
Abstract
Aim:
The present study aimed to evaluate the factors influencing the referral delay in patients with primary Sjogren’s syndrome (Sjogren’s) and systemic sclerosis (SSc).
Materials and Methods:
The independent, multicentre, cross-sectional study collected data from seven centres across India through the Indian Rheumatology Association (IRA) database. The patient-related factors and referral factors were determined based on the patient narrations. Based on the patient’s income, a modified version of the Prasad scale was employed to classify them according to socioeconomic status.
Results:
The study included 118 patients with Sjogren’s and 166 patients with SSc. Approximately 60% of patients with SSc and Sjogren’s received rheumatology specialty care more than 6 months after symptom onset. The primary reasons for this delay were identified as a lack of awareness of rheumatology specialty care among patients (Sjogren’s: 61%; SSc: 74%) and disease management by other specialists (Sjogren’s: 75%; SSc: 62%) rather than rheumatologists. Additionally, over 25% of primary care practitioners were unaware of rheumatology specialty services, and a similar percentage of patients were not diagnosed with rheumatic diseases by their primary care physicians. Patients with delayed referrals for Sjogren’s exhibited higher rates of haematologic, oral, and non-articular pain. Similarly, in SSc patients, delayed referral was associated with a significantly higher prevalence of skin involvement (P < .01).
Conclusion:
Patient referrals to other specialties and a lack of knowledge about rheumatology were the primary causes of referral delays. Educating primary care physicians and facilitating direct referrals to rheumatology specialists could help reduce these delays. The study findings may help in stratifying interventions to improve early referral and access to rheumatology specialty care for patients with Sjogren’s and SSc.
Keywords
Introduction
Diseases such as scleroderma (SSc) and primary Sjogren’s syndrome (Sjogren’s) have demonstrated better treatment outcomes under the specialty care of trained rheumatologists and immunologists. The availability of rheumatologists, and the awareness and attitude of both patients and primary care physicians are the key factors influencing the early referral and utilisation of rheumatology specialty care. 1
The delay in referral and management of patients with autoimmune rheumatic diseases (AIRDS) can cause significant mortality and morbidity, as the undiagnosed disease may lead to prolonged disease activity and associated sequelae. For Sjogren’s, there may be a window of opportunity where patients would benefit from immunosuppression, and this window of opportunity is lost when the diagnosis is delayed. 2 It is often challenging to establish a definitive cut-off period for diagnosing and referring patients. Some studies have investigated the delay from the first attributable symptom to diagnosis as the cut-off, while others have suggested the time required to access specialty care. In certain cases, patients with timely diagnoses might not have received the appropriate specialty care.
Studies have reported different time frames for delay in referral and diagnosis, ranging from weeks to months. According to the literature, the mean delay or time taken for patients with arthritis and systemic inflammatory diseases ranges from 3 to 12 months. A Europe-based study reported that the median delay across 10 centres from symptom onset to assessment by rheumatologists was 24 weeks. 3 Similarly, another UK-based study on the experiences of patients with lupus and related systemic autoimmune diseases reported 6 years and 11 months as the mean time to diagnosis from first experiencing symptoms. 4 Additionally, a study conducted in Pakistan reported the median time for patient-related delay in reaching a rheumatologist as 6 months. 5 Furthermore, a German-based study by Funch et al. reported 30 weeks as the median time from symptom onset to rheumatologist appointment. 6 A Canadian-based study reported that patients were seen by rheumatologists within 1 year of referral. 7 The National Health Service (NHS) submitted its recommendations to improve the referral time to treatment and reference to rheumatology to <2 months (8 weeks). 8 Based on these observations and the recommendation of 2 months, the current study proposes 6 months as a probable cut-off.
The number of trained specialists in the field of rheumatology required to cater to the population in India has improved in recent years. 9 However, such measures remain insufficient in ensuring optimal care. Factors influencing patient access to specialty care extend beyond mere availability and accessibility. These factors can be categorised into three main groups: (1) patient-related factors such as beliefs, self-care practices, education level, socioeconomic status, demographic characteristics, disease knowledge, and financial resources; (2) factors related to primary care or referring physicians including their knowledge regarding specialty services and accurate diagnosis; and (3) disease-specific factors such as clinical presentations. The study aims to evaluate the factors influencing referral delays in patients with SSc and Sjogren’s to the rheumatology specialty. The findings may assist in stratifying interventions to improve early diagnosis and enhance access to specialised care.
