
Abstract
Objective:
To determine the status of ‘residual inflammatory risk’ (RIR) and ‘residual cholesterol risk’ (RCR) in patients with Rheumatoid Arthritis (RA) in remission with the aim of estimating their atheroscle-rotic cardiovascular disease (ASCVD) risk.
Methods:
The study included patients with RA in remission during their last two clinic visits on treatment with disease- mod-ifying anti-rheumatic drugs (DMARDs). Using the QRISK-3 calculator, participants were stratified into four risk categories for ASCVD: ‘Very high’, ‘High’, ‘Moderate’, and ‘Low’. Patients were prescribed lipid-lowering drugs targeting low-density lipoprotein cholesterol (LDL-C) levels to <50 mg/dl, <70 mg/dl, <100 mg/dl or <130 mg/dl, respectively. Those with a history of ASCVD before or during the follow-up period was excluded from the study. Multimorbidity were also recorded in all the patients.
Results:
The study included 130 patients with RA in remission. The results showed that despite being in remission and taking treatment for lipid control, 81 (62%) and 91 (70%) patients still had ‘RIR’ and ‘RCR’, respectively. Hypertension, hypothyroidism, type-2 diabetes mellitus and obesity were the common multimorbidity.
Conclusions:
Persistent RIR in 62% of patients despite being in remission, could possibly be due to the current ‘liberal’ definition of RA permitting hs-CRP level up to <10 mg/l, which is five-fold higher than the recommended <2 mg/l for ASCVD prevention. Hence it may be necessary to revise the definition of ‘remission’ in RA factoring in the suggested lower level of hs-CRP. Additionally, rheumatologists might need to be more vigilant in lipid management with appropriate patient education regarding RCR.
Keywords
In patients with RA in remission, 62% had ‘residual inflammatory risk’. Factoring for the ASCVD-protective <2 mg/L hs-CRP level, RA definition of ‘remission’, may require revision. Additionally, rheumatologists must aim for more stringent lipid control with drugs and patient education.Key Messages
Introduction
Patients with rheumatoid arthritis (RA) have a substantially reduced life expectancy. The standardised mortality ratio (SMR) has been reported to range from 1.13 to 2.98, the main cause of which is increased atherosclerotic cardi-ovascular disease (ASCVD).1–5 Higher risk of developing premature aggressive ASCVD-related outcomes is also well documented in other immunoinflammatory disorders.6,7 Therefore, prevention of ASCVD has become a major responsibility for rheumatologists. The role of atherogenic blood lipids in the causation of ASCVD is well established.8–11 Seminal lipid-lowering statin trials of 1990s for preventing ASCVD are also widely known in the field of preventive medicine.12,13 Therefore, statin treatment for its prevention, mainly targeting low-density lipoprotein cholesterol (LDL-C), is the current treatment paradigm, 14 recommended by international/national (including India) recommendations/guidelines.15–18
Since 1997, the additional role of inflammation, measured by high-sensitivity C-reactive protein (hs-CRP), as a causative factor for ASCVD has been extensively studied and reported by Braunwald’s group at Harvard, led by Paul Ridker and colleagues including JUPITER study and the CANTOS trial, a proof-of-concept study.19–22 These workers have defined achieving the blood level of hs-CRP (as a surrogate for systemic inflammation) for the prevention of ASCVD to be <2 mg/l. 23 There is now evidence that direct suppression of inflammation mitigates ASCVD risk. 24 Thus, lipid-lowering (mainly LDL-C) therapies in combination with controlling systemic inflammation are now considered ideal for the prevention of ASCVD.25,26
The terms ‘residual cholesterol risk’ (RCR) and ‘residual inflammatory risk’ (RIR) have been coined by Ridker for patients not achieving the recommended LDL-C levels (vide infra) and hs-CRP levels (<2 mg/l), despite appropriate treatment. 27 In spite of such clear evidence of inflammation playing a crucial role in causing ASCVD, possibly even more significant than atherogenic lipids, 26 current treatment guidelines for the prevention of ASCVD in general populations as well as in SIRDs including RA and others, do not recommend additional anti-inflammatory therapy, over and above statins.28,29 This may be due to the inherent anti-inflammatory effects of statins, which are considered fortuitous among their pleiotropic effects. 30
The present observational study was conducted on patients with RA under follow-up in the outpatient clinic of this department to find out whether they had achieved the target levels of LDL-C and/or hs-CRP as per recommenda-tions/guidelines cited vide supra, and how many patients still carried ‘RIR’ and ‘RCR’.
