
Abstract
Introduction
Preterm birth complication is the first leading cause of neonatal mortality in Ethiopia. In this study, the pooled prevalence and predictors of preterm mortality in Ethiopia were assessed.
Methods
The research protocol was registered to PROSPERO under the CRD42023415334 registration number. PubMed, Google Scholar, Cochrane Library, and Hinari databases were searched for studies up to April 10, 2023. Cohort studies on the incidence of preterm mortality and its predictors in Ethiopia were included in this review. This review was reported using the preferred reporting items for systematic reviews and meta-analyses checklist. We extracted data from the selected papers and exported to R 4.2.3 and STATA version 15.0 for estimating pooled incidence proportion, density rate, and adjusted hazard ratio (AHR). By looking at the funnel plot and using Egger’s test, the publication bias was assessed. This study didn’t receive funds from any organization.
Results
From 152 identified studies, 16 studies were selected for final analysis. The pooled incidence proportion and incidence density of preterm mortality were 30% (95% CI: 27%–32%) and 40 (95% CI: 30–40) per 1,000-person days, respectively. Being a male (AHR = 1.43, 95% CI: 1.09, 1.78), gestational age (0.83, 95% CI: 0.80, 0.87), born before 32 weeks (AHR = 2.15, 95% CI: 1.15, 3.84), antepartum hemorrhage (AHR = 2.46, 95% CI: 1.07, 3.84), the fifth minute Apgar rating less than seven (AHR = 1.84, 95% CI: 1.43, 2.25), birth asphyxia (AHR = 1.87, 95% CI; 1.59, 2.14), birth weight 1,000–1,499 g (AHR = 3.63, 95% CI: 1.69, 5.57), respiratory distress syndrome (AHR = 1.80, 95% CI: 1.59, 2.02), jaundice (AHR = 2.39, 95% CI: 1.16, 3.61), neonatal sepsis (AHR = 1.54, 95% CI: 1.25, 1.83), and not using kangaroo mother care (AHR =1.92, 95% CI: 1.11, 2.72) were predictors of time to death of preterm.
Conclusions
Almost one third of preterm neonates treated at different health facilities in Ethiopia failed to survive to the first four weeks of life. Because every study that was included was an institution-based cohort study, the results may not generalized to preterm newborns who were not hospitalized at medical facilities.
Introduction
Preterm birth is the term used to describe babies born before the full 37 weeks of pregnancy. 1 It may happen due to spontaneous preterm labor or due to a medical indication such as antepartum hemorrhage, hormonal changes, bacterial infection, and others. 2 In 2020, over 13.4 million newborns were preterm worldwide. 1 In Ethiopia, the pooled prevalence of preterm birth was 11.4% in 2021. 3 It remains the main contributor to newborn death globally. 4 In Sub-Saharan Africa and Asia, the risk of infant mortality related to preterm birth is at least 12 times higher compared to Europe.5, 6
Different organizations are working toward the achievement of the sustainable development goal of reducing the neonatal mortality rate to 12 per 1,000 live births by 2030. 7 However, globally 2.4 million neonates (6,700 each day) died in 2020, where preterm birth complication is the first leading cause of it. 8 Of the 10 countries with the highest newborn death rates worldwide, Ethiopia ranked fourth. 8 Ethiopia’s health sector transformation plan II agenda has set a goal of lowering the neonatal mortality rate to 21 per 1,000 live births by 2025 9 ; however, it remained high. 10 In Ethiopia, preterm birth complications and other preventable causes account for greater than 80% of the cause of neonatal death. 11 The World Health Organization suggested that about 75% of neonatal deaths due to preterm birth complications are preventable with the current treatments. 1 In addition, the Ethiopian government also demonstrated its efforts to increase neonate survival, particularly for preterm births, by including high-impact life-saving neonatal interventions. 12
Generally, reports from studies done on preterm neonates treated at different health facilities in Ethiopia showed inconsistent preterm survival rates and its predictors.13–15, 22–28 Therefore, this study aimed to assess the pooled incidence of preterm mortality and its predictors among preterm neonates treated at different levels of health facilities in Ethiopia.
Methods
As per the guidelines provided by preferred reporting items for systematic reviews and meta-analyses, this systematic review and meta-analysis were carried out. The researchprotocol was registered to PROSPERO under the CRD42023415334 registration number.
