
Abstract
Introduction:
Peripheral ischemic lesions in rheumatic diseases have variable presentations, prognoses and outcomes that have not been well studied in published literature. The present study aimed to investigate the clinical presentation, aetiology, prognosis and outcomes of peripheral ischemic lesions in rheumatic diseases.
Material and methods:
A medical records review of all patients who presented with peripheral ischemic lesions was conducted in the Department of Clinical Immunology and Rheumatology of a tertiary care institution in Northern India. Data from March 2013 to December 2017 was collected in the form of demographic and clinical details, investigations, treatment and outcomes.
Results:
Of 103 patients that presented with peripheral ischemic lesions, 80 (77.6%) had an underlying rheumatic disease. In the group with rheumatic causes, the mean age was 29.31 years, and the majority (87%) presented in the winter season. The most common rheumatic cause was vasculitis (55%) followed by systemic sclerosis (17.5%), systemic lupus erythematosus (15%) and primary antiphospholipid antibody syndrome (6, 7.5%). Amputation (either surgical or auto-amputation) was observed in 55% of the cases, while the remaining recovered completely or near completely with medical treatment.
Conclusions:
Peripheral ischemic lesions may present as the initial or predominant manifestation of rheumatic disease with vasculitis being the most common cause. Late referral or presentation to the hospital, delayed specific management and presentation as gangrene resulted in poorer outcomes in these patients.
Introduction
Peripheral ischemic lesions encompass a wide spectrum of aetiologies, including rheumatic diseases, atherosclerosis, diabetes mellitus, infection, etc. These lesions present as the predominant manifestation or as an initial manifestation of a rheumatic disease which poses a challenge for its diagnosis and appropriate management. It often leads to extensive investigations, blanket therapies and delayed institution of targeted therapy. 1
Most studies have focused on peripheral ischemia in the setting of a particular rheumatic disease with a prevalence of 31.8% in vasculitis like Polyarteritis Nodosa (PAN), 8%–9% in systemic sclerosis (SSc) and 2%–5% in systemic lupus erythematosus (SLE).2–6 Even amongst rheumatic diseases, the mechanism of peripheral ischemia is multifactorial ranging from vasculitis, vasculopathy to accelerated atherosclerosis.3, 5, 7, 8 Peripheral ischemic lesions are the presenting features of small to medium-sized vasculitides like PAN and Antineutrophil Cytoplasmic Antibody (ANCA)-associated vasculitis.9, 10 They can be occasionally observed in large vessel vasculitis like Takayasu arteritis. 11 Other than the direct inflammatory affection of the vessel wall leading to vascular occlusion, vasculitis also forms an intense inflammatory state resulting in hypercoagulability. Thus, thromboembolic gangrene may also be observed in these patients. 12 In patients with SSc pathophysiology of ischemic lesions is better understood and it is believed to be secondary to the endothelial injury with resultant smooth muscle proliferation due to a disbalance between vasodilators such as prostacyclin and nitric oxide and vasoconstrictors such as endothelin and vascular endothelial growth factor in favour of the latter.13–15
There is a paucity of epidemiologic studies depicting a bird’s eye view of the common aetiologies of peripheral ischemia in a rheumatology clinic. A single-centre study from Western India reported 22 cases of connective tissue disease-associated gangrene with the most common cause being mixed connective tissue disease. 16 They have variable presentations and outcomes ranging from complete recovery to amputation. These factors have been largely undefined in the literature. Hence, we aimed to study the aetiology, clinical features and outcomes of peripheral ischemic lesions in patients presenting to the rheumatology unit in a tertiary care hospital in Northern India.
Methods
Aim
To study the aetiology, clinical features and outcomes of peripheral ischemic lesions in patients presenting to the rheumatology department.
Design
A medical records review in a retrospective manner was conducted in the Department of Rheumatology at a tertiary care hospital in Northern India from March 2013 to December 2017.
Inclusion and Exclusion Criteria
All patients presenting to the rheumatology unit with peripheral ischemic lesions with a rheumatic or unclear cause were included. Those with clear non-rheumatic or infectious aetiology and those referred to other departments and intensive care units were excluded.