Aims and Objectives
This study aimed to investigate the proportion of patients with RA who, despite meeting the updated remission criteria during their last two clinic visits, 31 did not achieve the target levels of LDL-C and hs-CRP. The objective of the study was to find out what proportion of patients continued to carry RIR and/or RCR.
Patients and Methods
The study included clinically diagnosed and ACR/EULAR-classified 32 patients with RA. Only those patients who were in complete remission at the last two outpatient rheumatology clinics were included. They had received DMARD treatment as recommended by international guidelines 33 and its previous versions (in patients who have been in the follow-up for a longer duration), aiming for ‘remission’ (based upon Simplified Disease Activity Index {SDAI} composite index). 34 The study excluded patients who had had any form of ASCVD in the past or during the follow-up in this clinic. Multi-morbidities if any were also recorded.
The rheumatology department of this hospital had obtained approval from the hospital’s Ethics Commit-tee to carry out ‘clinical data mining’ for research purposes. The condition for this research has been strict anonymity, ensuring that patient identities are never revealed. Consequently, the necessary information was extracted and stored in a password-protected ‘Excel’ sheet, accessible only to the researchers involved in this study.
Treatment for Lipid Control
A two-step approach was followed. First step was to calculate the ‘10-year risk for ASCVD’ using ‘QRISK-3’ calculator,
35
available online (QRISK→3-2018 risk calculator ‘Very High Risk’: QRISK-3 score ‘>20%’ 10-years ASCVD risk or, clinically diagnosed/established ASCVD on treatment, bypass surgery done, or coronary stenting done—under cardiology follow-up. ‘High Risk’ for ASCVD: Do not have clinically established ASCVD, but QRISK-3 score ‘10- to <20%’ 10-year ASCVD risk. ‘Moderate ASCVD risk’: Do not have clinically established ASCVD, but QRISK-3 score ‘5- to <10%’ 10-year ASCVD risk. ‘Low ASCVD risk’: Do not have clinically established ASCVD, QRISK-3 score ‘<5%’ 10-year ASCVD risk.
In the second step, the patients were prescribed lipid-lowering drugs to achieve the following targets of LDL-C stratified in different risk categories as has been recommended by the Indian guidelines for lipid con-trol:17,18
In those at ‘very high ASCVD risk’ LDL-C target to be achieved was <50 mg/dl. In those at ‘high ASCVD risk’, LDL-C target to be achieved was <70 mg/dl. In those at ‘moderate ASCVD risk’, LDL-C target to be achieved was <100 mg/dl. In those at ‘low ASCVD risk’, LDL-C target to be achieved was <130 mg/dl.