Material and Methods
Registry/Database Design and Study Population
The independent multicentre, database-based, cross-sectional study gathered data from seven centres across India (five private and two academic) using the database created by the Indian Rheumatology Association (IRA). The selection of centres was based on geographic location (Supplementary Figure 1), patient load, and data availability. The database focused on patients diagnosed with six autoimmune diseases namely psoriatic arthritis, rheumatoid arthritis, SpA, SLE, SSc, and Sjogren’s. The present study considered data of adult patients fulfilling American College of Rheumatology (ACR) criteria for Sjogren’s and SSc.10,11
The database, launched in April 2020, encompassed both newly diagnosed individuals and those undergoing follow-up at the centres. Data collection was carried out using two distinct, predefined structured proformas specific to each disease. The first proforma gathered information on common demographic and socioeconomic profiles, functional impairment, obstetrics, and health-related parameters, while the second proforma was used for collecting disease-specific details. The data collection protocol and training modules were prepared by experts in rheumatology, consisting of four principal investigators (PI). The proforma and modules underwent thorough trials and verifications. After ensuring accuracy and effectiveness, the proforma was finalised before the final data collection. Clinical research associates (CRAs) completed the answers based on patient responses. To ensure consistency across all centres, both PIs and CRAs underwent online training facilitated by the nodal centre. The PI at the nodal centre addressed any inquiries related to data collection.
Each of the participating centres secured approval from their respective institutional ethical committees (refer to the enclosed list in the appendix). Informed consent was also obtained from all enrolled patients, following the guidelines of their respective institutions.
Sample Size Calculation for Registry
The minimum number of participants needed for recruitment was determined with the primary goal of evaluating the clinical and laboratory profiles of all AIRDs under consideration. The estimated sample size for analysis was 6500 patients. Given its cross-sectional design and focus on patients seeking rheumatology care, the estimated prevalence of all AIRDs among individuals with musculoskeletal symptoms was approximately 10%. 12 The calculated P value was .01, corresponding to a Z-score of 2.59 for a 99% confidence interval, with an estimated precision (d) of 0.01. Based on these calculations, a population size of 6,037 was initially determined, with a buffer added to account for potential dropouts and missing data, resulting in a final estimated sample size of 6500 participants. 13 Patients with inconsistent or incomplete data were not considered for the analysis. The sample size for each disease was estimated based on the proportional prevalence of each autoimmune disease. Patients with Sjogren’s and systemic SSc were included in the sub-study, and the sample adequacy was calculated using post-hoc power analysis as described in the statistics section.
Data Collection and Definitions
In order to investigate the factors responsible for delayed access, the study considered the time taken to access rheumatology care from the onset of the first attributable symptom or sign related to the primary diagnosis. If a patient had visited another rheumatology centre prior to their visits to the participating centre, their prior visit was considered, although there were very few such patients. Based on previous literature evidence, a delay of 6 months was taken as the cut-off for referral delay or access to tertiary care. The patient’s first encounter with specialty care was considered instead of the diagnostic conclusion prior to referral or in the rheumatology department. Consecutive patients who consented were included in the study, encompassing those who reported new symptoms to the participating centre during the study period and those who were in follow-up and reported symptoms during the study period either as part of a routine visit or an emergency.
Each patient underwent interviews and assessments by the research team to investigate the factors contributing to the delay in referral. Patient-related factors considered included their belief in modern medical care, lack of awareness regarding rheumatology as a specialty, socioeconomic status (such as affordability of treatment and considerable distance to specialty centres), and concerns about potential adverse events associated with modern medical care. Key referral factors, as narrated by the patients, are outlined below: primary care providers either did not refer to a rheumatologist or were hesitant to do so; despite receiving a correct diagnosis, patients were referred to other specialties such as nephrology, dermatology, or orthopaedics; primary care physicians were unaware of rheumatology as a specialty; and patients were either unaware of their primary diagnosis or lacked documentation confirming it. If the researcher could not determine the reason despite considering all these factors, it was recorded as unascertainable.
The assessment of the knowledge of the primary care physician was concluded based on two criteria, with which the data collector was trained. First, if the diagnosis was confirmed in the prescription and the patient was managed solely by the primary care provider without consultation with a rheumatologist or specialist. Second, if the patient was recommended to see a rheumatologist but had not done so. Any failure to provide a proper diagnosis and appropriate management was considered a failure to recognise the disease. On the other hand, if the diagnosis was mentioned appropriately but the patient was not referred to rheumatology for further evaluation, it was considered reluctance to refer.
