
Abstract
Background:
This study examines the interaction between childhood trauma, emotional regulation, and externalizing symptoms among adolescents aged 13 to 19 years, elucidating the role of emotional regulation as a mediator in the relationship between childhood trauma and externalizing behaviors.
Methods:
This study utilizes a cross-sectional observational study design. A sample of 182 adolescents attending child and adolescent services was assessed. Demographic characteristics were analyzed using descriptive statistics. Childhood trauma was measured using the Childhood Trauma Questionnaire— Short Form (CTQ), emotional regulation through the Difficulties in Emotion Regulation Scale (DERS), and externalizing symptoms using the Child Behavior Checklist (CBCL). Hierarchical multiple regression and mediation analyses were conducted to explore the relationships.
Results:
Most participants were 16–19 years old (66.5%), and 54.9% were female. Notably, childhood trauma positively correlated with externalizing symptoms (r = 0.39, P < .001) and difficulties in emotion regulation (r = 0.25, P < .01). Emotional regulation, as measured by DERS, exhibited a significant positive correlation with externalizing symptoms (r = 0.23, P < .01). Hierarchical regression analysis revealed that emotional regulation played a significant role in predicting externalizing scores (b = 0.358, P < .001). Mediation analysis demonstrated both direct (B = 0.16, P < .001) and indirect effects (B = 0.036, P = .0273) of childhood trauma on externalizing behaviors through emotional regulation.
Conclusions:
This study underscores the multifaceted nature of externalizing behaviors and highlights the interconnectedness of childhood trauma and emotional regulation in their manifestation. Findings suggest that utilizing emotion regulation strategies is pivotal in treatment of externalizing symptoms among adolescents presenting with traumatic history. The proposed mediation model provides valuable insights for developing targeted interventions and preventive strategies in clinical settings.
Keywords
Introduction
Adolescence, a critical developmental phase marked by increased autonomy and identity formation, is often fraught with challenges that can influence psychosocial well-being. One pivotal aspect of adolescent mental health is the emergence of externalizing behaviors, encompassing a spectrum of disruptive conduct such as aggression, rule-breaking, and substance abuse. 1 Understanding the intricate relationship between childhood trauma, emotional regulation, and the manifestation of externalizing symptoms holds paramount importance in both research and clinical domains which will inform us about the treatment in focus. Previous research has suggested that compared to parents with normally developing children, parents with externalizing children reported more negative impact on social life, more negative and less positive feelings about parenting, and higher child-related stress. 2 Research evidence that childhood externalizing disorders are the harbinger of alcohol dependence. 3 The development trajectory starting from early childhood externalizing disorders has the potential to culminate in adult psychopathologies especially addiction which carries a huge burden of care. There is a window of opportunity to manage externalizing disorders early on if the underlying pathways are understood well.
Childhood trauma, encompassing various forms of abuse and neglect, has garnered considerable attention for its potential long-term consequences on mental health. 4 Adverse childhood experiences have been implicated as robust risk factors for a myriad of psychopathological outcomes, including externalizing behaviors. 5 While direct associations between trauma exposure and externalizing symptoms are established, the nuanced mechanisms underlying this relationship remain less explored.
Emotional regulation, the capacity to modulate emotional responses and manage distress, serves as a cornerstone of adaptive psychological functioning. 6 However, difficulties in emotion regulation have been identified as precursors to various psychopathological outcomes, particularly externalizing behaviors. 7 The role of emotional regulation as a mediator between childhood trauma and externalizing symptoms could provide valuable insights into the intricate pathways through which early trauma manifests as maladaptive behaviors during adolescence especially managing one’s emotions.
There are a number of risks and protective connections between attachment security and developmental process that are associated with externalizing behavior. 8 The relational processes get affected in the presence of childhood trauma due to the threat to attachment system early on which effects the domain of emotional regulation too. Externalizing problems are marked by emotional and behavioral lability, and the under-regulation of negative affect thus shedding light on the intricate mechanisms underlying externalizing behaviors contributes to the broader discourse on developmental psychopathology and fosters a more holistic perspective on adolescent mental health. A comprehensive understanding of the interrelationships among these constructs can inform mental health professionals about the assessment strategies, tailor interventions, and inform policy decisions to optimize the psychosocial well-being of adolescents. Thus, this study is poised to fill the gap in understanding externalizing disorders by mapping psychological pathways that could contribute to their development and maintenance. Researchers aim to study the mediating role of emotional regulation in presence of childhood trauma.