Methods
Data of all patients with peripheral ischemic lesions was retrieved from patient files colour-coded and stored as per their diagnosis. Details were recorded in the form of patient demographics (age, sex, co-morbidities, i.e., diabetes, hypertension, renal failure, Coronary Artery Disease (CAD)), the season of presentation, type of lesion (pre-gangrenous/gangrenous lesion), specific aetiology (rheumatic/non-rheumatic), the time interval between presentation of ischemic lesions and initiation of treatment. Investigations for the aetiology of ischemic lesions were carried out as per treating physician’s discretion. Arterial Doppler was done in all cases with comorbidities or a history of smoking and on a case-to-case basis in the others. Gangrene was defined as blackish discolouration of tissue due to a lack of blood supply with a complete absence of movement, and sensations in the affected part (Rutherford grade III). Pregangrene was defined as numbness, tingling, severe pain and discolouration of the affected area with impending gangrene. Patients with both gangrene and pregangrene, they were classified to have gangrene as it is the more severe of the two manifestations (Rutherford grade II). 17
Statistical Analysis
The data were checked for normality and expressed as mean ± SD. Quantitative variables were analysed by student t-test test based on normality assessment and qualitative by chi-square/fisher exact test between outcomes (amputation versus recovery). Comparisons across rheumatic diseases (vasculitis, SLE, primary antiphospholipid antibody syndrome [APS], SSc/mixed connective tissue diseases [MCTD]) were done using for quantitative variables and qualitative by chi-square/fisher exact test. For rheumatic diseases, secondary APS with SLE as the primary disease was grouped with SLE; PAN, ANCA vasculitis, unclassified vasculitis, RA vasculitis, Takayasu arteritis and cryoglobulinemia were grouped under vasculitis; and SSc and MCTD were grouped together. Clinically relevant parameters were selected as covariates (age, sex, comorbidities and smoking