The Modified Prasad scale, incorporating patients’ income, educational status, and profession, was utilised for socioeconomic classification. 14 Clinical presentation and systemic involvement were also taken into account for the analysis.
Statistical Analysis
Descriptive statistics were conducted using Microsoft Excel. Data from patients with Sjogren’s and SSc were analysed separately. Continuous variables were compared using t-tests, while categorical variables were assessed using the chi-square test or Fisher’s Exact test. Missing data, especially those without identifiable reasons, were excluded from the analysis under the assumption that they were unrelated to the variables of interest.
Subjects in each disease group were divided into those referred to rheumatology specialty within 6 months and those referred after more than 6 months. Statistical analyses were performed using the Statistical Package for the Social Sciences (SPSS, IBM, version 29.0.0). Additionally, a post-hoc power analysis was performed using SPSS to evaluate the statistical power of the study’s subjects. Separate one-sample proportion analyses were conducted for SSc and Sjogren’s. 15 For SSc, the sample size was 166, assuming a default proportion (P) of .5. For Sjogren’s, the sample size was 118, with a specified P value of .05 and a default null proportion of .5.
Results
The number of study subjects considered in the respective disease groups was 118 out of 124 for Sjogren’s and 166 out of 183 for SSc. Due to inconsistent data on the delay, 17 patients in the SSc group and six patients in the Sjogren’s group were excluded from the analysis. The post-hoc power analysis for sample adequacy yielded 84% for Sjogren’s and 94% for SSc. The demographic characteristics of the population and the mean referral delay observed for the disease groups are listed in Table 1. SSc patients were referred to specialty care 10.63 ± 24.67 (1–156) 10 months after the onset of the first attributable symptom, whereas the mean delay in referral was 5.91 ± 44.47 (1–288) 6 months for Sjogren’s.
Demographic Distribution of Sjogren’s and SSc Patients and Comparison of the Causes for Delay.
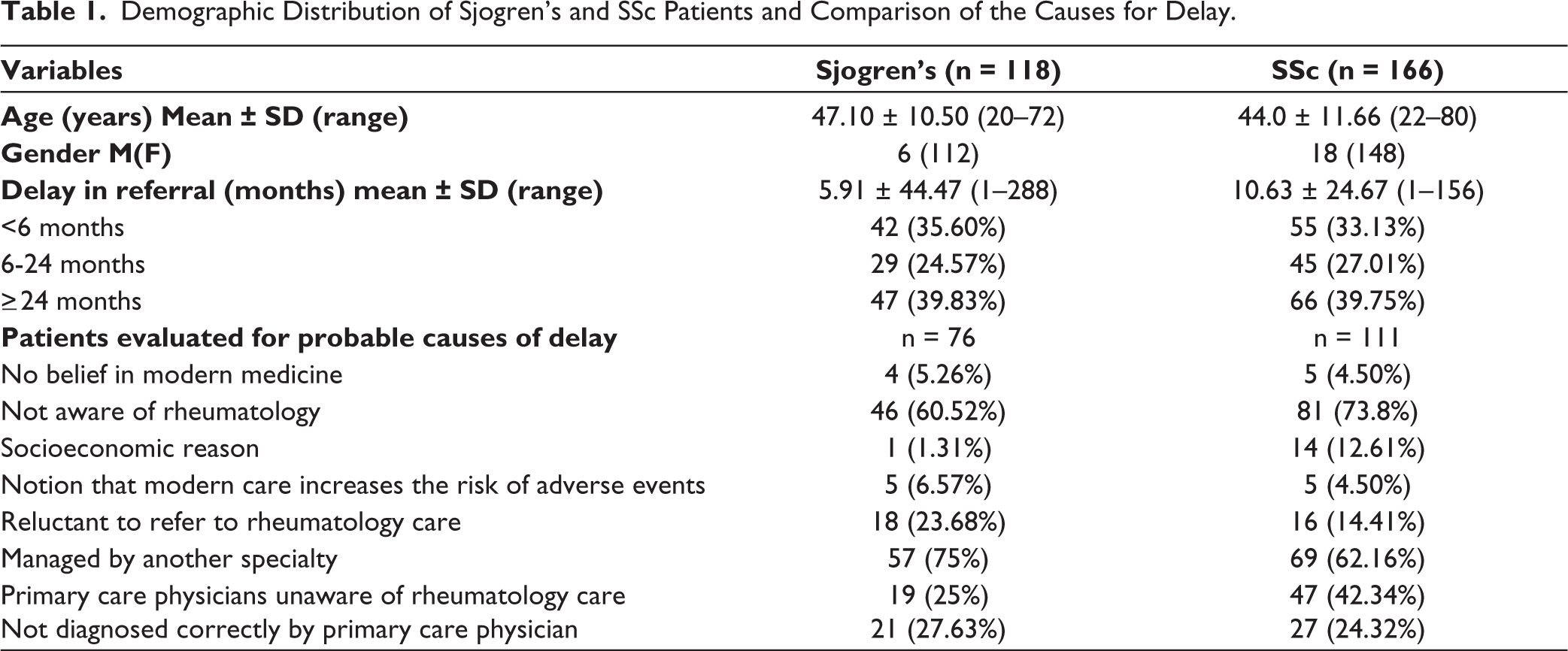
Both patient groups were categorised based on the timing of referral to the rheumatology specialty, either within 6 months or later. In patients with Sjogren’s, those referred within 6 months had a median delay in referral of 2 months (range: 1 –5 months), whereas those referred later had a median delay of 24 months (range: 6–288 months). Similarly, for patients with SSc, those referred within 6 months experienced a median delay of 2 months (range: 1–3 months), compared to 24 months (range: 6–156 months) for those referred later.