Search Strategy and Eligibility Criteria
We thoroughly searched the PubMed, Google Scholar, Cochrane Library, and Hinari databases for primary cohort studies that evaluated the incidence and predictors of preterm death in Ethiopia, without regard to the publications’ dates, which remained accessible until April 10, 2023. A combination of medical subject heading (MeSH) terms and free-text terms such as “incidence,” “Predictors,” “Ethiopia,” “preterm,” “Survival,” “Time to death,” and “premature birth” were used to search relevant studies from the indicated databases. The articles were been identified using the search terms; (“Survival status”[Title/Abstract] OR “Survival outcome”[Title/Abstract] OR “Survival”[Title/Abstract] OR “Incidence”[Title/Abstract] OR “Time to death”[Title/Abstract]) AND (“preterm”[Title/Abstract] OR “Premature Birth”[MeSH Terms]) AND (“predictor*”[Title/Abstract] OR “determinant*”[Title/Abstract]) AND “Ethiopia”[Title/Abstract]. Furthermore, the reference lists of the found papers were examined to determine whether any studies had been overlooked. Next, all identified studies were checked for duplicates, and when identified removed. Two authors separately screened the titles and abstracts of the identified papers after. Any disagreements were resolved by discussion with a third author. After the shortlisted abstracts’ full-text papers were obtained, inclusion and exclusion criteria were used to carefully evaluate the suitability of the full-text articles for the review. The inclusion criteria for the full-text articles were as follows:
Primary cohort studies conducted among preterm neonates in Ethiopia,
Studies that have estimated the incidence proportion and density rate of preterm mortality, and adjusted hazard ratio (AHR) for predictors of preterm mortality in a table,
Research that provided the information required to derive the numerator and denominator of pertinent metrics, such as pooled AHR, incidence density rate, and incidence proportion,
Full-text studies accessible in English.
Moreover, reviews, meta-analyses, abstracts, conference papers, and letters were excluded.
Extraction of Data and Evaluation of Study Quality
Using a data extraction form pre-prepared in Microsoft Excel, two authors extracted the data required for the final review from the selected studies. The first author’s name, the year of publication, the study design, study setting, study area, name and level of the health facility, follow-up period, sample size, total death, total time at risk, predictors of mortality with its comparison group, AHR, and 95% CI of the AHR were the essential details that were taken out of the selected studies. The Newcastle–Ottawa Scale (NOS) for cohort studies was used to evaluate the quality of the eligible studies based on the selection, comparability, and outcome criteria. 29 A low risk of bias was considered having NOS score of 7 or higher. We requested the corresponding author to supply the required data which was not included with the original papers. In addition, in some studies, when the proportion of the outcome variable alone was reported, the numerator was estimated from the reported proportion and the final sample size (those who participated in the study).
Outcomes
Incidence proportion and incidence density rate were considered primary outcome measures. In addition, the predictor of preterm neonatal mortality was the secondary outcome measure.
Statistical Analysis
General characteristics of individual studies and the risk of bias were presented in the table and figure. The meta-analysis of the selected articles was performed using R version 4.2.3 and STATA software version 15.0. Meta R package was used for estimating the incidence proportion (using metaprop) and incidence density rate (using metarate). In addition, the Meta R package was used to plot the forest plot and funnel plot 30 ; the STATA version 15.0 Metan package was used to estimate the pooled AHR.
The pooled estimates of incidence proportion, incidence density rate, and AHR of predictors along with its 95% confidence intervals were estimated. The total number of preterm deaths by the total person-time at risk was used to calculate the incidence rate, and the incidence proportion was calculated by dividing the total number of preterm neonates that died at discharge from the total number of preterm neonates admitted. Using the random effects model, the incidence proportion, rates, and pooled AHR were computed. To evaluate heterogeneity, the I2 statistic and Cochrane’s Q statistical test of heterogeneity were used. The funnel plot was inspected to visually assess the publication bias, and Egger’s test was used to quantitatively assess it. Using the STATA metaninf function, the impact of each study on the total meta-analysis was determined by taking each one out separately during the sensitivity analysis.