status, type of rheumatic disease, type of lesion, presenting manifestation or not, delay in presentation, delay in institution of specific therapy) for multivariate analysis (binary logistic regression) using the forward likelihood ratio test with the outcome as the dependent variable. The p value <.05 was considered statistically significant. SPSS version 24 (Chicago, Inc., USA) was used for statistical analysis. The study was approved by the Institutional Ethics Committee at King George’s Medical University (658/ethics/2020) with an exemption for patient consent in view of the retrospective design.
Results
Demographics
A total of 103 patients presented with peripheral ischemic lesions with a mean age of 29.31 years with a female-to-male ratio of 3.2:1. Out of these, 80 (78%) patients had an underlying rheumatic disease (Figures 1 and 2). Amongst those with rheumatic diseases, 17 (21.3%) were children, and the majority (87.5%) presented in the winter. Associated comorbidities in the form of hypertension, diabetes mellitus and hypothyroidism were present in 16 patients (20%) and 12 (15%) were ever smokers. All but two patients had good glycemic control based on fasting and post-meal blood sugar or glycosylated haemoglobin levels (one each with PAN and ANCA-associated vasculitis). None of the 89 patients tested for hepatitis B surface antigen, anti-hepatitis C antibody and Human immunodeficiency virus serology were positive. Of the 23 with non-rheumatic aetiology, 9 had diabetes-related atherosclerosis, 9 had Buerger’s disease, three with unclear aetiology and two had atheroembolic disease.
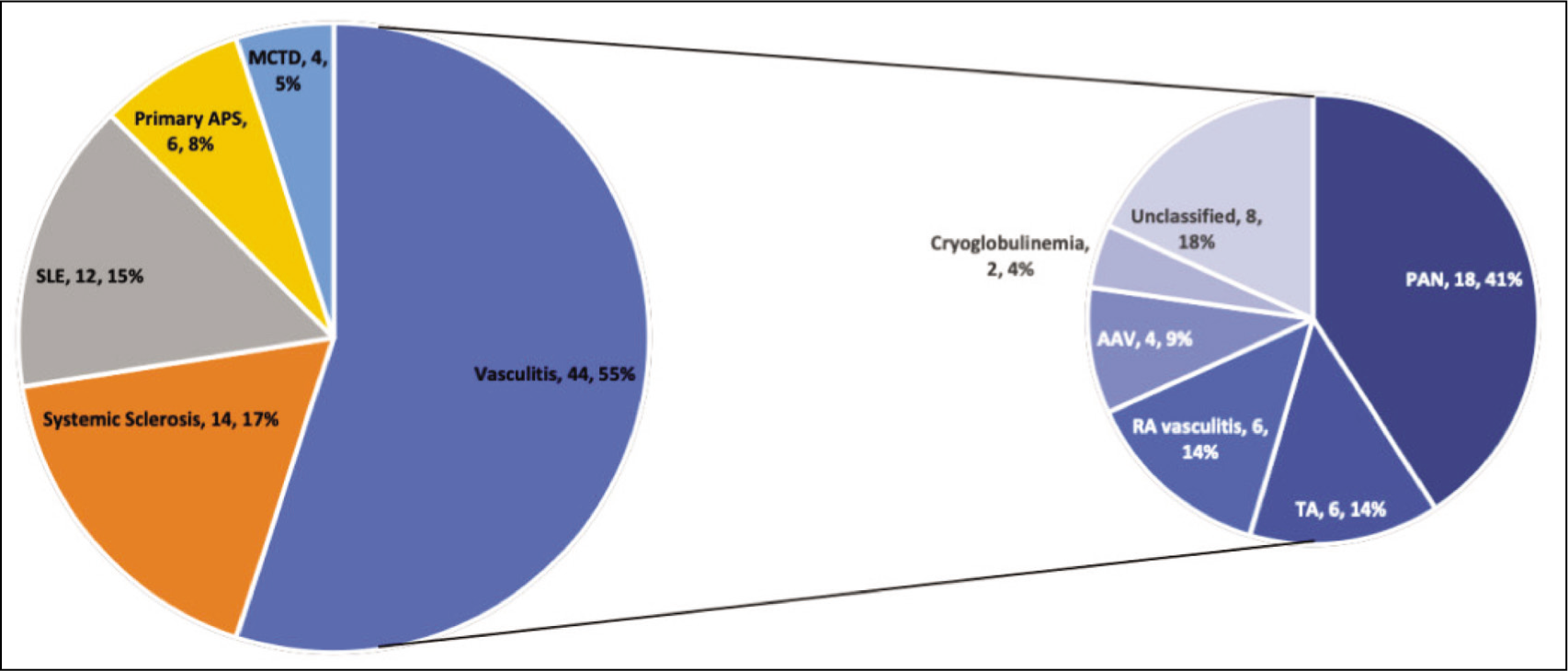
Aetiology of Ischemic Lesions Amongst Patients with Rheumatic Diseases.
Before and After Treatment Images of Peripheral Gangrene in a Man with Polyarteritis Nodosa.

Presentation and Outcomes of Those with a Rheumatic Aetiology
