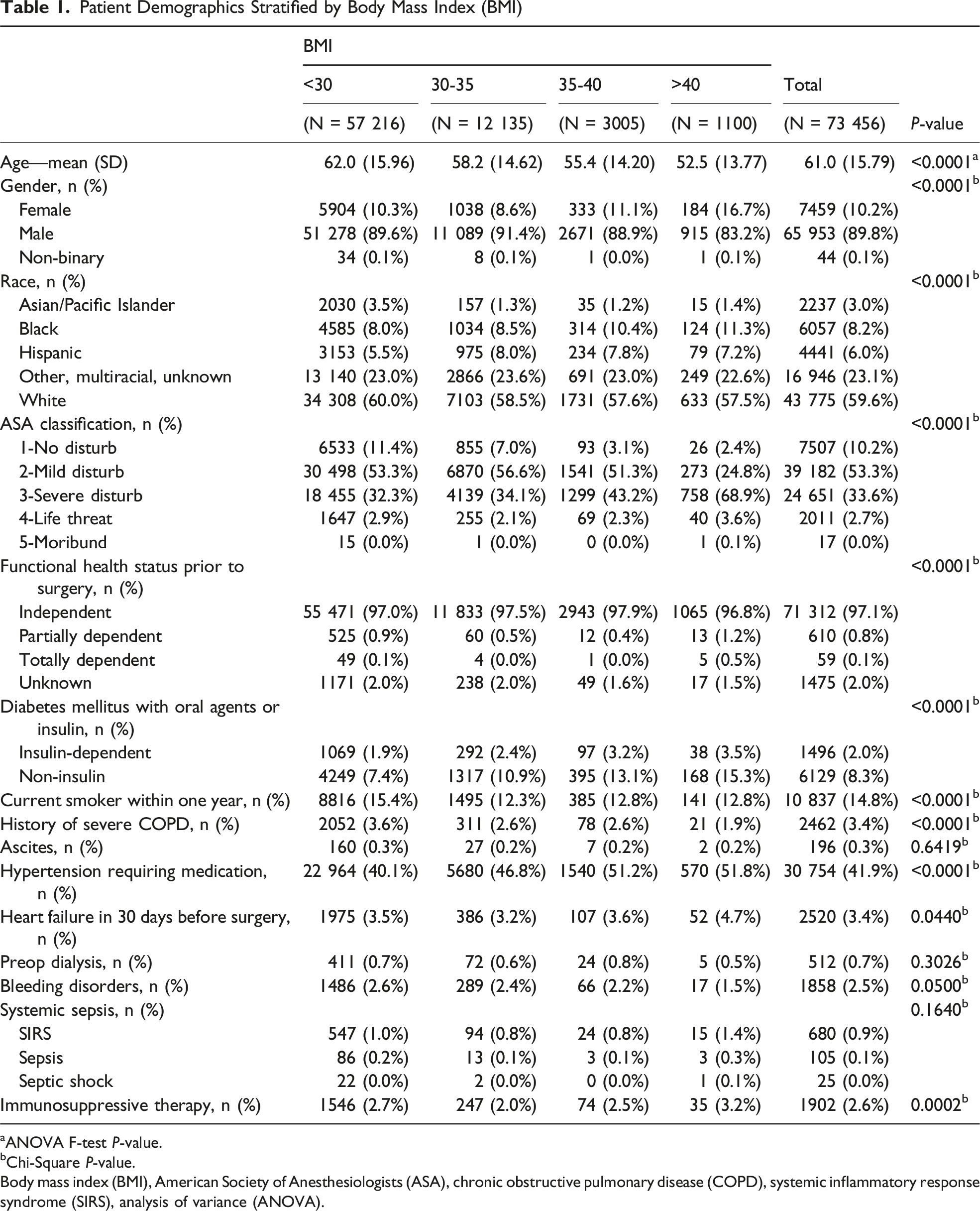
aANOVA F-test P-value.
bChi-Square P-value.
Body mass index (BMI), American Society of Anesthesiologists (ASA), chronic obstructive pulmonary disease (COPD), systemic inflammatory response syndrome (SIRS), analysis of variance (ANOVA).
