
Abstract
Background
Breastfeeding is crucial for maternal and child health. However, mastitis and lactational breast abscesses (LBAs), pose serious health risks for nursing mothers and are traditionally treated with minor surgery, that often separates mother and child, and causes significant maternal distress. This study investigates dynamic tape (DT) as a nonsurgical intervention for LBAs that will allow breastfeeding even during treatment in postpartum Indian women.
Methods
This prospective, observational cohort study was conducted at a tertiary maternity center (Karnataka, India) between October 2017 and December 2018 [CTRI Number/2018/05/013788]. Twenty postpartum women with mastitis and LBA were subjected to dynamic taping (using DT Beige Tattoo or DT Eco based on breast size and abscess location). LBA resolution was confirmed through ultrasonography and clinical examination.
Results
Twenty participants (median age = 30 years) completed the study without adverse reactions; 65% practiced exclusive breastfeeding. Lump sizes and pus volumes were significantly reduced after treatment; 60% experienced self-drainage, 35% experienced resolution without self-drainage, and only 5% did not experience resolution; average time to resolution was 13.95 days, with each taping session lasting 3.85 days. The mean lump measurement and pus volume significantly reduced post-treatment from 108.7 cm3 and 54.58 ml to 3.14 cm3 and 1.07 ml, respectively, with 95% experiencing abscess resolution. The positive outcomes were observed during the three-month follow-up, with no recurrence of LBAs.
Conclusions
Dynamic taping resolves LBAs without surgery, by aiding lymphatic flow, reducing inflammation, and supporting breastfeeding. Larger randomized studies are required to validate its efficacy and safety.
Keywords
Introduction
The importance of breastfeeding for maternal and child health is now a global consensus. Both the World Health Organization (WHO) and the United Nations International Children’s Emergency Fund (UNICEF) strongly recommend exclusive breastfeeding for the first six months of a child’s life and encourage continuation up to the age of two years. Breastfeeding offers protection against infection and malnutrition and enhances a child’s brain development. 1 Moreover, studies have indicated that breastfeeding can increase a child’s intelligence quotient (IQ) by three to four points. Currently, the worldwide exclusive breastfeeding rate for infants aged zero to six months is 43%. 2 In the Indian context, 63.7% (59.6% in urban and 65.1% in rural areas) of children under the age of six months are exclusively breastfed. 3
Mastitis is a condition characterized by the presence of at least two breast-related signs or symptoms (such as pain, redness, or a lump) along with one systemic symptom (such as fever or flu-like symptoms) persisting for a minimum of 12 hours. 4 The worldwide prevalence of mastitis in breastfeeding women ranges from 0.4% to 11%.5, 6, 7 However, the incidence of mastitis may be as high as 33%.2, 8
The highest occurrence of mastitis typically occurs during the puerperium, with the peak incidence happening in the second and third weeks after childbirth. 4 Initially, mastitis is usually localized to one segment of the breast but can spread to affect the entire breast if left untreated. As the condition advances, it may culminate in the development of a lump, accompanied by fever, chills, fatigue, headaches, and other symptoms associated with infection and inflammation. Failure to manage the inflammation in a timely manner may result in the formation of a breast abscess in approximately 4.6%–11% of patients. 2 In the absence of intervention, certain patients may experience the drainage of pus through the skin, leading to the formation of ulcers. 2
An unnoticed or untreated infection of the breast parenchyma may eventually develop into a breast abscess (BA).9, 10 Such abscesses can be categorized into lactational breast abscess (LBA) and non-lactational breast abscess (NLBA). 11 The LBAs typically arise in young, first-time or expectant mothers as a complication of lactational mastitis. 11 On the other hand, NLBA develops due to various factors, including diabetes mellitus, smoking, and underlying structural breast issues such as duct ectasia. 11 The LBAs pose high risks to nursing mothers during two stages: in the first month after childbirth, when inexperience and inadequate hygiene can lead to nipple damage (85% occurrence), and during weaning, when breast engorgement and the baby’s teeth increase the chances of nipple trauma.11, 12 Abrupt discontinuation of breastfeeding may exacerbate an existing infection and serve as a significant risk factor for the development of LBAs. 13 While some LBAs drain spontaneously, others may necessitate interventions such as needle aspiration, incision, and drainage (I&D), or excision. 10
Antibiotics and I&D are the most common therapies for the management of LBAs in both high-income and low-income countries. 7 Also surgical intervention itself is a downer and could be a risk factor for postpartum depression in some mothers. However, recent studies have shown that ultrasound-guided aspiration is a viable option for managing these abscesses, even when they are large. 14 This approach facilitates healing in a majority of cases with several positive outcomes, including early resumption of breastfeeding, cosmetic benefits, reduced pain, and avoidance of hospitalization. 14 However, LBAs can recur even after surgical intervention; this recurrence rate has been reported to be 6.6%, though older studies have reported LBA recurrence rates as high as 40%–50%.11, 15
To reduce the recurrence of LBAs, new treatment modalities such as ultrasound therapy, 16 manual breast massage,17, 18 manual milking techniques, 19 cold and warm applications,6, 20 cabbage leaf compressions,21, 22 manual lymphatic drainage (MLD), 23 and Kinesio taping (KT)9, 24 are gaining popularity; most of these treatments are associated with low or no reported adverse effects.
