
Abstract
Reduced life expectancy in rheumatoid arthritis (RA) has been recognised since the 1950s, with standardised mortality rates (SMRs) of 1.41 for females and 1.08 for males. Extensive studies worldwide, including in India, have attributed this to a high prevalence of atherosclerotic cardiovascular disease (ASCVD) in RA. The increased ASCVD risk in RA and other inflammatory rheumatic and musculoskeletal diseases (I-RMDs) is influenced not only by conventional ASCVD risk factors (such as hypertension, diabetes mellitus, obesity, smoking, physical inactivity, and family history) but also by the degree and duration of systemic inflammation, as indicated by high-sensitivity C-reactive protein (hs-CRP) levels. Therefore, preventing ASCVD in RA and other I-RMDs has become a critical responsibility for rheumatologists. A two-pronged strategy is recommended: (a) strict lipid control and (b) stringent management of systemic inflammation, measured by hs-CRP levels.
This article summarises the Lipid Association of India (LAI) guidelines for preventing ASCVD in RA and other I-RMDs, which can be implemented by specialist rheumatologist-nurse-led teams in rheumatology clinics and departments.
Keywords
Introduction
Reduced life expectancy in patients with rheumatoid arthritis (RA) has been observed since the 1950s, 1 with standardised mortality rates (SMRs) of 1.41 for females and 1.08 for males. 2 An important contributor to this reduced life expectancy is the increased prevalence of conventional risk factors for atherosclerotic cardiovascular disease (ASCVD), including hypertension, diabetes mellitus, obesity, smoking, physical inactivity, and family history.3,4 More recently, this increased ASCVD risk has been recognised across nearly all autoimmune diseases.5,6 Given this context, monitoring and managing ASCVD risk in RA and other immune-mediated rheumatic and musculoskeletal diseases (I-RMDs) has become a key responsibility of rheumatologists. This subject has been extensively reviewed, highlighting the critical role of caregivers in preventing ASCVD in these conditions. 7 Consequently, the European Alliance of Associations for Rheumatology (EULAR) published recommendations for ASCVD prevention in patients with RA and other I-RMDs in 2016 and updated them in 2022.8,9
Specific Features of ASCVD in Indians
India is at the epicentre of the global cardiovascular disease epidemic.10,11 This trend is evident in the incidence rates of ASCVD among Indian patients with RA, as reported in multiple studies.12-16 These studies have highlighted an increased prevalence of subclinical atherosclerosis and endothelial dysfunction in Indian RA patients. In fact, a significant proportion of RA patients in Asia, including India, exhibit ASCVD, with reports indicating its presence in 15% of these patients. These findings underscore the unique cardiovascular risk profile in the Indian population, further emphasising the need for targeted prevention and management strategies.
Aim of the Review
This review aims to provide a stepwise approach for:
Assessing ASCVD risk in Indian patients with RA and other I-RMDs using the Lipid Association of India (LAI) guidelines, specifically tailored for these populations.
17
Implementing LAI guidelines for targeted lipid management to achieve optimal levels for ASCVD prevention in these diseases. Discussing a research agenda that includes:
Evaluating whether these recommendations effectively reduce ASCVD risk in real-life scenarios and identifying additional interventions needed beyond lipid management. Investigating the ideal strategies to mitigate ‘residual inflammation’, which has increasingly been recognised as a key contributor to ASCVD.
18
Exploring the practicality of implementing the comprehensive LAI guidelines in busy outpatient rheumatology clinics and considering the use of simpler tools, such as the ‘QRISK-3 lifetime’ calculator, for routine ASCVD risk assessment.
19
ASCVD Risk Assessment in RA and Other I-RMDS
The most widely used cardiovascular risk calculators globally are the ‘Systematic Coronary Risk Evaluation’ (SCORE) calculator and the Framingham Risk Score (FRS).20,21 However, studies have shown that applying these risk calculators, developed for the general population, to patients with RA and other I-RMDs often results in significant underestimation of ASCVD risk.22-26 This discrepancy arises due to several factors, including the predominance of female patients in specific age ranges, the impact of systemic inflammation, and the use of medications like glucocorticoids, which increase ASCVD risk but are not accounted for in these general risk scores. As a result, despite EULAR recommendations, alternative risk scores tailored for RA and I-RMDs have been explored.