Operative Characteristics Including Case Acuity and Operative Time
Operative Characteristics Stratified by Body Mass Index (BMI)
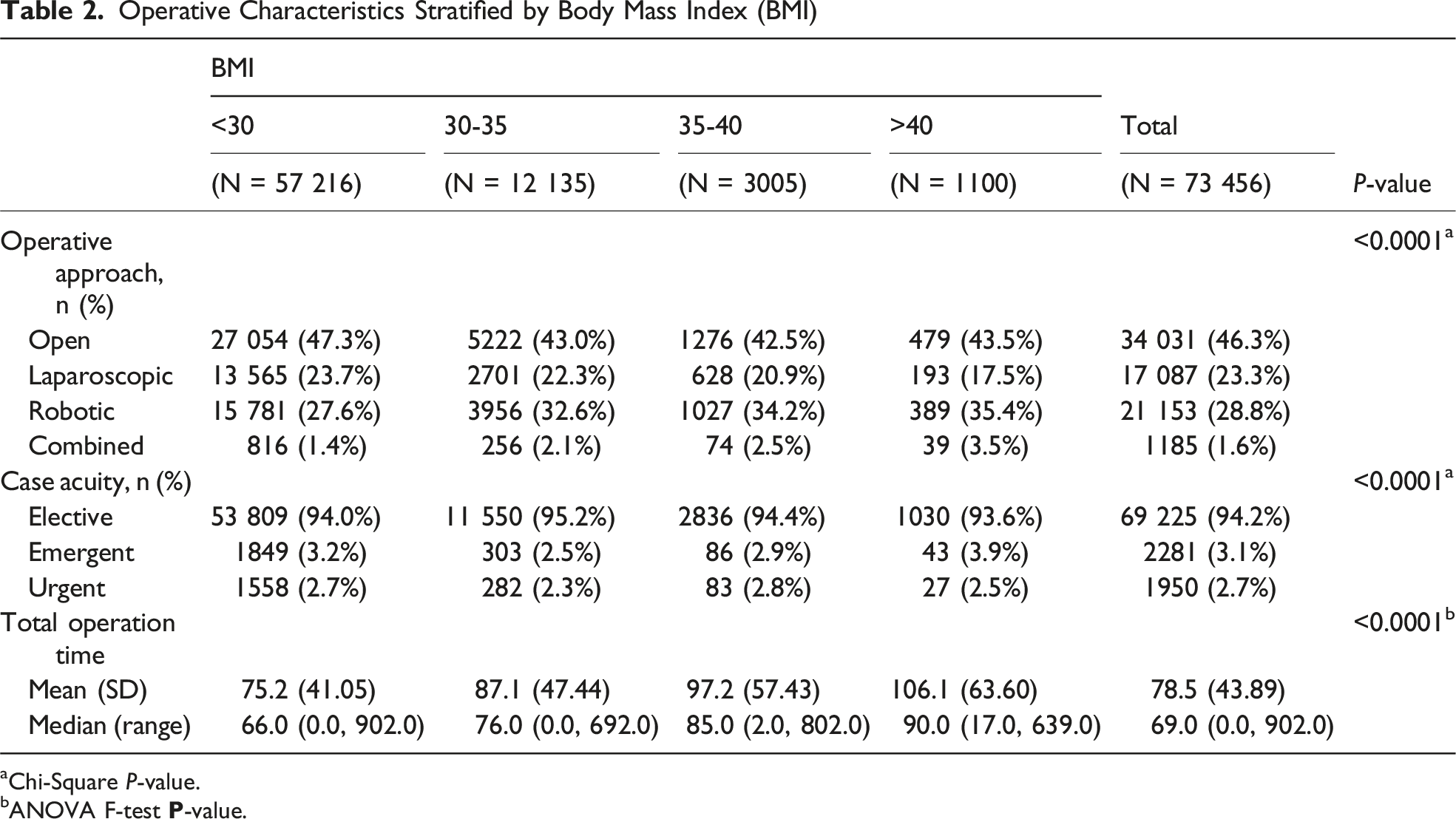
aChi-Square P-value.
bANOVA F-test
To characterize which patient-level factors are associated with urgent vs elective hernia presentation, we modeled case acuity as the dependent variable in an exploratory multivariable logistic regression. In multivariable logistic regression, BMI demonstrated a nonlinear association with case acuity (urgent/emergent vs elective). Among patients with BMI ≤23, each one-unit increase in BMI was associated with lower odds of urgent or emergent surgery (OR: 0.87, 95% CI: 0.85-0.90, P < 0.001), whereas no significant association was observed for BMI >23. Female sex, current smoking, and COPD were independently associated with higher odds of urgent or emergent operations. Compared with open repair, robotic and laparoscopic approaches were less likely to be performed in the urgent/emergent setting (OR: 0.17 and 0.39, respectively, all P < 0.001), while combined approach was more likely done as urgent/emergent cases (OR: 2.17, 95% CI: 1.85-2.54, P < 0.001) (Supplemental Table 1).