The KT method uses an elastic, water-resistant, and air-permeable band to alleviate breast engorgement.9, 24 Studies have indicated that KT, with its capacity for regulating movements in the fascia and facilitating lymphatic collectors, can alleviate symptoms of engorgement, as well as pain and stiffness.9, 25 Since engorgement and increased breast milk can lead to an increase in fluid volume and weight in the breast, which may obstruct lymphatic drainage, KT application along with complex decongestive therapy can be very effective in reducing lymphedema in breasts.9, 26 However, studies have also shown that MLD plus routine breast care was more efficacious in reducing breast pain, engorgement, and milk volume than KT plus routine care or routine care alone. 9 Moreover, some studies revealed that KT did not have a significant impact on the incidence of breast engorgement. 23
Considering these issues with KT, this study explores the use of dynamic tape (DT) in the management of LBAs in Indian women. Dynamic tape is a specialized tape made from a Visco-elastic blend of nylon and Lycra and was developed by an Australian physical therapist, Ryan Kendrick, in 2009. 27 This tape possesses unique properties, including four-way stretchability, strong elastic resistance, and recoil; DT can stretch up to at least 200% (unlike KT, which stretches to about 140%) of its original length, with no rigid.27, 28, 29 By using DT to lift and support the weight of the breast, the occlusion in the lymphatic vessels of the breast is reduced and lymphatic drainage is stimulated; this in turn, helps decrease the perception of pain, promotes blood circulation, and allows faster healing. This study explored the effectiveness of DT as a non-surgical intervention for treating LBAs in postpartum women in India.
Materials and Methods
Study Design
This study was a prospective, observational study conducted in 2018 at a tertiary maternity center in Bangalore, Karnataka, India with the primary objective of exploring the effectiveness of DT as a non-surgical intervention for treating LBAs in postpartum women. The secondary aim of this study was to develop a viable non-operative alternative treatment method to resolve LBAs and to reduce the chances of milk suppression.
Inclusion Criteria
The study enrolled 20 postpartum women who were diagnosed with the conditions mentioned below.
Gigantomastia Engorgement of breast Pathological engorgement Blocked duct Mastitis Areolar edema Breast Abscess
Exclusion Criteria
Those who presented with burnt skin around the breast area due to hot/cold compression and unable to provide written informed consent were excluded. A patch sensitivity test was conducted to check for any allergic reactions; participants who developed any allergic reactions were sent to their primary consultant for further follow-up.
A detailed written informed consent for participation & photographing the procedure was obtained from the participants.
Ethics Approval
This study obtained ethical clearance from the Institutional Ethics Committee.
All participants were given a detailed explanation regarding the treatment procedures involved and prior to their participation, a written informed consent was obtained, indicating their voluntary consent to participate in the study. Also, written informed consent was taken for photographing the treatment procedure & de-identified usage.
Dynamic Tape Application
The study employed two types of DTs, based on the size of the breast, the abscess, and its location.
The principal investigator certified in DT therapy applied, monitored, and recorded the outcomes of the same.