Calculating Lifetime Risk of ASCVD
Due to the reasons discussed above, the SCORE and FRS were found to be unsatisfactory for assessing ASCVD risk in patients with RA and other I-RMDs.21,22 This highlighted the need for a scoring system that incorporates the specific characteristics of these patients. The ‘QRISK’ score, developed by researchers at the University of Nottingham, UK,
19
appeared to be the closest to an ideal calculator for RA and I-RMDs, as it includes key factors such as specific diagnoses (e.g., RA, SLE) and glucocorticoid use, which are particularly relevant to rheumatologists. Another notable feature of the QRISK system is its validation among individuals of Indian ethnicity, which adds to its applicability for the Indian population. Recently, the QRISK score was validated in Indian patients with RA,
27
further supporting its utility, although the study used carotid intima-media thickness (IMT) as a surrogate marker of cardiovascular risk, a method that has some controversy.28,29 Additionally, QRISK-3 has been validated in patients with systemic lupus erythematosus (SLE), adding to its versatility.
30
The LAI has also recommended the QRISK-3 calculator for the Indian population, making it a suitable tool for estimating lifetime ASCVD risk in RA and other I-RMDs among Indian patients.
17
The QRISK-3 calculator is also freely available online for routine use (QRISK→3-2018 risk calculator:
ASCVD Risk Assessment in RA and Other I-RMDS in Indian Patients
Recommendations of the LAI. 17
ASCVD major risk factors:
Age: >45 years in males; >55 years in females Current cigarette smoking or tobacco use* High blood pressure >140/90 mm Hg or, on antihypertensive drugs Low HDL-C (values not defined; international figures for non-South Asians is <40 mg/dL. Given the elevated high risk of ASCVD in South Asians, the figures of <50 or <60 mg/dL may be more appropriate).
31
*‘Bidis’, ‘Paan with zarda’, ‘gutka’, other similar tobacco, and other forms of tobacco used in India.
ASCVD major risk modifiers:
Lipoprotein (a) 120-149 mg/dL. Impaired fasting glucose 100-125 mg/dL (on repeated testing). Increased waist circumference >90 cm in males, >80 cm in females (when measured at the superior border of Iliac crest). High-sensitivity C-reactive protein (hs-CRP) level >2 mg/L measured at least on two occasions two weeks apart. Plasma triglycerides >150 mg/dL fasting or >175 mg/dL non-fasting. Presence of rheumatoid arthritis, psoriasis or spondyloarthropathies. Premature menopause, pre-eclampsia, gestational diabetes, polycystic ovarian syndrome. Human immunodeficiency virus infection. Air pollution. High polygenic risk score.