Additionally, increasing BMI was independently associated with longer operative duration, with each one-unit increase in BMI corresponding to a 1.5% increase in operative time (on log scale, beta = 0.0152, 95% CI: 0.0145-0.016, P < 0.001). Operative approach was also a strong predictor of operative duration, with combined and robotic approaches associated with substantially longer operative times (63.5% and 33.9% increase, respectively) compared to open repair, while laparoscopic repair was associated with a modest 4.8% increase in operative time (all P < 0.001) (Supplemental Table 2).
Higher BMI Is Associated With Increased Risk of Surgical Site Occurrences (SSOs)
Bivariate Analysis of Patient Outcomes Stratified by Body Mass Index (BMI)
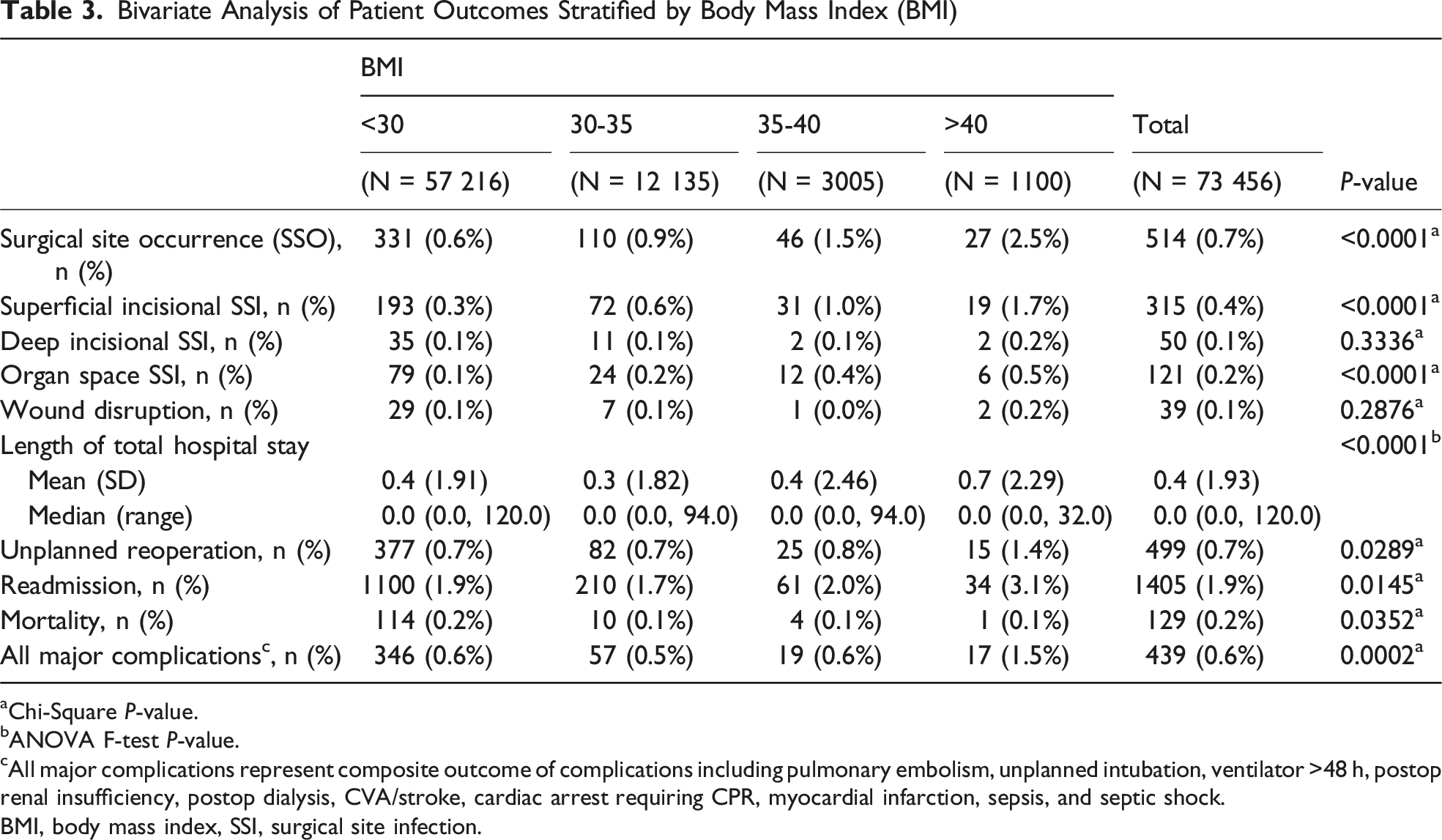
aChi-Square P-value.
bANOVA F-test P-value.
cAll major complications represent composite outcome of complications including pulmonary embolism, unplanned intubation, ventilator >48 h, postop renal insufficiency, postop dialysis, CVA/stroke, cardiac arrest requiring CPR, myocardial infarction, sepsis, and septic shock.