Early ischemic/pre-gangrenous lesions and gangrenous lesions were equally distributed in the cohort [38 (47.5%) and 42 (52.5%)]. They were the presenting manifestations of the disease in 61 (71.3%) patients. The most common rheumatic cause of peripheral ischemic lesions was vasculitis (44, 55%), followed by SSc [14, 17.5%; diffuse SSc in 11 (61.1%)], primary APS (6, 7.5%), SLE (12, 15%; 3 of 12 had associated secondary APS) and MCTD (4, 5%).
Amongst vasculitis, PAN (including cutaneous PAN) was the most common cause followed by unclassified vasculitis (Figure 1). Details about the presentation, treatment and outcomes across diseases are detailed in Table 1.
Comparative Analysis Across Various Rheumatic Diseases.
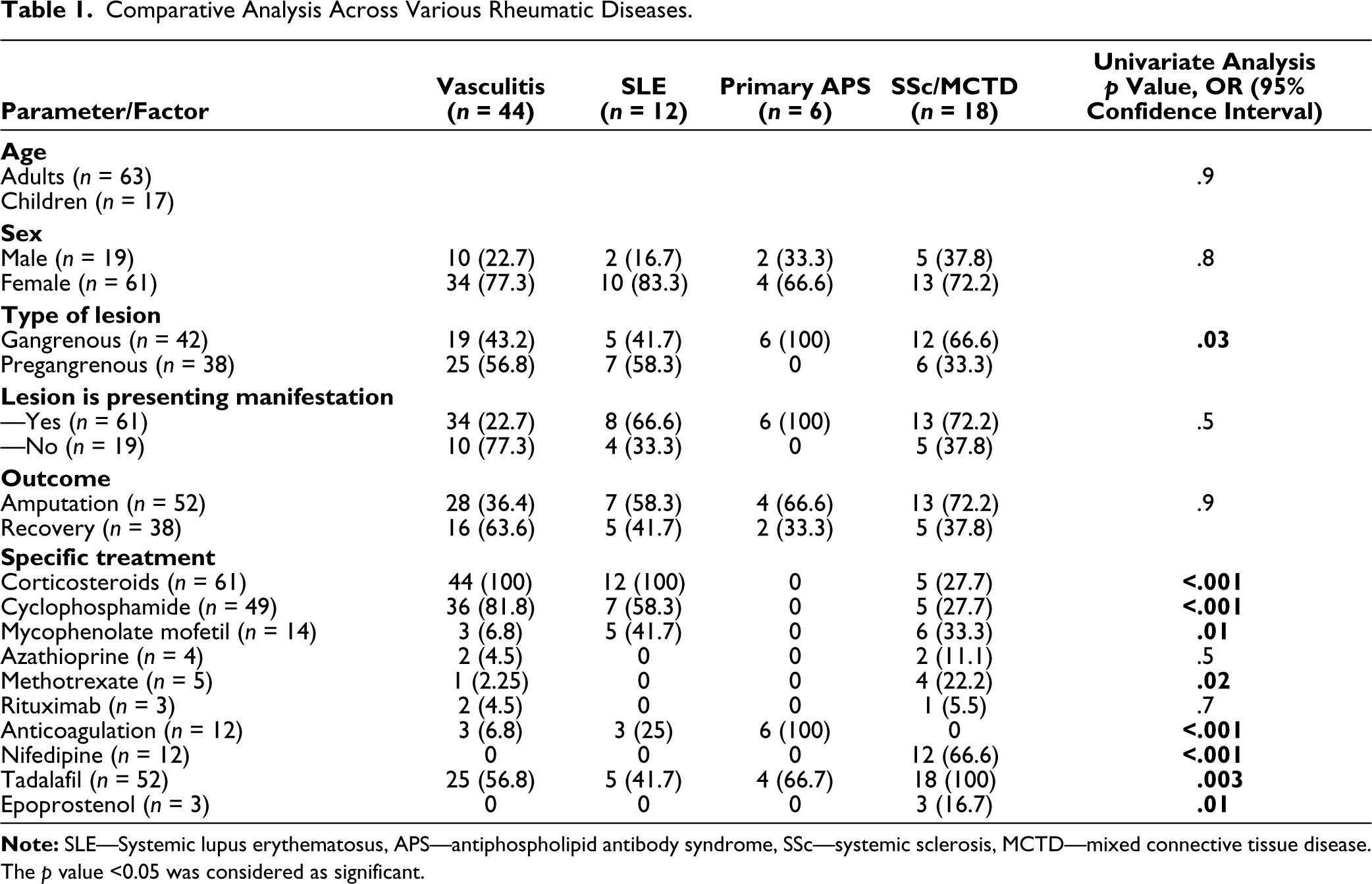
Two-thirds (52, 66.2%) of patients underwent amputation of which surgical amputation was required in 22/80 (21.5%) and the remaining had an auto-amputation. With conservative medical management, 27/80 (33.8%) patients showed a complete or nearly complete recovery.
Associations with Outcomes
The factors associated with recovery have been described in Table 2. The most important factors associated with recovery were early referral, early initiation of treatment and pregangrenous changes. Age, gender and aetiology were not associated with recovery.
Factors Associated with Outcomes in Rheumatic Peripheral Ischemic Lesions.
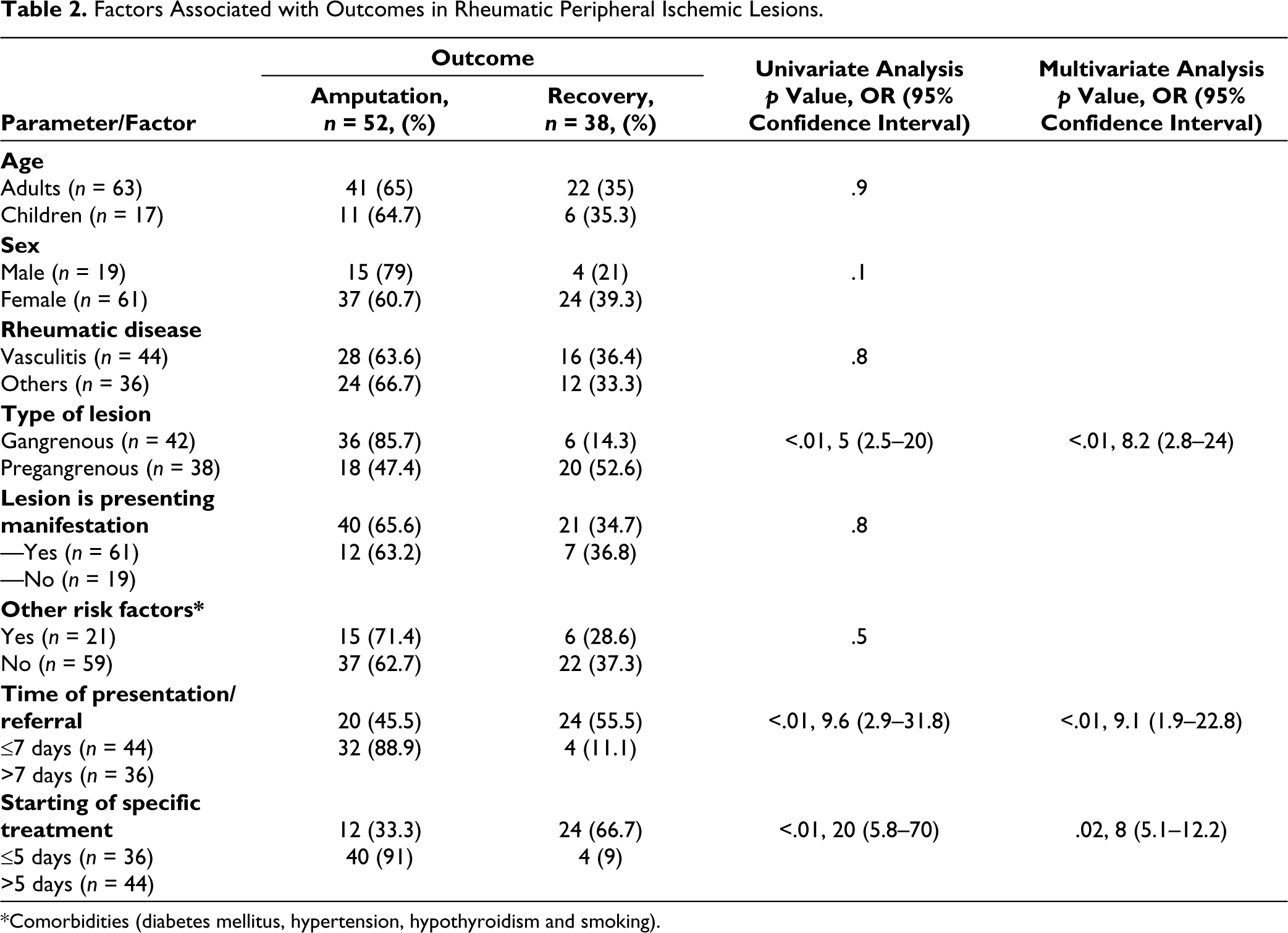
*Comorbidities (diabetes mellitus, hypertension, hypothyroidism and smoking).
On multivariate analysis, the type of ischemic lesion and time of presentation were significantly associated with recovery.
Discussion
We found that the majority of patients presenting to the rheumatology clinic with peripheral ischemia had associated systemic rheumatic diseases, the most common being the vasculitis spectrum of diseases. The underlying diseases significantly determined the severity of ischemia at presentation and the choice of therapy, however, there was no impact on the outcomes. It was the presenting manifestation in 75% of cases, and two-thirds of patients underwent either an auto- or surgical amputation. Early referral, early initiation of specific treatment, and the presence of pregangrene were associated with recovery.
