
Abstract
Idiopathic granulomatous mastitis is a benign chronic inflammatory breast disease and a confused treatment plan may result in worsening of the disease, unacceptable cosmetic damage for the patient and even mastectomy. We report a case of a 39-year-old Chinese woman with a two-month history of painful, solid, diabrotic, left breast lesions that measured 10 × 15 cm. Misdiagnosis had led to delayed wound healing with extensive ulcerative skin lesions. The patient was successfully treated with oral corticosteroids and bromocriptine without requirement for surgery.
Introduction
First described in 1972, 1 idiopathic granulomatous mastitis (IGM) is an uncommon, benign and chronic inflammatory breast disease. It is characterized clinically by breast lumps with sinus formation and abscesses, and histologically by the presence of non-caseous granulomatous lobulitis, infiltrated by neutrophils, epithelioid histiocytes and multinucleated giant cells. 2 Although its exact aetiology is unknown, possible causes include autoimmune diseases, foreign body reaction, fungal or parasitic infections, hyperprolactinemia and the use of oral contraceptives. 3 Management of the condition remains controversial.4–7 A commonly used treatment is wide surgical excision of the mass but this procedure is associated with high recurrence rates, skin ulceration, fistula formation, and wound infection, especially in patients with extensive inflammation. 8 Corticosteroid therapy with or without surgery has also been reported to be effective.4–7 Other treatments that have been used include, antibiotics, prolactin lowering agents, colchicine, azathioprine and methotrexate. 3 , 7
We report here on a case of severe IGM that was successfully treated with oral corticosteroids and bromocriptine without the requirement for surgery.
Case report
This case study was approved by the ethical committee of Guangdong Women and Children’s Hospital and the patient provided written informed consent for publication of this report and any accompanying images.
A 39-year-old Chinese woman (gravida 2, para 1, abortus 1) with no significant past medical history presented to our breast clinic with a two-month history of painful, solid, diabrotic, left breast lesions that measured 10 × 15 cm (Figure 1). She had not suffered any other symptoms such as nodal erythema or fever. She had one child whom she had breastfeed for one year. During lactation, she had experienced galactostasis and was prescribed cephalosporin antibiotics for >10 days. Her condition worsened and at her local hospital she subsequently had a core needle biopsy taken of a lesion which had developed on her left breast. Chronic suppurative inflammatory changes were identified from histopathology. She was prescribed anti-tuberculosis treatment and received isoniazid (0.3 g/day), rifampicin (0.45 g/day) and pyrazinamide (0.75 g/day) for one week and her lesions improved slightly but there were no significant signs of remission.

Patient presented to our breast clinic with a two-month history of painful, solid, diabrotic, left breast mass (10 × 15 cm). Signs of inflammation, spotty necrosis, and haemorrhage were present.
Twenty days after treatment had stopped the abscess was punctured at the local hospital and thin yellow pus flowed from the puncture site. Unfortunately, the exudate was not examined for bacterial culture. The wound did not heal and the surface swelling became more pronounced (Figure 2). The ulcerated skin bled easily and had a white discharge on its surface. The patient was still able to express milk from the nipple without retraction. The patient was referred to our clinic.