Categorising patients in different degrees of lifetime ASCVD risk based upon the recommendations of LAI17:
0-1 major risk factor (as listed above)
and
LDL-C 100-129 mg/dL
and
Non-HDL-C 130-159 mg/dL
and
Lifetime ASCVD risk <30% (as calculated by QRISK-3 calculator)
Two major ASCVD risk factors (as listed above)
or
LDL-C 130-159 mg/dL
or
Non-HDL-C 160-189 mg/dL
or
Low-risk group with >1 risk modifier or lifetime ASCVD risk >30%
Three or more major ASCVD risk factors (as listed above)
or
LDL-c 160-189 mg/dL
or
Non-HDL-C 190-219 mg/dL
or
Diabetes with 0-1 major ASCVD risk factor (as given above)
or
Two major ASCVD risk factors + > 1 ASCVD risk modifiers (as listed above)
or
Any 1 ASCVD high-risk feature (as listed above)
Diabetes with target organ damage Diabetes with >2 major ASCVD risk factors Coronary artery calcium score (CACS) 100-299, or >75th percentile if CACS 1-99 >2 ASCVD high-risk factors (as listed above) Established ASCVD (stenotic or nonstenotic carotid, femoral or coronary arterial plaques as well as ankle-brachial index <0.9 in either leg). LDL-C > 190 mg/dL or heterozygous for familial hypercholesterolaemia
ASCVD with > 1 high-risk group CACS > 300 Homozygous for familial hypercholesterolaemia
ASCVD with
>1 feature of ‘Very High Risk’ group (above) Recurrent acute coronary syndrome Polyvascular disease Homozygous for familial hypercholestero-laemia Recurrent ASCVD despite LDL-C level around 30 mg/dL
Statin therapy is recommended for all patients at risk of ASCVD. The intensity of treatment and the lipid targets to be achieved are determined by the patient’s lifetime ASCVD risk, which is categorised into different risk levels. Statin therapy is classified into three intensity levels as follows:
32
Low-intensity statin (LIS) dose: The statin dose that would achieve <30% reduction in LDL-C level. Moderate intensity statin (MIS) dose: The statin dose that would achieve 30-<50% reduction in LDL-C level. High-intensity statin (HIS) dose: The statin dose that would achieve >50% reduction in LDL-C level.
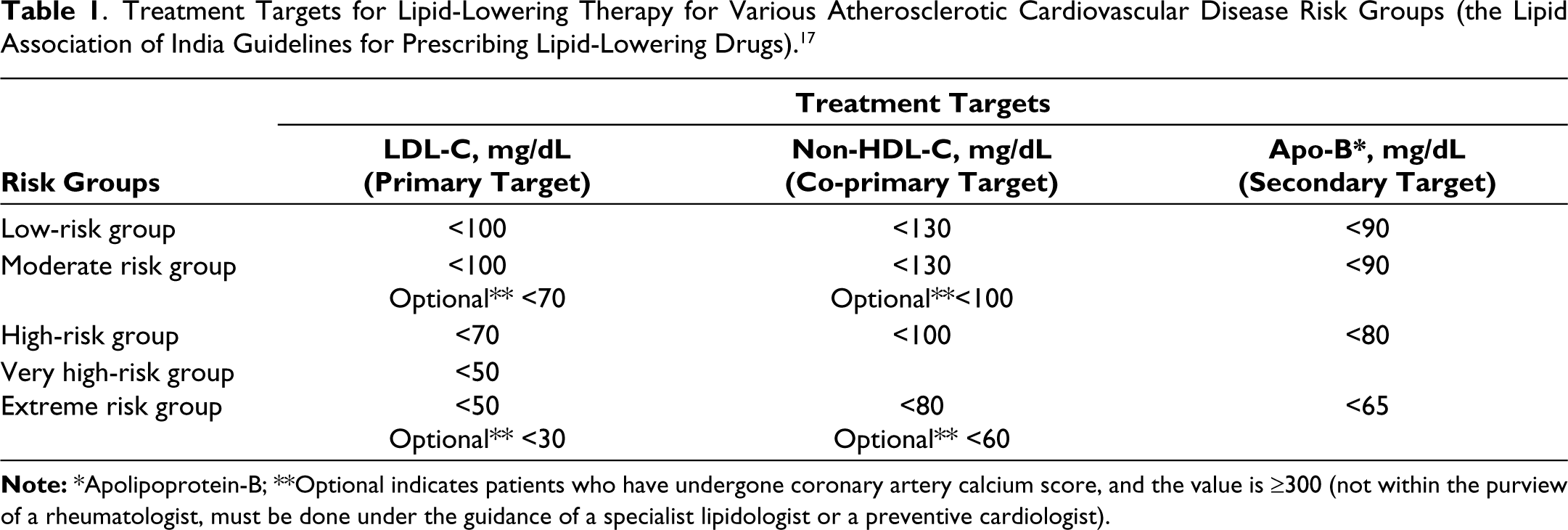
The intensity of treatment and the need for additional medications depend on the patient’s risk category and the desired extent of LDL-C reduction. The ASCVD risk reduction strategy involves a combination of lifestyle interventions and the use of lipid-lowering drugs to achieve the targets recommended by the LAI, as detailed in Table 1.