More than 60% of the patients with SSc and Sjogren’s had availed rheumatology specialty care after 6 months of disease onset. Nearly 5% of the patients across the disease groups had no faith in modern care due to the notion of elevated risk for adverse effects. Lack of awareness of rheumatology specialty care among patients (Sjogren’s: 61%; SSc: 74%) and disease management by other specialists (Sjogren’s:75%; SSc: 62%), instead of rheumatologists, were identified as the primary causes for delay in utilising the rheumatology specialty. Around 25% of primary care physicians managing patients with Sjogren’s were concluded to be unaware of rheumatology care, while 27.63% of Sjogren’s patients were not correctly diagnosed. Similarly, in the SSc cohort, 42.34% highlighted a lack of awareness among primary care physicians regarding rheumatology care, and 24.32% were not diagnosed by primary care providers (Table 1).
A statistically significant difference in the clinical characteristics was observed for Sjogren’s patients referred within and after 6 months, for haematologic (P = .004), oral (P = .056), and other clinical features (P = .049, musculoskeletal pain other than joint pain). Whereas, in SSc patients, skin involvement was higher among those referred late to rheumatology, after 6 months. No significant differences were identified in the socioeconomic status, profession, or education of Sjogren’s patients seeking rheumatology specialty care. Whereas, a direct association was found between monthly income and access to specialty care for SSc patients (details provided in the supplementary file).
Discussion
The patients suffering from Sjogren’s reached rheumatology slightly earlier than those with SSc. Forty percent of patients with SSc and Sjogren’s received rheumatology care later than 2 years. The delay in referral in AIRDS has been reported by several national and international studies, but the reasons are often zone-specific.16-18 Delayed referral noted in Sjogren’s and SSc could be attributed to the fact that these diseases are less frequent and tend to progress gradually. Primary reasons for delayed referral included a lack of awareness about rheumatology care and limited disease knowledge. Socioeconomic factors did not significantly influence access to rheumatology care.
There were no significant differences in the clinical features between patients referred late and those referred early, except for higher rates of skin involvement observed in patients with SSc who were referred late. This could be attributed to the likelihood that patients with only skin involvement were managed by dermatologists. Similarly, patients exhibiting systemic features such as haematology and non-joint symptoms experienced delayed referral, or these features were already present by the time of rheumatology referral.