Pre-application Assessment
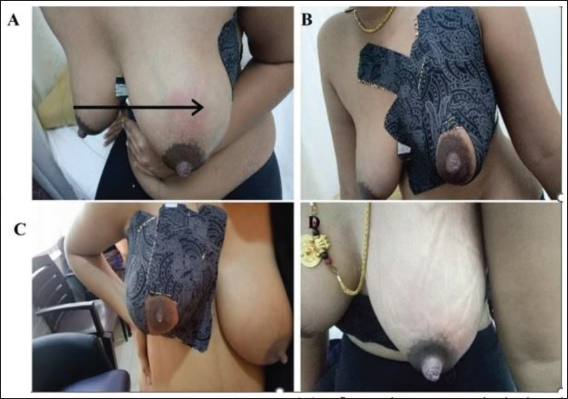
After a comprehensive clinical evaluation and diagnosis, participants were counselled by a certified lactation consultant. All the participants underwent an ultrasound examination to determine the size and volume of the abscess before the treatment. Additionally, a patch sensitivity test was performed for 15 minutes to assess adverse reactions to the adhesives used in the DT. Participants who exhibited any symptoms such as itching, erythema, or a burning sensation were excluded from the study and referred for appropriate medical management. The participants in the trial who had a negative patch test were excluded. Following a thorough clinical examination and assessment, DT was applied to the breast, carefully avoiding the areolar area. The tape was then rubbed to activate the heat-sensitive glue and enhance skin adherence. Strips of tape were applied to promote MLD and compression of the breast tissue (Figure 1A & B).
Post-application Assessment
To enhance lymphatic drainage, participants were advised to perform upper limb mobility exercises and simple breathing exercises for stress management. The referring consultant also prescribed anti-inflammatory agents and antibiotics as part of the treatment plan. Breastfeeding was recommended, as it was anticipated that the repeated suckling by the baby and the stretching of the superficial skin in the opposite direction due to the DT would aid in better lymphatic drainage and help gather pus at one location in the case of multicentric abscesses. Once this occurs, the pus would naturally ooze out at periodic intervals through a natural opening. If the mother was unable to breastfeed, syringing or hand expressing was advised. Participants were scheduled for a review after three days or earlier.
Follow-up
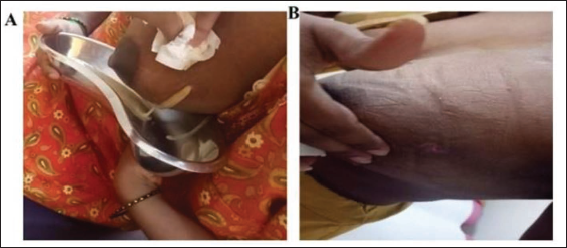
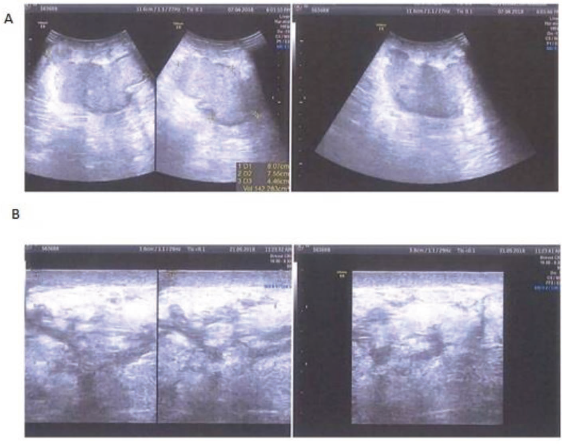
During the first follow-up (fourth day) of the tape application, the tape was carefully removed in the direction of hair growth. A clinical examination was performed to assess any changes in the breast lump, including size, redness (erythema), firmness (induration), and sensitivity (tenderness) (Figure 1C & D). The skin was also checked for any signs of allergic reactions to the tape. The taping procedure was then repeated every third day for a maximum of six taping sessions or until the breast lump was resolved. The treatment was considered successful if the LBA was completely resolved, with or without a natural opening (Figure 2A and B). The confirmation of complete LBA resolution was validated via ultrasonography (Figure 3A and B) and clinical examinations by our lactation consultants and respective obstetricians. The participants were followed up for a further period of six months to check for any recurrence of LBAs. No reoccurrences were reported.
Statistical Analyses
Collected data were entered in Excel and analyzed using R software version 4.0.2. Continuous variables were presented as median and range. The medians of the pre and post-taping values were compared using the Wilcoxon signed-rank test and a p value of <.05 was considered statistically significant.
Results
A total of 22 participants were screened. Of these, 20 participants did not exhibit any adverse reactions during the patch test and were therefore included. Two patients declined consent and were hence excluded (Figure 4). Of the 20 enrolled, 16 (80%) were primiparous mothers, 70% delivered via
A Flowchart Indicating the Design of the Study.
Cesarean section and the remaining had normal vaginal deliveries. Of the 20 babies, nine were inborn and 11 were outborn and presented to the lactation consultant in the out-patient department.