Methodology
All adolescents aged between 13 and 19 years and attending the child and adolescent services at Institute of Human Behaviour and Allied Sciences (IHBAS) were approached. Purposive sampling was utilized for the recruitment of patients. A previous study 9 from a tier 2 city in the northern part of India reported a large proportion of the sample with childhood abuse or neglect (83.36%), and experienced symptoms of one or more psychiatric disorders (83.33%). However, there is no such prevalence data available from India. Hence, the authors aimed to screen all adolescents attending the clinic over the continuous duration of three months. Adolescents aged between 13 and 19 years able to understand Hindi or English providing assent and consent by parents were included in the study. All adolescents with neurodevelopmental disorders, intellectual disability, or any chronic physical illness that may have affected the normal developmental course or inflated distress, any severe mental illness or physical illness interfering with the ability to give assent, or parents’ ability to provide consent are excluded from this study. The parents were interviewed on any presenting complaints suggestive of externalizing symptoms like hostility, aggression, truancy, impulsivity, inattention, or any other. Adolescents were interviewed on Child Behavior Checklist (CBCL) and self-rated on Difficulties in Emotion Regulation Scale (DERS) in the preferred language (English/Hindi). The researcher interviewed the participants on Childhood Trauma Questionnaire—Short Form (CTQ) measure.
Procedure and Ethical Considerations
This study was approved by the institute’s ethics committee before starting the study. A team of mental health professionals including a psychiatrist and clinical psychologist diagnosed the adolescents and screened them for the study. Assent from the participants and consent from the parents was obtained after the researchers explained the purpose and procedure of the research to the selected participants. They were informed about the anonymity and their right to withdraw from the study which will not imply their treatment as usual. Adolescents presented with the risk of harming themselves or others during the interview were provided with immediate crisis support by the trained professional embedded within the facility through appropriate referral thus not interfering with their treatment as usual.
Measures