Lipid-Lowering Treatment in Patients with RA and Other I-RMDs
General measures:
Patient education and counselling: Emphasise the importance of understanding cardiovascular risk, adherence to treatment, and lifestyle modifications. Healthy lifestyle: Encourage a balanced diet and regular physical activity to maintain weight control and reduce abdominal girth. Smoking cessation: Counsel patients against all forms of smoking.
Drug treatment:
Statins:
Statins are the first-line treatment for achieving target LDL-C levels in patients with RA and other I-RMDs. The intensity of statin therapy is determined by the patient’s cardiovascular risk profile, with the goal of reaching the recommended LDL-C (or non-HDL-C) target levels. Combination therapy:
If the target LDL-C level is not achieved with statins alone, combination therapy with ezetimibe is recommended. PCSK9 inhibitors:
For patients at very high cardiovascular risk who have persistently elevated LDL-C levels despite maximum tolerated doses of statins combined with ezetimibe, PCSK9 inhibitors are recommended. For patients who still fail to meet treatment targets, the use of additional medications, such as bile-acid sequestrants or bempedoic acid, should be considered. This should be done in collaboration with a lipidologist or preventive cardiologist experienced with these therapies.
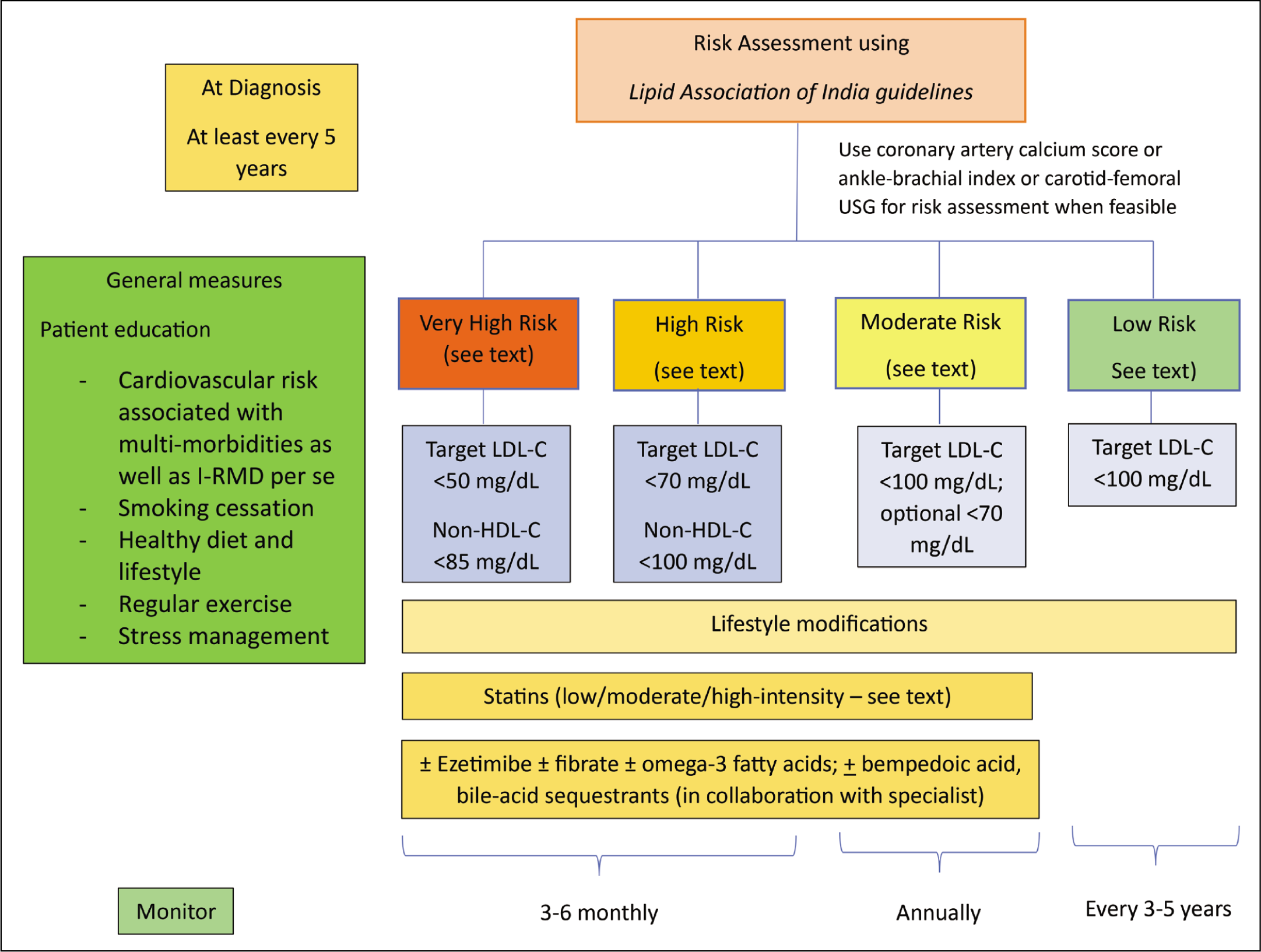
Figure 1 provides a summary of the recommendations for preventing ASCVD in RA and other I-RMDs.
Visual Summary of the Guidelines of the Lipid Association of India.
Discussion