Results
Study Selection
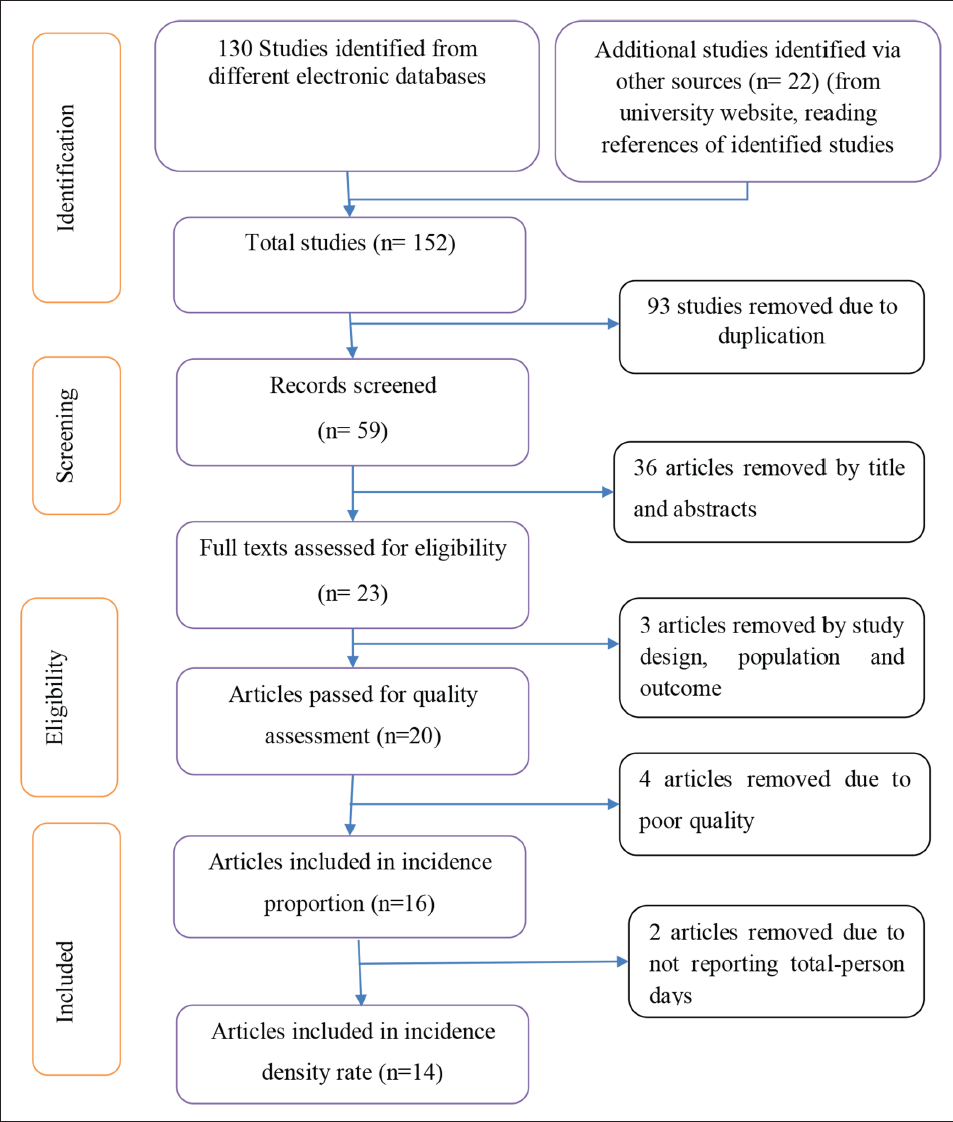
A total of 152 studies were identified from different databases and searching of gray literature. We removed 93 papers due to duplicates; therefore, 23 articles with complete texts were obtained out of the 59 that were screened for titles and abstracts. Three studies were eliminated following a full-text evaluation due to variations in study design, population, and outcomes. Therefore, 20 studies were evaluated eligible to be evaluated using the NOS criteria. Ultimately, this systematic review and meta-analysis comprised 16 studies. Out of these 16 studies, 2 studies did not report total person-time at risk, so only 14 studies were used for estimating pooled incidence density rate (Figure 1).
PRISMA Flow Chart for the Research Identified, Screened, and Included.