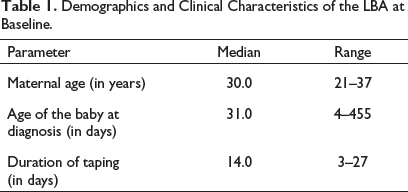
The median age of the participants was 30 years (Range: 21–37 years). Out of the 20 women in the cohort, 16 (80%) were primiparous mothers (Table 1).
Demographics and Clinical Characteristics of the LBA at Baseline.
Resolution of the LBA through self-drainage occurred in 12 (60%) participants; in 7 (35%) participants, the LBA resolved without self-drainage, and the LBA in 1 (5%) participant could not be resolved by dynamic taping despite multiple taping sessions due to the depth of the abscess (>5 cm) (Table 2; Figure 5).
Comparison of LBA at Pre- and Post-taping

Graph Showing the Measurements of the LBAs Before and After Application of DT.
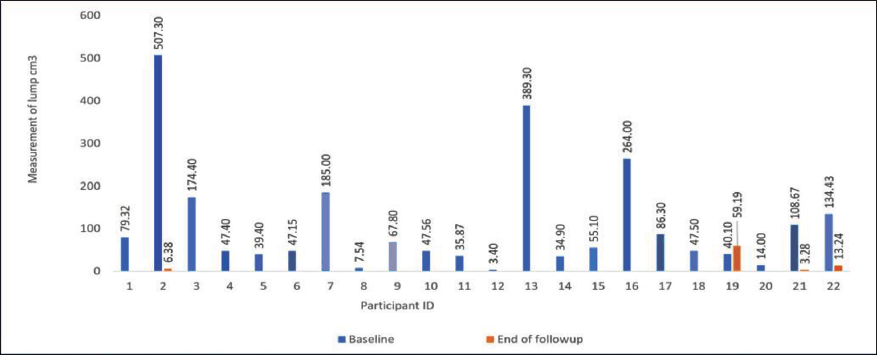
The average lump measurement and pus volume at diagnosis were 108.7 cm3 and 54.58 ml, respectively. Following treatment, these values were reduced to 3.14 cm3 and 1.07 ml, respectively (Table 1). An impressive 95% of the participants experienced complete LBA resolution on average, after 13.95 days of taping (with each taping session lasting on average 3.85 days); notably, breastfeeding was not interrupted during this period for any of the participants.
At baseline, exclusive breastfeeding was practiced by 13 (65%) women, 5 (25%) used methods of syringing and hand expression, and 2 (10%) women did not breastfeed (Figure 6). Among the two women who were not breastfeeding, one had a baby with a cleft palate and another baby was in the process of weaning with complementary feeding.
Women Practicing Exclusive Breastfeeding and Alternative Forms of Feeding Before and after the Resolution of the LBA.
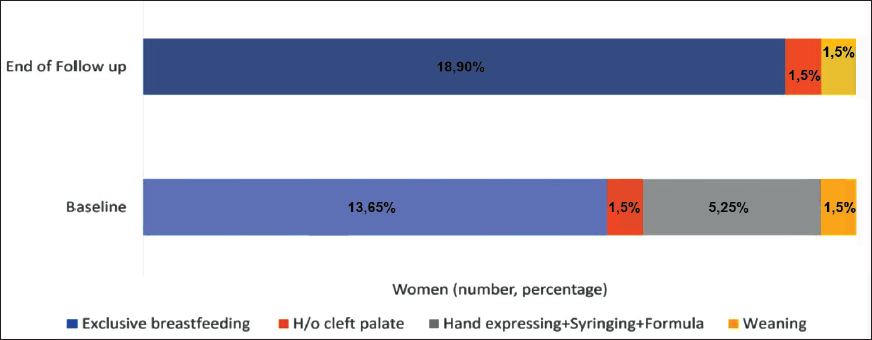
Post-treatment, all participants were breastfeeding except for one participant who had a baby with a cleft palate. The three-month follow-up showed positive outcomes, with no recurrence of LBAs, scar formation, or skin puckering at the sites of natural openings.
Discussion
This study aimed to investigate the efficacy of the DT in the management of mastitis and resolution of LBA in postpartum women. The results indicate promising outcomes for the use of dynamic taping as an adjunctive treatment, which promotes resolution through self-drainage without the need for surgical interventions.