The heightened risk of ASCVD in individuals with RA and immune-mediated rheumatic diseases (I-RMDs) is now widely recognised and reported globally. A significant study from the UK, involving 22 million individuals, investigated 19 autoimmune diseases and 12 cardiovascular diseases, further confirming this elevated risk. 5 Similar findings have been reported in publications from India,10-15 including a recent international study that incorporated Indian patients. 16 However, there is a notable scarcity of guidelines on assessing and managing lifetime ASCVD risk specifically for Indians with RA and other I-RMDs. To date, only one study has compared cardiovascular disease risk prediction scores and evaluated subclinical atherosclerosis in Indian patients with RA. 27 This study found that the QRISK score is satisfactory for estimating lifetime ASCVD risk in Indian RA patients. It is important to note that this study used carotid IMT as a surrogate marker for ASCVD, a method that has limitations in providing a comprehensive assessment.28,29 There are two consensus statements from India regarding the assessment of ASCVD risk and lipid management in Indian patients.17,33 Of these, the LAI provides detailed recommendations specifically for RA and other I-RMDs, which this review endorses. 17
This review aims to raise awareness among Indian rheumatologists about the heightened ASCVD risk in patients with RA and other I-RMDs. It provides guidelines for assessing ASCVD risk in rheumatology clinic patients and emphasises the appropriate use of statins and other lipid-lowering medications, as outlined by the LAI. 17 These recommendations have been summarised in Table 1 and Figure 1.