Quality Assessment
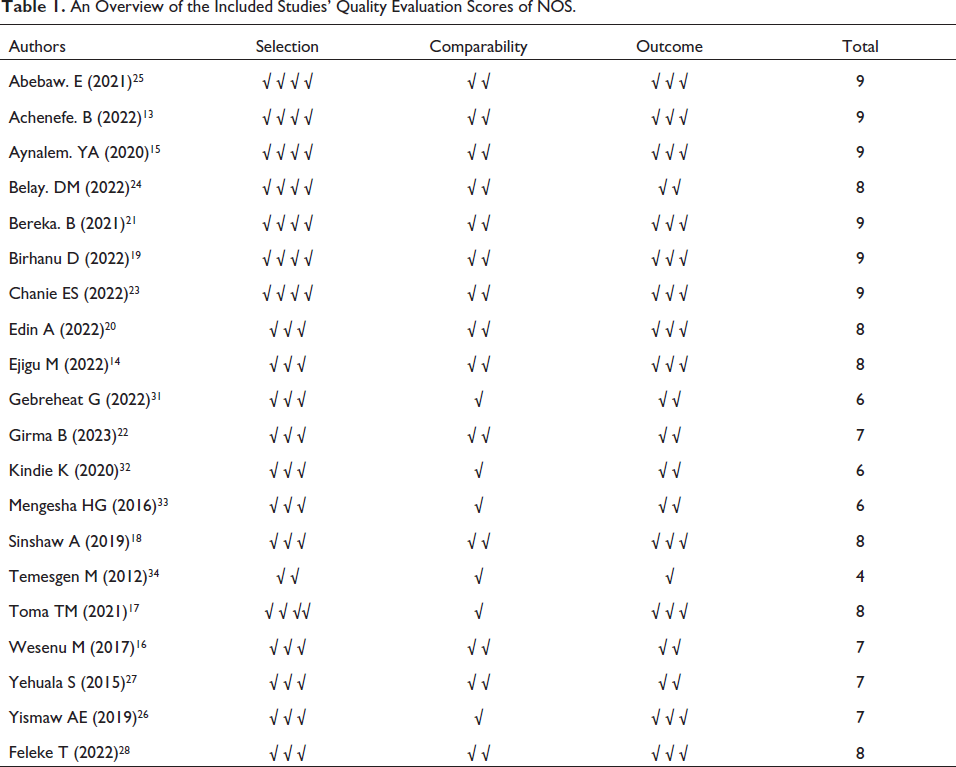
Four studies have a high risk of bias with a quality score <7, whereas 16 studies have a low risk of bias with a quality score of 7 and above (Table 1).
An Overview of the Included Studies’ Quality Evaluation Scores of NOS.
Study Characteristics
As described in Table 2, all the selected studies were published between 2015 and 2023. Eight studies were conducted in Amhara,13, 14, 18, 23–27 three studies were in the Oromia,16, 17, 20 and two studies were in Southern nations nationalities and peoples region,21, 28 In Addis Ababa, there were two studies,15, 19 and one study was in Tigray region 22 of Ethiopia. However, in terms of study design, two studies were prospective cohorts, while 14 studies13, 14, 16–24, 26, 27 were retrospective cohorts.
General Attributes of the Research that Were Used in the Final Analysis.
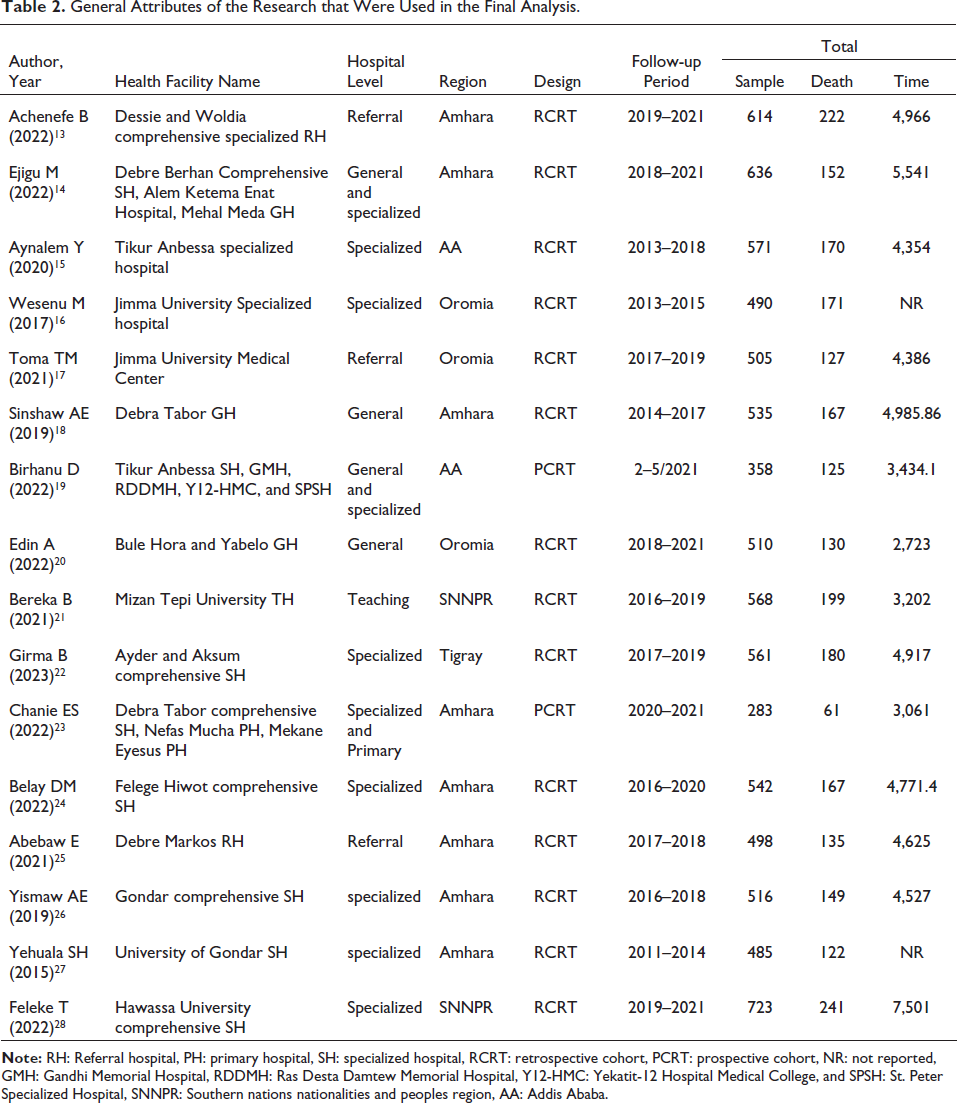
However, in terms of study design, two studies were prospective cohorts,19, 23 while 14 studies.13–18, 20, 21, 24–28 The selected studies had sample sizes ranging from 283 to 723 preterm neonates, with 8,395 preterm neonates participating in total. The total number of neonatal deaths in this study was 2,518 preterm neonates. The total person-time under observation ranged from 