The demographic characteristics of the study participants revealed a mean age of 28.7 years with 80% being primiparous mothers. This finding is consistent with previous studies demonstrating the higher susceptibility of first-time mothers to mastitis and LBA due to the learning curve associated with breastfeeding and potential difficulties in setting up proper latch and positioning responses with the baby. 7 The mean age of the baby at diagnosis was 71.2 days; although in most cases, mastitis and LBA occur in the first few weeks postpartum (within six weeks), these conditions can occur as late as 12 weeks to six months postpartum.11, 30, 31 In many Indian households, new mothers typically have family support (mothers/mothers-in-law who help care for the family and baby) that lasts for two to six months, the delayed presentation of LBAs in this cohort could be due to stress, inexperience and inadequate hygiene as family support becomes after two months and the new mothers adjust to these conditions. In this study, dynamic taping was performed using two different types of DTs, namely, DT Beige Tattoo and DT Eco. The DT enhanced lymphatic drainage, reduced inflammation, and supported the affected breast tissue during breastfeeding. Patients demonstrated good compliance with the taping procedure. No adverse reactions were reported, suggesting that dynamic taping is a safe and economical option for adjunctive therapy in the management of LBA.
Among the 20 participants enrolled in the study, most (60%) experienced resolution of the LBA through self-drainage, indicating that the DT effectively facilitated lymphatic flow and pus drainage; 35% achieved a resolution without self-drainage, suggesting that the DT may have helped reduce inflammation, leading to abscess resolution without spontaneous drainage. Only one participant (5%) did not experience resolution due to the depth of the abscess (>5 cm) from the skin surface. This is a limitation of dynamic taping; it cannot be used to treat deep-seated abscesses, which need alternative management strategies.
Breastfeeding may have profound impacts on the outcomes of DT used for LBA resolution as the repeated suckling action of the baby likely aids in better lymphatic drainage and gathering of pus at one location, facilitating natural drainage. For mothers unable to breastfeed, alternative methods such as syringing, hand expression, or formula feeding were recommended.
The success of DT (complete resolution of LBAs with or without natural openings) was confirmed through ultrasonography examination. The absence of scar formation and skin puckering at the site of the natural opening during the three-month follow-up suggests that the DT contributes to better cosmetic outcomes.
In summary, DT of the breast tissue can help in resolving LBAs without the need for surgical intervention as the DT stimulates lymphatic flow by directing it in the appropriate direction. This action helps uplift the skin, reducing the pressure on the damaged tissue, and restoring the skin’s texture by reducing inflammation. The tape’s elastic recoiling effect accommodates the influx and outflux of milk during breastfeeding, providing support to the breast tissue.
Strengths and Limitations of this Study
This study is the first to explore the use of DT as a non-surgical alternative for LBAs in an Indian setting. However, the low sample size, lack of a control group, and single-center design of this study may limit the generalizability of its results. Furthermore, the lack of a control group and randomization might have introduced biases and confounding factors. Future studies with larger cohorts and randomized controlled designs are warranted to validate the efficacy and safety of DT in the management of mastitis and LBAs.
There is preliminary evidence that decongestive therapy using dynamic tape is a promising non-surgical and minimal/pain-free technique that is cost-effective and devoid of side effects compared to invasive procedures. This technique also circumvents the need for maternal separation and cessation of breastfeeding. This is a boon for maternal and child health as it reduces the use of formula feed at a tender age which is financially beneficial for specific socio-economic demographics in developing countries where the cost of formula feeding can be hugely burdensome for families.
Conclusion
The results of this study indicate that DT allows continued breastfeeding while facilitating abscess resolution and reduction in symptoms through self-drainage this reduces the need for surgical interventions, making DT a viable, non-operative alternative treatment method for LBAs that reduces milk suppression. Exclusive breastfeeding appears to be a favorable factor in achieving successful outcomes. Thus, the use of DT for treating LBA has emerged as a novel, non-surgical, and minimally invasive technique. It offers a non-nociceptive (non-painful) treatment allowing uninterrupted breastfeeding circumventing the need for maternal separation and cessation of breastfeeding during treatment. However, further studies are needed to validate these findings and explore the broader applicability of DT in different populations and healthcare settings.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to Shalini Wiseman (MSc, POGP, MISCP; Clinical Lead, The Cork Women’s Health, Cork Clinic (Ireland) – who reviewed the manuscript, gave critical appraisal and helped design the final manuscript and Ryan Kendrick (MPhtySt, BPhty (MSK); Port Vila, Vanuatu, Posture Pals Private Limited).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Disclaimer
The authors have no connection to the brand product or services and have not received any funding or any compensation for using the product in this study.
Ethical Approval and Patient Consent
This study obtained ethics clearance from the Institutional Ethics Review Board of Cloudnine Hospital Jayanagar, Bangalore, India. Written informed consent was obtained from all 20 women enrolled in the study, indicating their voluntary agreement to participate in the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.