Results
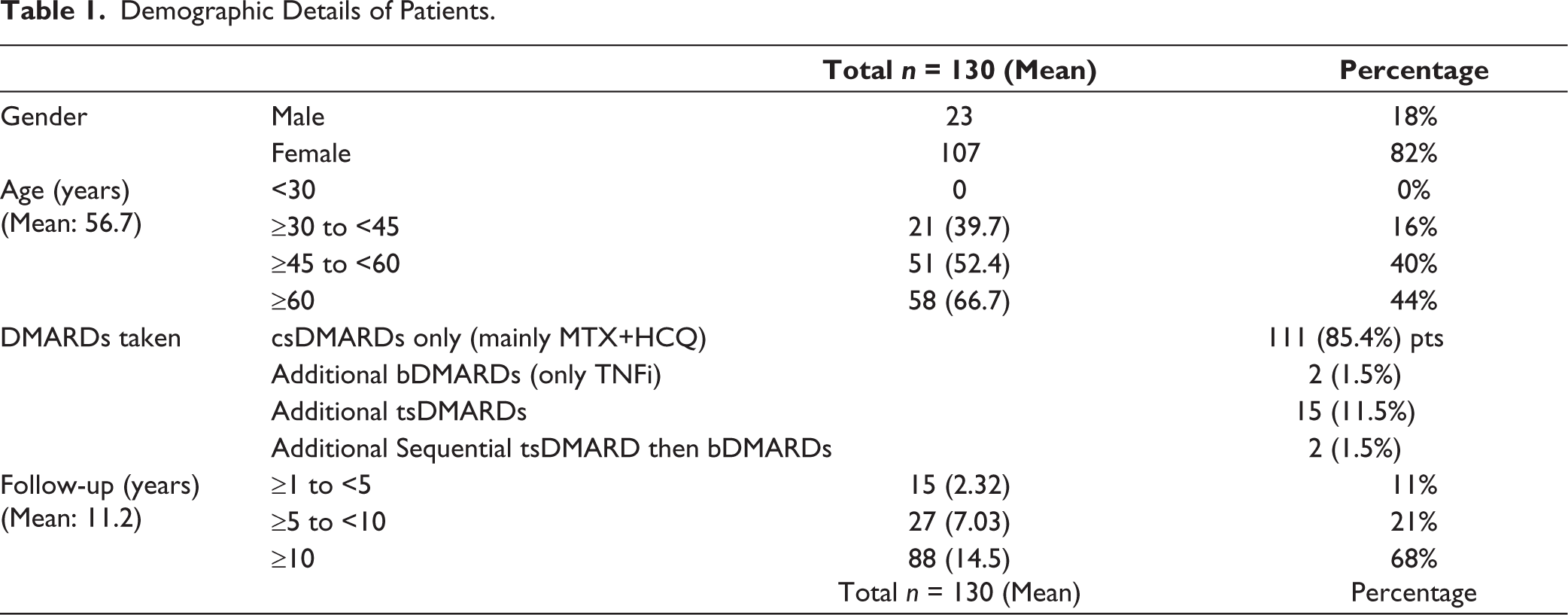
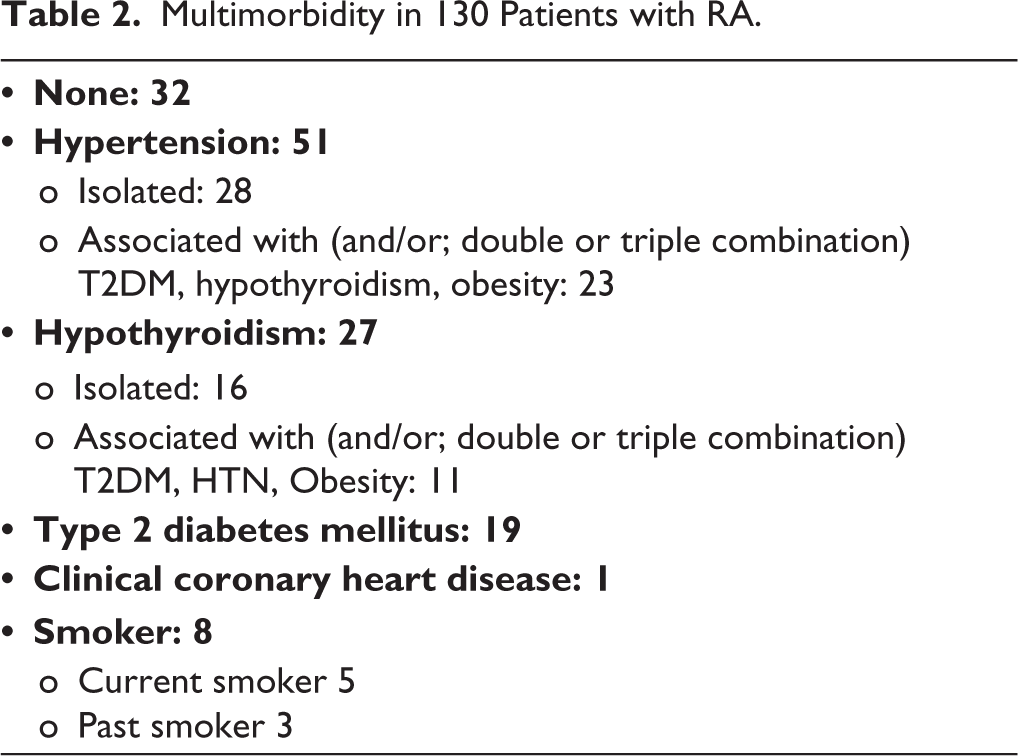
In this study, 130 patients diagnosed with RA and meeting the ACR/EULAR classification criteria, 32 were included. Table 1 provides demographic information about the study subjects, treatment taken type of Disease-Modifying Antirheumatic Drugs (DMARDs) taken, including conventional synthetic DMARDs (csDMARDs), targeted synthetic DMARDs (tsDMARDs; either tofacitinib or baricitinib) and biological DMARDs (bDMARDs); and the duration of their follow-up. Notably, all participants were receiving appropriate treatment with DMARDs as per the ‘treat-to-target’ approach. 33 These patients had met the criteria for remission at the time of their last two fol-low-up clinic visits. 