Diagnostic delay remains largely unexplored in Sjogren’s. The self-reported diagnostic delay noted in a nationwide survey conducted by Segal et al. in 277 Sjogren’s patients was an average of 7.1–9.4 years. 19 A Ukranian study reported a substantial time gap between the onset of symptoms and diagnosis of Sjogren’s, especially in patients with ocular/oral dryness. 20 An exploratory cross-sectional study conducted in Saudi Arabia has reported approximately 2 years as the mean diagnostic delay noted in Sjogren’s patients. The study has highlighted the need to implement measures facilitating early diagnoses in specialties receiving suspected diagnoses of Sjogren’s patients such as ophthalmology, dentistry, neurology, pulmonology, and family medicine. 21
Sandhya et al. reported that diagnosis of Sjogren’s, even in referral centres, is often challenging due to the presentation of patients with myriad features to different specialties. The study found that patients consulted 24 different types of specialists during their initial visits, and many of them visited multiple hospitals before receiving a final diagnosis of primary SS. However, in 64.84% of cases, it was a rheumatologist who first suspected the disease. They concluded that a high index of suspicion along with anti-SSA (anti-Ro) antibody testing may help in enhancing the diagnosis. 22 However, in the present cohort, clinical features were not significantly different between the patients with early or late diagnosis, suggesting the delay was more due to lack of knowledge about the specialty and disease.
In the present study, more than 60% of patients with SSc and Sjogren’s were referred to specialty care only after 6 months. Omair et al. reported that early referral to the specialised clinic for SSc and rapid access to minor salivary gland biopsy within 2 weeks helped in reducing the delay in diagnosis (not <2 years). 21 In the present study, SSc patients with skin involvement reported a delayed referral to the specialty centre. Pauling et al. reported that diagnostic delay in primary care could be attributed to the significant lag between the coding of Raynaud’s phenomenon and systemic sclerosis (SSc). 23 A German-based trial reported a significant reduction in diagnostic delay for inflammatory rheumatologic diseases with the use of criteria like positive rheumatoid factor or anti-CCP elevated inflammatory parameters and musculoskeletal symptoms along with the implementation of open-access rheumatology care. 24
The current study found that over 50% of patients were directed to other specialties, while 5%–8% of the patients were sceptical regarding modern medical care. Addressing the misconception that modern medicine carries higher risks and educating patients about medical care can help overcome these obstacles through counselling and education. Overall, no significant impact was noted for socioeconomic status on the delay in referral to specialty care, especially for Sjogren’s and SSc. The accessibility to rheumatology specialty care was not significantly affected by the affordability, as data was collected from both public fund-supported institutions and the private sector.
In both Sjogren’s and SSc groups, a notable proportion of patients faced challenges related to primary care, emphasising potential areas for improvement. Among Sjogren’s patients, 25% reported primary care physicians being unaware of rheumatology care, while 27.63% were not correctly diagnosed. Similarly, in the SSc cohort, 42.34% highlighted a lack of awareness among primary care physicians regarding rheumatology care, and 24.32% reported misdiagnosis by primary care providers. The difference in these proportions regarding awareness of rheumatology between the two diseases does not indicate a lack of awareness of the rheumatology specialty among primary care providers. Instead, it reflects their perception that SSc is managed by dermatologists. These findings highlight the importance of increasing rheumatological awareness and promoting timely referrals at the primary care level to facilitate optimal and accurate management of AIRDS.
The major strengths of the present study include multicenter data collection, a larger sample size, and involvement of both academic (public) and private settings, which allowed for the representation of individuals belonging to different socioeconomic status. However, limitations of the study include non-uniformity in the number of patients recruited from different centres and the study cohort not being representative of the geographic population, which restricts the generalisation of the study findings. The post-hoc analysis suggests adequate power for proportion studies. The potential bias due to researchers’ discretion in gathering reasons for the delay in referral through the recall method cannot be excluded. Providing sufficient training on data collection could have minimised this bias.
Conclusion
In developing countries such as India, delays in seeking rheumatology care adversely impact the prognosis and increase the disease burden of autoimmune rheumatic diseases like Sjogren’s and SSc. It is important to increase awareness regarding specialty care and disease among primary care physicians and patients to facilitate early referral and treatment, thereby achieving the best possible outcomes.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The methodology section may have similarities to our previous publication titled ‘Chandrashekara S, Shenoy P, Kumar U, et al. Delay in Referral to Specialty Care in Patients with Spondyloarthropathy and Psoriatic Arthritis in India: IRA Database Report. Indian Journal of Rheumatology. 2024;19(1):41-46,’ as the data collection and procedures were similar. Dr. Debashish Dhanda and Dr. Aman Sharma for their participation in administrative role in IRA database. The authors acknowledge the help of Research Assist (
Author contributions
All the authors have contributed equally to the conceptualization, data capturing and developing the content.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Each of the participating centres secured approval from their respective institutional ethical committees.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Educational and research grants from Novartis India.
Patient Consent
Informed consent was obtained from all enrolled patients, following the guidelines of their respective institutions.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.