BMI, body mass index, SSI, surgical site infection.
Multivariable Logistic Regression Model for Surgical Site Occurrences (SSOs)
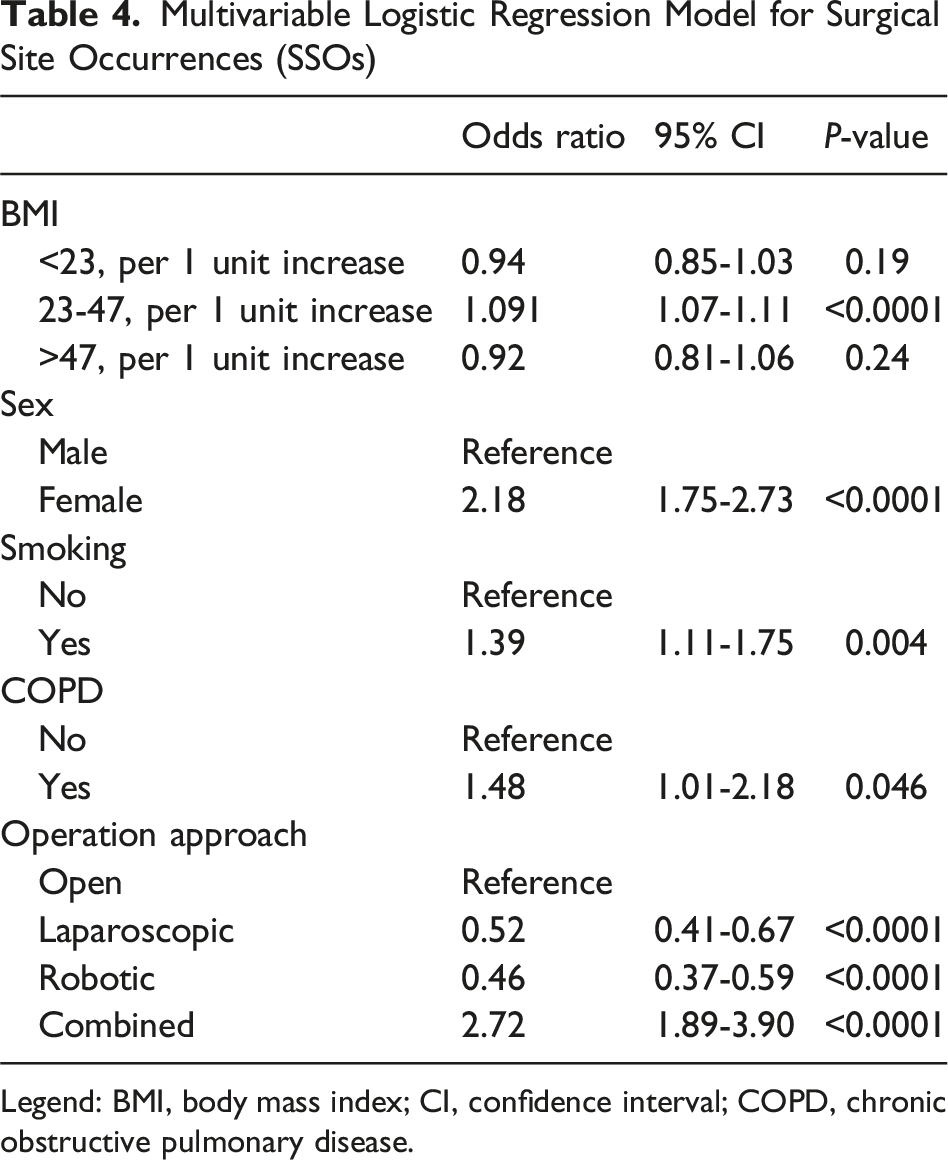
Legend: BMI, body mass index; CI, confidence interval; COPD, chronic obstructive pulmonary disease.