Sociodemographic proforma and clinical data were collected for each participant. CBCL—youth self-report measure 10 included 113 items with a three-point Likert-scale response format that can be summarized into three scales: Externalizing, internalizing, and total problems. Only an externalizing scale was utilized for the study and both subsyndromal and clinical scores were considered. CTQ 11 was used to determine the degree to which adolescents had previously suffered emotional (EA), physical (PA), and sexual abuse (SA) as well as emotional (EN) and physical neglect (PN). It is a Likert scale ranging from 1 = never to 5 = very frequently true. Test-retest reliability varied from 0.66 to 0.94, while the alpha reliability for internal consistency ranged from 0.70 to 0.93. The DERS 12 was used which is a commonly used self-report measure of subjective emotion ability. Since it’s a self-rated measure, participants could prefer to fill in the preferred language (Hindi/English). The scale has well-established psychometric properties.
Statistical Analysis
The demographic characteristics of adolescents will be described using descriptive statistics. For data analysis, R 13 was used for correlation, regression, and mediational and moderation analysis using the Hayes Macro Process plugin. 14
Results
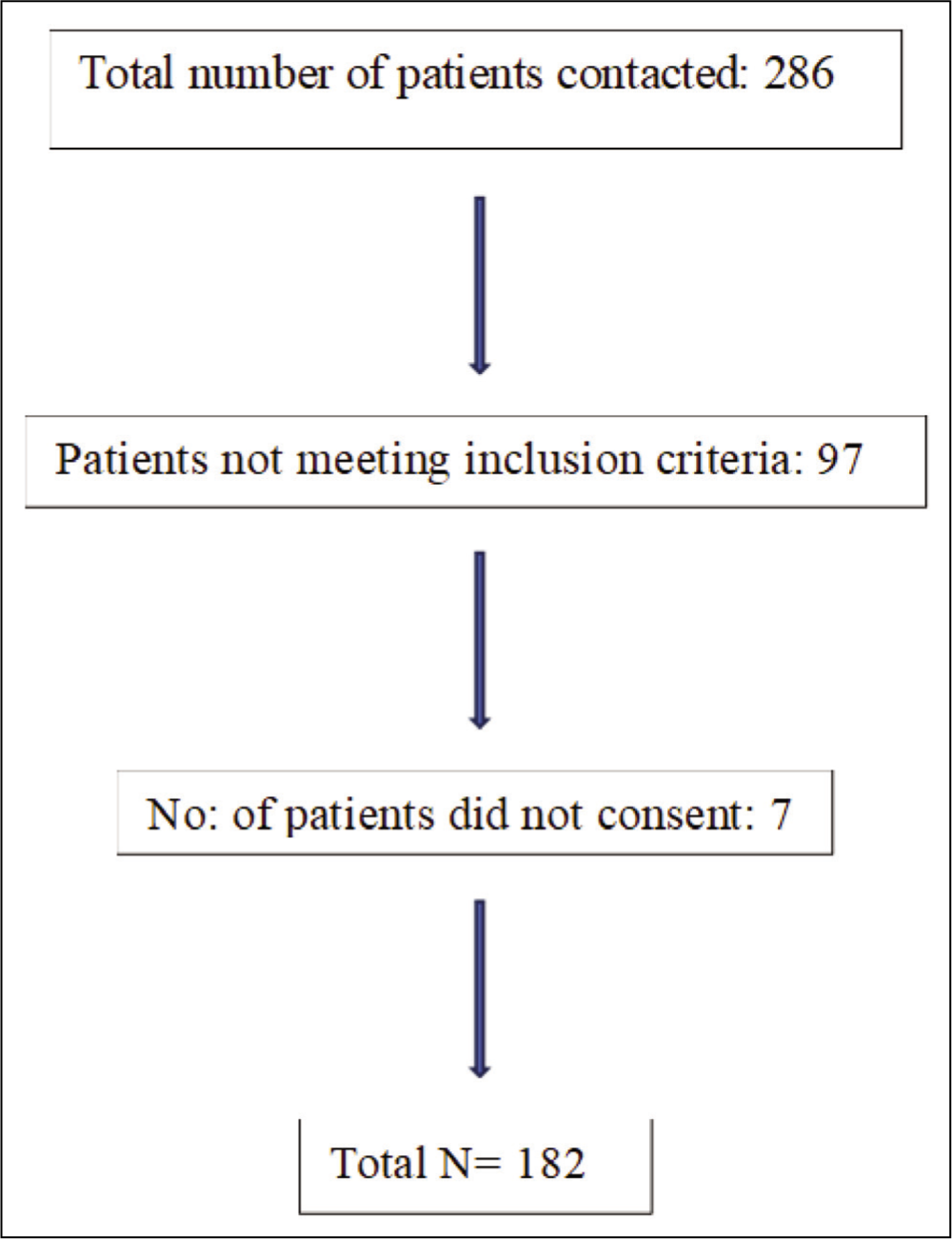
To ensure that the assumptions of normality were not violated, preliminary analyses were conducted using the Kolmogorov-Smirnov statistic, which was nonsignificant for all variables except CTQ scores. The multivariate normality assumption was addressed in the mediation analysis using bootstrapping, thus increasing the accuracy of the conclusions drawn from this research. Multicollinearity was acceptable after conducting collinearity diagnostics (tolerance values >0.2, and variance inflation factors values <10). Figure 1 shows the sample selection, and the sociodemographic characteristics of the study participants (n = 182) are presented in Table 1. Around 33.5% of the sample population were between 13 and 15 years old, while 66.5% fell within the 16 to 19 age group. Gender distribution showed that 45.1% were male and 54.9% were female. Regarding education, 36.8% had completed middle school or below, while 63.2% had attained senior school level or above. Family income distribution revealed that 52.2% were categorized as lower income, 36.8% as middle income, and 11% as upper income. Living arrangements indicated that 17% of participants resided with one parent, while the majority (83%) lived with both parents. In terms of residence, 29.8% were from rural areas, 23.6% from semi-urban areas, and 47.8% from urban settings. Sibling distribution demonstrated that 11% had no siblings, 33% had one sibling, 23% had two siblings, and 33% had three or more siblings. Order of birth analysis indicated that 40.1% were the eldest, 46.2% were in middle birth order, and 13.7% were the youngest in their families. Family history of psychiatric illness was reported by 13.2% of participants, and 23.6% had a lifetime history of psychiatric illness. A small proportion (8.8%) exhibited a risk of suicide.
Flow Chart of Participant Recruitment and Inclusion.
Sociodemographic and Clinical Profile.