3,061 to 7,501 person-days at risk. Ten of the selected studies were published in different journals,15, 16, 19, 21–27 three studies were masters science thesis,13, 14, 20 and three studies were preprint17, 18, 28 (Table 2).
Synthesis of Results
Incidence Proportion
Sixteen studies reported an incidence proportion of preterm neonatal mortality. The finding from this study indicated that from the total 8,395 followed preterm neonates, 2,518 neonates died. The pooled incidence proportion of preterm death in this study was 30% (95% CI: 27%–32%) (Figure 2). With an I2 of 80% and a p value <.01, the studies showed substantial heterogeneity.
Forest Plot Describing Pooled Incidence Proportion of Preterm Mortality in Ethiopia.
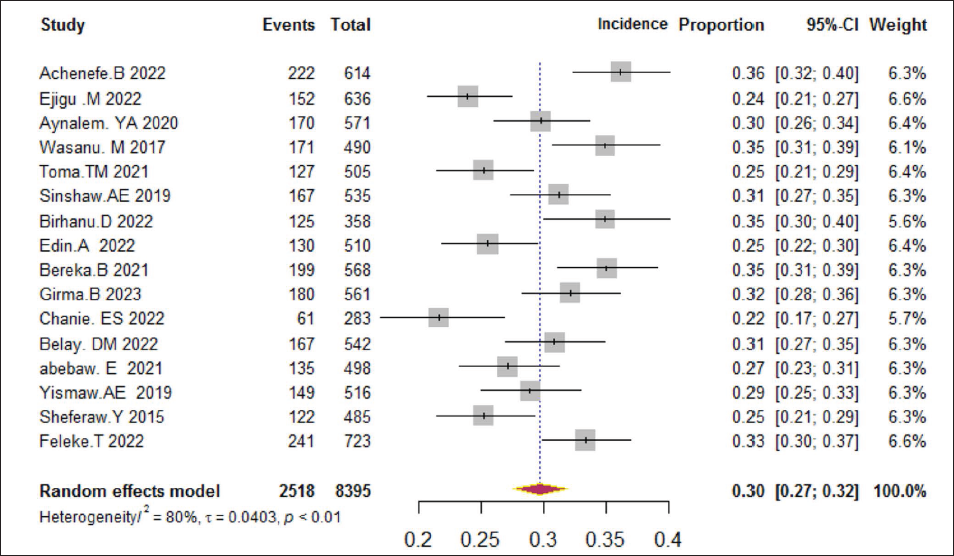
There was significant heterogeneity between the studies with an I2 of 80% and a p value <.01. To identify the possible causes of this high heterogeneity, we conducted a subgroup analysis using regions and levels of the hospital, but there was no discernible variation in the occurrence of proportion of preterm mortality. Therefore, there was no identified evidence in this study about the possible cause of heterogeneity among the study. So, we conducted meta-regression to identify significant determinants of preterm neonates’ survival.