31 Multimorbidity present in patients with RA included in this work, are given in Table 2. The results detailing hs-CRP levels and LDL-C are provided in Table 3. Notably, 81 patients (62%) were classified as having ‘RIR’ despite being in ACR/EULAR definition of remission. Similarly, 91 patients (70%) who were categorised as having ‘RCR’, despite rigorous lipid control measures guided according to their ‘10-year risk for ASCVD’ that included intensive statin therapy, frequently combined with ezetimibe treatment.
Demographic Details of Patients.
Multimorbidity in 130 Patients with RA.
LDL-C and hs-CRP Blood Levels of Patients at the Last Clinic Visit.
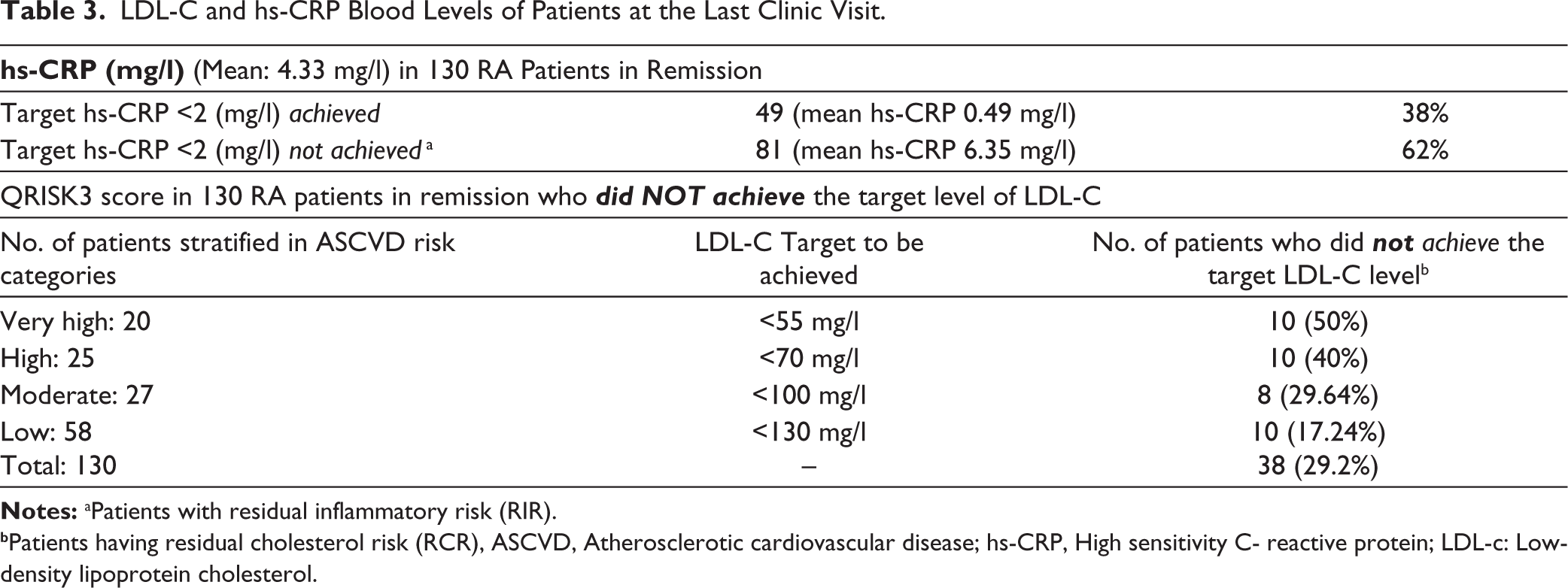
bPatients having residual cholesterol risk (RCR), ASCVD, Atherosclerotic cardiovascular disease; hs-CRP, High sensitivity C- reactive protein; LDL-c: Low-density lipoprotein cholesterol.