Treatment Targets for Lipid-Lowering Therapy for Various Atherosclerotic Cardiovascular Disease Risk Groups (the Lipid Association of India Guidelines for Prescribing Lipid-Lowering Drugs). 17
In a busy rheumatology outpatient clinic, there is a tendency for rheumatologists to seek alternatives to the time-consuming process of using the LAI guidelines for estimating lifetime ASCVD risk. One such alternative is the ‘QRISK’ score, particularly its third version, QRISK-3. 19 This tool is not only readily available online, making it convenient for outpatient use, but it also incorporates a wide range of factors, including age, sex, ethnicity, and common diseases that increase ASCVD risk—such as diabetes, coronary artery disease, chronic kidney disease, atrial fibrillation, hypertension, migraine, severe mental illnesses (including the use of antipsychotic drugs), HIV infection, and erectile dysfunction. Most notably for rheumatologists, QRISK-3 accounts for glucocorticoid use and the presence of RA or SLE. Several reports have confirmed the utility of QRISK-3 for stratifying ASCVD risk, including in patients with SLE and RA.27,30
However, there is ongoing debate about the validity of QRISK-3 as the sole tool for ASCVD risk stratification, primarily because it does not account for the patient’s systemic inflammation status. Seminal studies by Ridker et al. have demonstrated that elevated levels of hs-CRP >2 mg/L are directly linked to ASCVD.34-36 These pivotal studies have established that systemic inflammation, indicated by elevated hs-CRP levels, plays a more significant role in ASCVD development than atherogenic lipids. Based on this evidence, ‘proof-of-concept’ trials with anti-inflammatory drugs, including canakinumab (a human IgGκ monoclonal antibody targeting interleukin-1β, a potent pro-inflammatory cytokine) and low-dose colchicine, have shown efficacy in preventing ASCVD.37-40 Following the results of these trials, the FDA has approved the use of low-dose colchicine for ASCVD prevention in the general population with hs-CRP levels >2 mg/L. 41
In a recently published study, we clearly demonstrated that QRISK-3 underestimates ASCVD risk, likely because it does not account for systemic inflammation in its calculation. 42 Our study revealed that, despite being in remission and receiving lipid-lowering treatment, 62% of our RA patients still had residual inflammatory risk (RIR), as indicated by hs-CRP levels >2 mg/L. 34
Research Agenda
Despite commendable efforts by researchers worldwide, including those from India, a significant gap remains in understanding the extent of ASCVD across different populations and races. 43 Most international guidelines and recommendations share similar limitations due to the absence of well-conducted, appropriately controlled long-term studies. This shortcoming is also evident in the two clinical practice guidelines from India.17,33 The current recommendations, guidelines, and consensus statements have relied on surrogates for ASCVD since there is no reliable method for directly measuring the extent of ASCVD in the body. Furthermore, in the absence of rigorously controlled long-term studies from India, the LAI and Cardiology Society of India (CSI) guidelines remain expert consensus statements, which is a significant limitation.
This observation also applies to many international guidelines, which suffer from similar drawbacks. Additionally, the existing guidelines are often cumbersome and time-consuming, making them impractical for routine use in busy outpatient clinics. Therefore, there is an urgent need for a simple tool that integrates all relevant variables related to ASCVD risk, is available online, and provides an accurate assessment of ASCVD risk for each patient. This would be the most practical way to ensure comprehensive ASCVD risk mitigation. Efforts are ongoing worldwide to measure the extent of atherosclerotic cardiovascular involvement using advanced imaging and genetic methods. 44
In summary, despite the existence of international and national consensus statements on blood lipid control for ASCVD prevention, several gaps remain in the field. Most large-scale, long-term studies have been conducted on populations from developed countries, which differ significantly from the Indian population. Given that India is at the epicentre of the ASCVD epidemic, applying these recommendations to Indian patients may result in undertreatment. Therefore, there is a pressing need for multicenter, long-term studies focused on patients with RA and other I-RMDs in India to better understand ASCVD in this population.
Accurate and reliable methods for assessing the extent of ASCVD involvement, such as advanced imaging techniques, must be explored and applied to Indian patients to ascertain their true ASCVD status. This will pave the way for the development of evidence-based guidelines specifically tailored to preventing ASCVD in individuals with I-RMDs. Major medical research and teaching institutions in India must rise to this challenge to mitigate ASCVD-related risks among Indian patients.
Footnotes
Acknowledgements
Authors would like to convey sincere thanks and acknowledge the help provided by the Associate Editor of this journal Dr D. P. Misra, for his inputs to improve the manuscript and for providing several key international articles that have included patients from India in studies of ASCVD in I-RMDs.
Clearance of the Institution’s Ethics Committee
Not required as it does not involve any human or animal subjects.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.