Incidence Density Rate
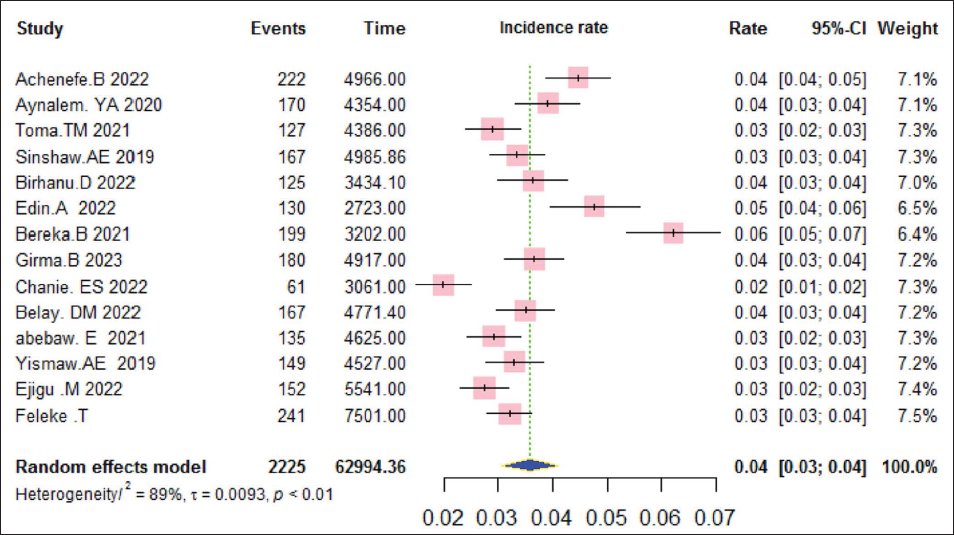
Fourteen studies reported a total number of neonatal deaths and person-time at risk, which enabled us to estimate the incidence density rate. In this study, during a total of 62,994.5 person-days at risk, 2,225 preterm neonates died, yielding a pooled incidence density rate of 40 (95% CI: 30–40) per 1,000-person days. The studies exhibited significant heterogeneity, as shown by an I2 of 89% and a p value of <.01 (Figure 3).
Forest Plot Revealing Pooled Incidence Density Rate.
Preterm Mortality Predictors
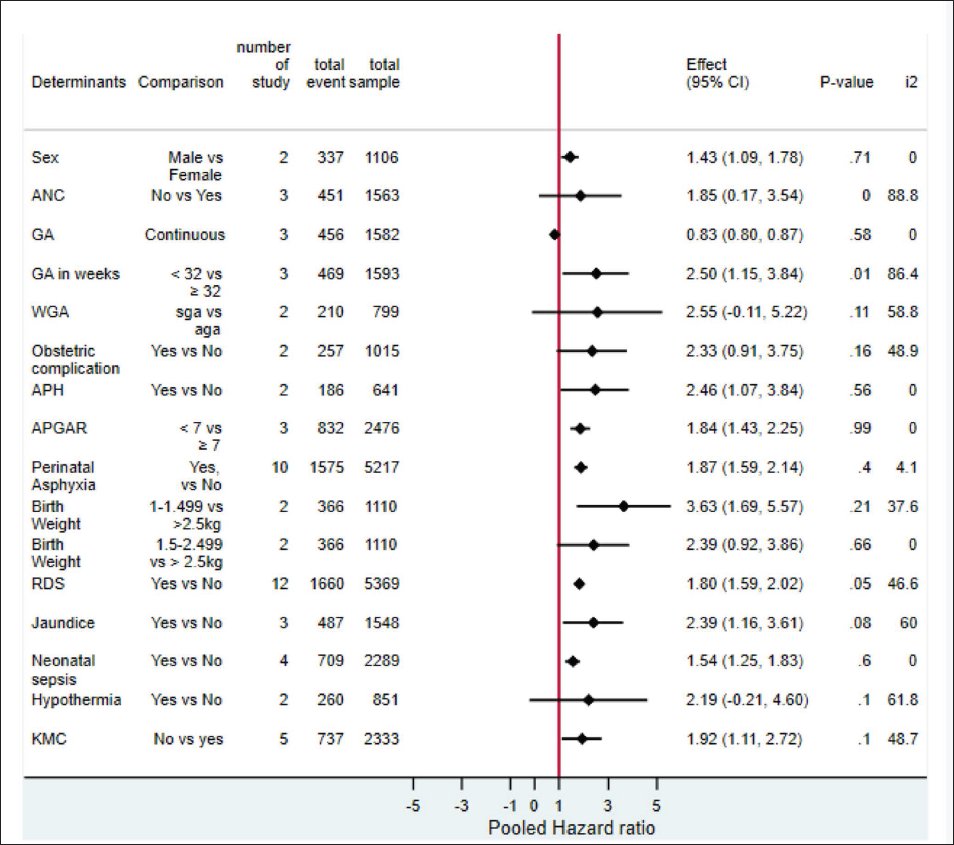
It was identified that being a male (AHR = 1.43, 95% CI: 1.09, 1.78), low gestational age (0.83, 95% CI: 0.80, 0.87), born before 32 weeks (AHR = 2.15, 95% CI: 1.15, 3.84), antepartum hemorrhage (AHR = 2.46, 95% CI: 1.07, 3.84), the 50 minutes Apgar rating less than seven (AHR = 1.84, 95% CI: 1.43, 2.25), birth asphyxia (AHR = 1.87, 95% CI; 1.59, 2.14), birth weight 1,000–1,499 g (AHR = 3.63, 95% CI: 1.69, 5.57), respiratory distress syndrome (AHR = 1.80, 95% CI: 1.59, 2.02), having a history of jaundice (AHR = 2.39, 95% CI: 1.16, 3.61), having neonatal sepsis (AHR = 1.54, 95% CI: 1.25, 1.83), and not using kanagro mother care (AHR =1.92, 95% CI: 1.11, 2.72) (Figure 4).