Among vasculitis, PAN (classical and cutaneous PAN) was the leading cause of peripheral ischemic lesions. A French cohort of PAN reported peripheral ischemia in 43 of 348 (12%) patients whereas a Chinese study reported a much higher prevalence of 31.8% (6, 10). PAN represents a classic form of medium vessel vasculitis with digital ischemia as a presenting feature. This was observed in our cohort as well in which the majority of patients with PAN had peripheral ischemia as the presenting feature. The second most common causes were rheumatoid vasculitis and Takayasu arteritis. Although gangrene is uncommonly observed in Takayasu arteritis, it is more common in Asians and Indians resulting in it being the second most common cause in our cohort. 11
The mechanism of peripheral ischemia in SSc is related to vasculopathy and secondary obliterative thickening of vessel walls. Inflammatory infiltrates are absent, and the internal elastic lamina remains intact.18, 19 Although rare, typical vasculitis with inflammatory infiltrates damaging blood vessels has been reported in patients with SSc. 20 Thus, occasionally, vasculitis and stenosing vasculopathy may coexist. SSc being an important cause of vasculopathy was responsible for ischemic lesions in 14 (17%) patients in our study. All of these patients had a history of Raynaud’s phenomenon suggesting a vasculopathic origin of peripheral ischemia. 21
Vascular involvement is frequent in SLE patients and represents the most frequent cause of death in established diseases. 22 These lesions are commonly known as lupus vasculopathy and are one of the most typical symptoms. Vascular involvement in SLE may be due to accelerated atherosclerosis, associated anti-phospholipid antibodies, or vasculitis. A typical vasculitis with inflammatory infiltrates and vascular wall necrosis occurs less often. 23 In patients with APS, ischemic lesions are due to arterial and/or venous thrombosis. Of the 12 (15%) patients of SLE who had peripheral ischemic lesions, one-fourth of them also had secondary APS in our series. Primary APS was diagnosed in 6 (8%) patients in our series.