After a local puncture, thin yellow pus spilled out of the wound and there was pronounced surface swelling.
Investigations showed that the patient had a normal chest X-ray but an ultrasound scan of her left breast demonstrated a huge inhomogeneous hypo-echoic area. Mammography was not performed because of the wide-ranging inflammation. Routine blood tests showed that her white blood cell count (15.4×109/l), neutrophil count (12.9×109/l) and neutrophils (83.8%) were elevated. Her haemoglobin was low at 95 g/l, but her levels of C- reactive protein (39.0 mg/l), prolactin (990 mIU/l), gamma-glutamyl transferase (79 U/l) and uric acid (660 umol/l) were also elevated. Levels of complement C4 (0.44 g/l), immunoglobulin (Ig) G (16.3 g/l) and IgM (1.4 g/l) tended to be high and albumin levels (37.5 g/l) were slightly lower than the normal range.
Core needle biopsy of the lesion showed granulomatous inflammation with multinucleated giant cells, epithelioid histiocytes and neutrophils, occasional features of fat necrosis and micro abscesses (Figure 3). Bacterial cultures of secretions from the breast ruptured skin surface, breast tissue and pus were negative. A diagnosis of IGM was made. Total mastectomy and breast reconstructive surgery were offered to the patient but she rejected this proposal because of her personal circumstances and financial situation.
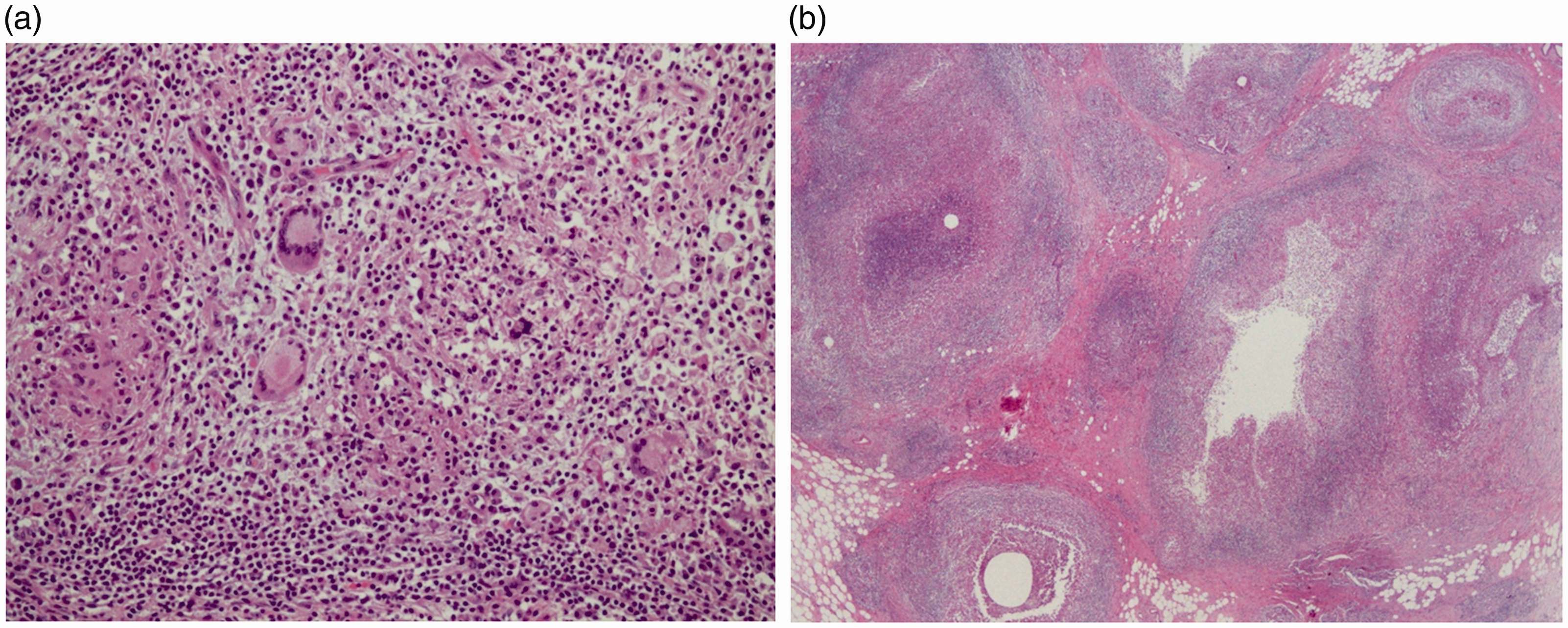
Pathologic histology showed (a) granulomatous inflammation with multinucleated giant cells, epithelioid histiocytes and neutrophils, and (b) occasional features of fat necrosis and micro abscesses.
She was prescribed oral methylprednisolone (20 mg/day) for three months and bromocriptine (2.5mg/day) for six months. After two days of treatment, the mass began to shrink and there were fewer secretions on the surface (Figure 4). Over the next month, the mass decreased significantly in size and the ruptured surfaces improved (Figure 5). At three months the lesion had shrank completely and no palpable lumps were detected. Corticosteroid therapy was reduced to 4mg/day for a further six months (Figure 6). At a five-year follow-up, the patient reported that there had been no recurrence.

Following treatment with oral methylprednisolone (20 mg/day) and bromocriptine (2.5 mg/day) for two days, the mass began to shrink and the ruptured surface became drier with fewer secretions.

Over the next month, the mass decreased significantly in size and the ruptured surfaces improved.

At three months the lesion had shrank completely and no palpable lumps were detected.
Discussion
Idiopathic granulomatous mastitis is a rare benign disease of unknown aetiology. 9 Moreover, its clinical and radiological manifestations are similar to breast cancer and tuberculosis mastitis making it difficult to diagnose and treat. 5 In western countries, tuberculosis mastitis is rare and associated with only 0.1% of all breast lesions, but in developing countries, it accounts for almost 3% of breast conditions. 10 Therefore, physicians must be cautious when examining patients from high-risk populations or endemic areas. 11 In the case reported here, it appears that tuberculosis was initially suspected but although the lesions improved, the patient showed no significant signs of remission after receiving different types and doses of antibiotics for seven days. While there are no guidelines or consensus for diagnosis or treatment of IGM,4–7 before microbiological evidence and a pathological diagnosis are obtained, empirical antibiotic therapy has been recommended by several authors, particularly for patients with cellulitis, abscesses and sinus secretions.8–10
Although the causes of IGM are unclear, primary or secondary hyperprolactinemia may have a role in the pathogenesis of the condition. 12 Indeed, hyperprolactinemia causes a continuous production of breast intraductal secretions which may well prompt a local immune response. 13 Therefore, in the diagnosis of IGM, measuring serum prolactin is important. For example, the serum prolactin levels in this patient were elevated (990 mIU/l) and so bromocriptine was prescribed as part of her medical therapy.
Some authors consider surgical excision to be the treatment option of choice for IGM, 14 However, excision is not always possible, particularly for patients with advanced invasion 9 and it has been associated with several side effects. 8 In this present case, surgical treatment in the first instance was not appropriate since it would have required wide excisions and rectus abdominis or latissimus dorsi flap repair surgery. Oral corticosteroids are regarded by several authors as the treatment of choice for conservative management7,10 and they have been used successfully before and after surgery.8,10 Some reports suggest that treatment with corticosteroids provides significant regression of the granulomatous mass therefore permitting more conservative surgery. 5 In this present case, methylprednisolone was prescribed for a total of nine months and bromocriptine for six months. The breast mass shrank and the ruptured surface converged markedly. Although corticosteroids have proved a successful treatment for IGM, patients should be closely observed for potential adverse effects such as Cushing’s syndrome, weight gain, osteoporosis, and glucose intolerance. 7 , 14 In addition, the exclusion of an infectious aetiology is essential before corticosteroid treatment commences. 9 , 14
In summary, IGM is a benign but devastating disease and a confused treatment plan may result in severe disease that causes unacceptable cosmetic damage for the patient and even mastectomy. Diagnosis should combine pathological features with clinical, radiological and microbiological evidence. Treatment should be established following a fully integrated clinical and pathological profile of the patient, real-time microbiological evidence and consideration of any potential side effects of treatment. Surgical treatment may possibly be avoided by appropriate systemic medication.