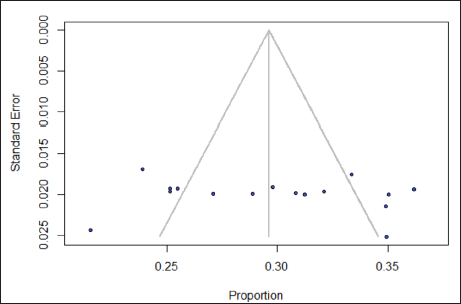
A p value of .65 for Egger’s test suggests that the symmetry of the funnel plot supports the conclusion that there is no publication bias (Figure 5).
Funnel Plot Indicating Symmetry of the Included Studies.
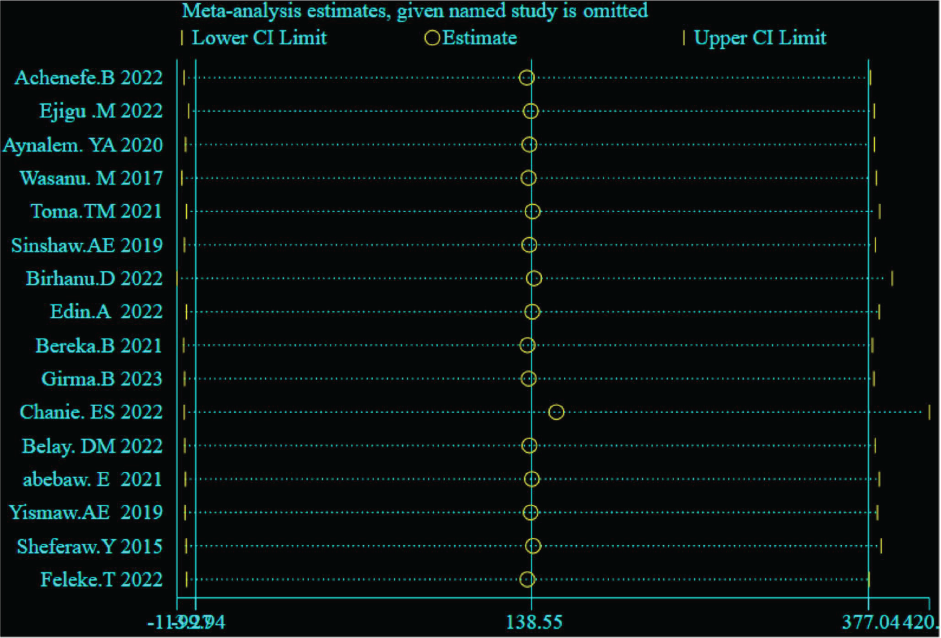
Sensitivity analysis: The finding indicates that all estimates were in the range of the final result. This suggests that none of the included research stood out from the others (Figure 6).
Sensitivity Analysis.
Discussion
The objective of this study was to assess the pooled incidence and predictors of mortality among preterm newborns receiving care at various Ethiopian health facilities. The pooled incidence proportion of preterm mortality was 30%, which is higher than findings from India, Pakistan, England, and Uganda.35–37 The discrepancy might be due to the difference in socio-economic status and infrastructure for caring the sick neonates. This finding is lower than the findings of a study conducted in the United States, 38 which might be due to the clinical condition difference, where preterm neonates in a study done in the United States had a comorbid congenital diaphragmatic hernia, which reduces survival probability and because the study design differs. Moreover, the pooled incidence density rate of premature mortality was 40 (95% CI: 30–40) per 1,000-person days.
Preterm neonates born from mothers having a history of antepartum hemorrhage were nearly three times more likely to die than those born from their counterparts. This might be due to a decreased supply of blood, oxygen, and nutrients for the fetus while in the uterus. This is an implication for increasing care for pregnant mothers during ANC follow-up.