Higher BMI Is Associated With Worse 30-day Postoperative Outcomes
Additional 30-day postoperative outcomes stratified by BMI are also shown in Table 3. Increasing BMI was associated with worse short-term postoperative outcomes, including higher rates of unplanned reoperation, readmission, and major complications (all P < 0.05). Patients with BMI >40 experienced the highest rates of reoperation (1.4%), readmission (3.1%), and major complications (1.5%). Length of hospital stay also increased with BMI, with patients in the highest BMI category demonstrating longer mean postoperative length of stay (P < 0.001). Although overall mortality remained low across all groups (0.1-0.2%), small but statistically significant differences were observed (P = 0.035).
On multivariable logistic regression modeling, each one-unit increase in BMI above 30 was independently associated with higher odds of major complications (adjusted OR: 1.08, 95% CI: 1.06-1.11, P < 0.001), whereas no significant association was observed for BMI ≤30 (P = 0.44). Additional independent predictors of major complications included female sex (OR: 1.31, 95% CI: 1.01-1.71, P = 0.042), current smoking (OR: 1.70, 95% CI: 1.32-2.20, P < 0.001), COPD (OR: 2.15, 95% CI: 1.57-2.95, P < 0.001), insulin-dependent diabetes (OR: 1.48, 95% CI: 1.22-1.80, P < 0.001), older age >51, and operative approach. Compared to open repair, combined approach was associated with higher odds of complications (OR: 2.58, 95% CI: 1.69-3.95, P < 0.001) while laparoscopic (OR: 0.58, 95% CI: 0.44-0.77) and robotic (OR: 0.56, 95% CI: 0.43-0.72) approaches were protective (all P < 0.001) (Supplemental Table 3).
Discussion
In this study, we aimed to examine the impact of obesity and BMI on operative characteristics as well as postoperative outcomes in patients undergoing inguinal hernia repair using the most recent NSQIP data including robotic approach as an important variable. We found that higher BMI was associated with greater operative complexity as indicated by operative approach and longer operative time as well as worse short-term outcomes. As BMI increased, patients were more likely to undergo robotic or combined repairs and experienced progressively longer operative times, suggesting increased technical demands and resource utilization. Higher BMI was also associated with higher rates of 30-day adverse outcomes, including surgical site occurrences and major complications, as well as increased readmissions, reoperations, and length of stay.
More importantly, the association between BMI and outcomes was not uniform across the BMI levels for case acuity, SSOs, and major complications. Finally, minimally invasive approaches including robotic and laparoscopic were consistently associated with lower odds of SSOs and major complications compared with open repair. However, it is worth noting that operative approach was not randomly assigned in this observational data, and these associations likely reflect both the technical advantages of minimally invasive techniques and systematic differences in patient selection. Surgeons may preferentially choose laparoscopic or robotic approaches in patients who are higher BMI but otherwise lower risk. On the other hand, combined approach was associated with higher odds of SSOs and complications in addition to higher acuity and longer operative time, which likely speaks to the complexity of the inguinal hernia for which simultaneous open exposure and laparoscopic/robotic access is indicated.
Prior literature has largely focused on the impact of obesity on ventral hernia repair, where increased BMI is clearly associated with worse postoperative outcomes and minimally invasive approaches associated with lower rates of obesity-related complications compared with open surgery.6,7 In contrast, the relationship between obesity and inguinal hernia repair is less well defined. While one observational study by Miranda et al 8 showed open repair is more commonly performed in patients with higher BMIs when compared to laparoscopic approach, other studies have shown higher average BMIs among patients undergoing robotic or minimally invasive repairs and lower BMIs in those who had open repair,9,10 which is more consistent with our analysis. An important finding of our study is the progressive shift toward robotic repair with increasing BMI, confirming what most hernia surgeons already practice. This pattern likely reflects both increasing technical complexity in patients with obesity and the rapid adoption of robotic platforms, which offer ergonomic and visualization advantages that may be particularly appealing in higher BMI patients.
Our findings regarding operative time and case acuity are consistent with existing literature. Previous studies have demonstrated a positive association between increasing BMI and operative duration, with reported increases of 18-20 minutes when comparing obese to normal-weight patients.11,12 Similarly, we observed a stepwise increase in operative time with increasing BMI, as well as longer operative time associated with robotic and combined approaches, which is also consistent with existing literature.13,14 With respect to case acuity, existing data suggest higher rates of emergent repair among lower-BMI patients, 15 which is consistent with the findings of inverse relationship between BMI and case acuity in those with BMI <23. This may reflect the higher proportion of thin female patients undergoing emergent groin hernia repair, including femoral hernias, which is also supported by female sex as an independent risk factor for urgent/emergent cases in our multivariable regression model.