A female preponderance was noted in our cohort of patients which is in line with rheumatic diseases are more common in women. Also, the female preponderance was much lower in children (81% females amongst adults versus 62% amongst children). The majority presented during the winters as cold-induced vasospasm is one of the most common precipitating factors for Raynaud’s phenomenon. It also reduces the reserve for peripheral circulation in other causes of peripheral ischemia like atherosclerosis, thromboembolic and vasculitic. While peripheral ischemic lesions are usually encountered during severe disease courses with the involvement of multiple organs, these lesions may represent either initial or isolated manifestations in some patients of rheumatic disease. In two-thirds of our patients, it was the presenting manifestation of the disease.
In our study vasculitis was the leading cause (45%) of peripheral ischemic lesions/gangrene as compared to earlier published data from India by Bichile et al. 24 who reported SSc as the leading cause (35.8%), Kirthi et al. 25 who reported SLE (41%) as leading cause and Vijayan et al who found MCTD as the most common cause (7 of 22, 31.8%). This may be related to the different geographic distribution of rheumatic diseases or changing rheumatic disease patterns over time. We also found patients with primary APS and SSc/MCTD were more likely to present as gangrene compared to those with vasculitis and SLE which had an equal proportion of those presenting with gangrene and pregangrene is likely due.
The treatment was based on the specific disease aetiology with the use of corticosteroids, cyclophosphamide and mycophenolate mofetil significantly higher in the vasculitis and SLE group; anticoagulation in the APS group, and vasodilators in the SSc/MCTD group in line with the standard treatment norms.
The outcomes were dependent upon the timing and type of presentation. A late presentation with gangrene resulted in amputation in the majority of the cases. Early initiation of a cocktail of multipronged therapy targeting multiple mechanisms like anticoagulation, vasodilators and corticosteroids may be helpful in the initial stages till a definite diagnosis is made to prevent delay in the institution of correct treatment.
An accurate diagnosis of the underlying disease, suspicion of the mechanistic aetiology of the peripheral ischemia, and prompt management are very important in reducing morbidity. Early specific treatment may prevent progression and help in the recovery of lesions and salvage of digits/limbs.
The distinct strengths of our study include a broad overview of the aetiology of peripheral ischemic lesions presenting to the rheumatology clinic and factors associated with its outcomes. Our study has several limitations including a retrospective design and bias involving a tertiary care referral system translating into a greater proportion of patients with rheumatic causes. The mechanistic cause of the ischemic lesions was not evaluated in detail. A prospective longitudinal design capturing multiple episodes would be the future direction along with analysing non-rheumatic causes of gangrene commonly confused with rheumatic diseases resulting in an undue delay in the institution of therapy. A collaboration with vascular surgery and haematology departments would be an appropriate next step as well to capture the maximum number of cases.
Conclusion
Vasculitis was the most common cause of peripheral ischemia presenting to our rheumatology unit. Treatment was based on the underlying pathophysiologic mechanisms of ischemia as per the primary diagnosis, with no difference in the outcomes across the underlying primary diseases. Late referral or presentation to the hospital, delayed specific management and a higher grade of ischemia (gangrene) resulted in poorer outcomes in these patients. Early diagnosis and aggressive multidisciplinary management should be warranted for optimal outcomes in cases of peripheral ischemic lesions.
Footnotes
Author Contributions
UD was involved in the data collection. Dr UD, PM and KK contributed to the statistical analysis, manuscript drafting and corrections.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Patient Consent
Reference number for ethical approval by institutional ethics committee is mentioned on page No-2 of manuscript’s, statistical analysis section. Exemption of patient consent was taken in view of retrospective design of study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.