In addition, a one-week increase in the gestational age decreases the hazard of mortality by 17%, and, compared to those born after 32 weeks, newborns born before 32 weeks had a 2.5 times higher risk of dying; study done in Nigeria supports this finding. 39 This might be due to the immaturity of the vital organs of neonates who were born early, which could be reduced during antenatal care visits. Male neonates had 1.43 higher hazards of mortality compared to females; which is contradictory to a finding of a study in Spain. 40
Preterm neonates having fifth minute Apgar score <7 had almost two times higher hazards of death compared to those having ≥7, which is supported by studies in Spain and Rwanda.40, 41 Furthermore, compared to their counterparts, preterm neonates with birth asphyxia had twice the risk of dying; which is supported by studies in Uganda and Nigeria.37, 39 This might be due to oxygen deficit during delivery leading to severe hypoxia of vital organs and becoming a double burden, which is an implication for close labor follow-up.
Preterm neonates weighing 1,000–1,499 g were nearly four times more likely to die than those weighing more than 2,500 g, which is supported by studies in Rwanda and Nigeria.39, 41 Low birth weight neonates have feeding difficulty, hypoglycemia, hypothermia, pulmonary immaturity, and fluid and electrolyte imbalance, making them more susceptible to infection. This is an implication for assuring healthy pregnancy, which is the fundamental intervention that begins before conception via full availability of family planning; pre and post-pregnancy risk identification, counseling, and reduction.
We also found that preterm neonates having a history of respiratory distress syndrome had a 1.81 times higher risk of death than those who do not have it, which is supported by studies in Uganda and Rwanda.37, 41 In addition, those having hyaline membrane disease had almost three times higher hazard of death compared to those who do not have it. It might be because the immaturity of the lung fails to produce a liquid called surfactant, which hinders the full expansion of the lungs and leads to a shortage of oxygen. So, facilities with limited access to assisted ventilation failed to help the survival of preterm neonates. Therefore, it is implication for clinicians to close follow-up of labor and policymakers to facilitate interventions needed.
Preterm neonates who had a history of neonatal sepsis, on the other hand, had a 1.54 times higher risk of death than those who did not have the disease; a study done in Rwanda also supports this finding. 41 Preterm neonates having Jaundice had a 2.39 times higher hazard of mortality compared to their counterparts. Premature neonates have immature self-defense mechanisms, so this would decrease survival probability, which is an implication for the sterile procedure during labor, delivery, and transfer to the intensive care unit.
Furthermore, neonates who did not use the kangaroo mother care had almost two times higher hazard of mortality compared to those who used it; which is supported by a study in Uganda. 37 Preterm neonates have immature organs, so kangaroo mother care helps in stabilizing the baby’s heart rate and improving breathing patterns via improving oxygen saturation levels. So, it is an implication to improve the quality of care.
This is the first comprehensive review to describe the pooled incidence and predictors of preterm mortality in Ethiopia, to the best of our knowledge. To the extent possible, different databases, including Hinari, PubMed, Google Scholar, and Cochrane Library, were searched comprehensively without regard to publication date, and gray literature was also included. To assess the quality of the studies, a structured objective NOS criterion was used. Furthermore, the review followed the PROSPERO-registered protocol. However, this study has some limitations. First, the search term was limited to English only. Second, because all of the studies included were institution-based cohort studies, the findings may not be generalizable to preterm neonates who are not admitted to health facilities. Therefore, further community-based studies that address incidence and predictors of preterm mortality should be conducted in the country. Finally, being born at the treatment center or referred there from different health facilities might have affected the survival status of those preterm neonates. Therefore, future studies should consider this variable.
Conclusion
Almost one third (30%) of preterm neonates treated at health facilities in Ethiopia failed to survive to the first month of life. In Ethiopia, the incidence rate of preterm mortality was 40/1,000 person days. The predictors of preterm mortality were being male, low gestational age, born before 32 weeks, antepartum hemorrhage, fifth minute Apgar score <7, birth asphyxia, birth weight 1,000–1,499 g, respiratory distress syndrome, jaundice, neonatal sepsis, and not using kangaroo mother care.
Therefore, we suggest non-governmental organizations that fund child care and clinicians who work in antenatal care, labor and delivery, and neonatal intensive care units to target those identified factors to improve the survival rate of preterm neonates in Ethiopia. In addition, we suggest researchers conduct further community-based studies on the survival of preterm neonates.
Author Contributions
LK was involved in conceptualizing, protocol registration process, searching, extraction, formal analysis, and manuscript writing, FR was involved in data extraction, formal analysis, and manuscript writing, and DE, SB, and DN were involved in formal analysis and manuscript writing.
Availability of Data and Materials
The dataset that supports this study finding is available online (
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.