Regarding surgical site occurrences (SSOs), a recent meta-analysis by Li et al examined 9 studies and concluded patients with obesity had more wound infections (OR: 1.43) and more overall complications (OR: 1.12), which is in agreement with our findings. However, our multivariable regression model demonstrated a positive association only for BMI 23 to 47 where higher BMI increased SSOs in a stepwise fashion. This is somewhat similar to a large Swedish registry study by Rosemar et al 15 where a U-shaped relationship was demonstrated between BMI and surgical site occurrence after inguinal hernia surgery, segmented by BMI. The authors found patients with BMI <20 and >25 had significantly increased risk compared to patients with BMI 20-25. A more recent NSQIP analysis by Lee et al 16 found that BMI >40 was associated with increased odds of major adverse events, wound complications, and readmission, while underweight BMI had greater odds of prolonged length of stay and unplanned readmission. These findings are consistent with our results in terms of SSOs and complications. In contrast, our study modeled BMI as a continuous variable and accounted for different operative approaches including robotic data, thus providing more granular risk stratification and better reflects current practice patterns.
Prior studies comparing operative approaches in patients with obesity have reported mixed findings, with laparoscopic repair often associated with fewer SSOs and complications in prior NSQIP analyses,17,18 while small retrospective studies of robotic repair have shown either no difference in complications or lower complication rates compared with open repair.11,19 On the other hand, our analysis incorporating robotic and combined approach demonstrates that combined approach is associated with substantially higher odds of SSOs and major complications compared with open across BMI strata, likely reflecting increased case complexity. Both laparoscopic and robotic repairs were independently associated with lower odds of SSOs and major complications with robotic approach potentially offering additional benefit over laparoscopic approach.
Limitations
This study has several important limitations. First, its retrospective design using ACS-NSQIP limits causal inference and is subject to residual confounding and selection bias. Second, the NSQIP database lacks granular operative details; CPT codes identify the procedure category but do not distinguish specific repair techniques, mesh use, or other technical factors, which may vary by surgeon or institution and influence outcomes. Additionally, while the cohort includes heterogeneous patient populations, including femoral hernias and a small proportion of urgent/emergent cases (<7%), our multivariable models adjust for case acuity and operative approach, mitigating potential confounding. These broad inclusion criteria were intentional to reflect the full spectrum of groin hernia surgery as it relates to patients with obesity. Furthermore, given that operative approach may lie on the causal pathway between BMI and postoperative outcomes, our multivariable models including operative approach therefore only estimate the direct effect of BMI conditional on the approach used, rather than the total effect of BMI on outcomes. Finally, NSQIP captures outcomes only within 30 days, precluding assessment of long-term and hernia-specific endpoints such as recurrence and chronic pain.
Conclusion
In our 2022-2023 ACS-NSQIP analysis, obesity and higher BMI were associated with greater operative complexity and worse 30-day outcomes after inguinal hernia repair, with risk increasing most noticeably above certain BMI levels. Increasing BMI also corresponded with longer operative times and greater use of robotic and combined approaches. Importantly, minimally invasive approaches (laparoscopic and robotic) were associated with lower odds of SSOs and major complications compared with open repair, while combined approach carried highest risk, likely reflecting increased case complexity. These findings support individualized risk stratification, targeted preoperative optimization, and thoughtful approach selection for patients with obesity undergoing inguinal hernia repair.
Supplemental Material
Supplemental material - Impact of Obesity on Surgical Approach and Outcomes in Inguinal Herniorrhaphy: An ACS-NSQIP Analysis
Supplemental material for Impact of Obesity on Surgical Approach and Outcomes in Inguinal Herniorrhaphy: An ACS-NSQIP Analysis by Sachin N Reddi, BS, Li Ding, MD, PhD, Brynne A Ichiuji, MD, Simon Akhnoukh, MD, Katie Galvin, MD, Sharon Shiraga, MD, Stuart A Abel, MD, Luke R Putnam, MD, MS, and Harry J Wong, MD, MS in The American Surgeon™
Footnotes
Ethical Considerations
This study was approved by the University of Southern California Institutional Review Board, and the requirement for informed consent was waived due to the retrospective, deidentified nature of the data.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for Advancing Translational Science (NCATS) of the National Institutes of Health under award number UL1TR001855. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.