Discussion
Prevention of ASCVD in RA (as well as in other rheumatic and musculoskeletal diseases) is currently recommended by international guidelines as part of appropriate management.28,29 The results of the present study showed two shortcomings in achieving this goal. First, despite efforts to bring down atherogenic blood lipids to recom-mended target levels, a large majority of patients did not achieve the specified treatment goal. This observation indi-cates that the treating rheumatologists, possibly did not monitor the blood lipid levels frequently or did not pay ade-quate attention to this aspect of treatment. The other possibility could be a lack of appropriate patient education re-garding the prevention of ASCVD that could have led to drug default. The second observation related to ‘systemic inflammation’, is even more disturbing. The present study showed that 62% of patients, even though in remission, exhibited hs-CRP levels ranging from 2 to <10 mg/l. This range, classified as RIR within the context of ASCVD, underscores the persistent low-grade inflammatory state despite their RA being in remission. Studies quoted vide supra23,24 have shown that in normal population, hs-CRP levels in RIR range result in higher risk for ASCVD. In this regard, it is important to note that the current formal definition of remission in RA allows for hs-CRP level up to 10 mg/L. 31 Thus, RIR is in-built in latest recommended definition of remission in RA. This finding raises the possibility of RIR being the cause of ‘residual life-expectancy gap’ because even with the availability of effective drugs and ‘treat-to- target’ approach, there still remains a mean loss of life expectancy of 4.97 years in patients with RA. 38
The present study has limitations. It is only a small preliminary report from the standpoint of prevention of ASCVD in patients with RA. At the most, it can be considered a ‘hypothesis generating’ observational work. Till today there are no major long-term follow-up population studies on RA that have proven further reduction of ASCVD rate in those who achieve hs-CRP levels of <2 mg/l. Well-designed large studies with long-term follow-up would be required to prove/disprove whether the proposed hs-CRP recommendations (targeting <2 mg/l levels) along with the current lipid recommendations for the prevention of ASCVD in RA and other RMDs are successful or not. Another limitation of the present work is that the targets for lipid control used in the present work are based upon recommendations for normal Indian population. 17 Yet, Curtis and colleagues have demonstrated that ASCVD risk in RA is ~ 1.5 times higher than normal. Therefore, treating hyperlipidaemia to targets set for normal population may not be correct. However, the support of the lipid target used in this work derives from specific use of ‘QRISK-3’ instrument that has factored for glucocorticoid use, as well as diseases like RA 35 and SLE 36 thus offsetting some of the disadvantages of using targets recommended for normal population. ‘QRISK-3’ has also been specifically recommended for the patients of Indian ethnicity. 37
In conclusion, this preliminary work demonstrates that the treating rheumatologists may not be critically and fre-quently examining the atherogenic lipid profile of the patients with RA (and possibly other RMDs) and educating them regarding ASCVD and the need for prevention with appropriate drug treatment. This study also brings out a clear dis-crepancy between the recommended lower target level of hs-CRP for ASCVD prevention (<2 mg/l) versus the permitted level of hs-CRP <10 mg/l in the definition of remission in RA. International bodies like EULAR, may like to investigate/revise this aspect of the definition of ‘remission in RA’.
Footnotes
Acknowledgements
Authors would like to sincerely thank colleague Consultant Rheumatologists Drs Sanjiv Kapoor and Shriram Garg for their encouragement and cooperation. We also acknowledge the help provided by Secretarial Assistants Ms Pinki Negi-Bisht and Miss Deepa in writing this article. We gratefully acknowledge the help extended in data analysis by Ms Nishtha Agarwal, Senior Research Fellow, Department of Basic Research at this hospital.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.