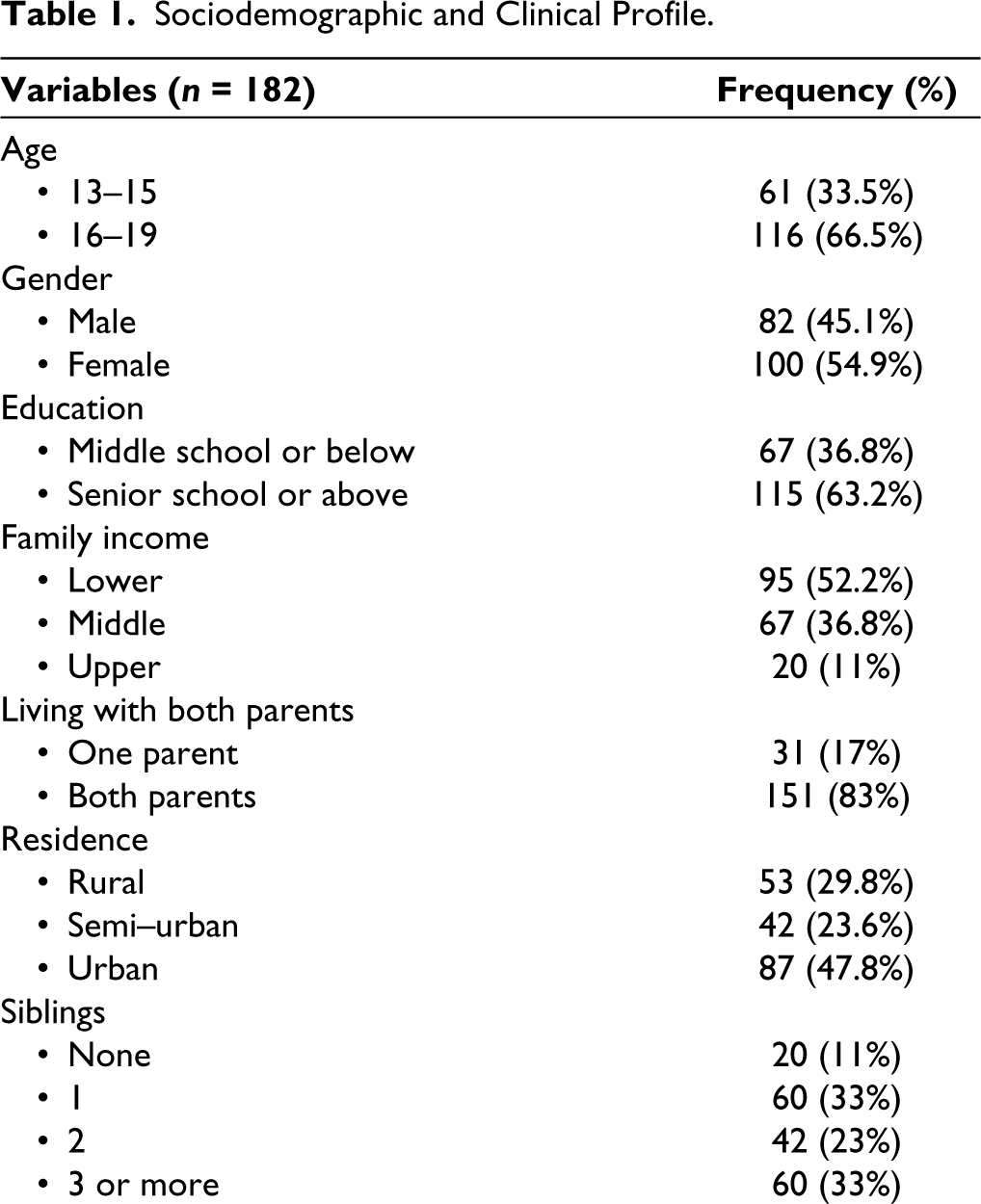
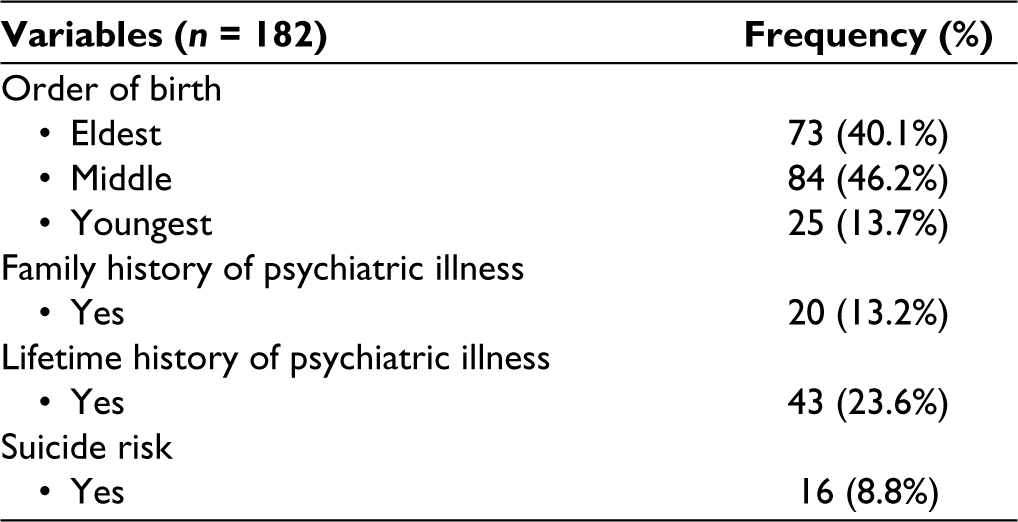
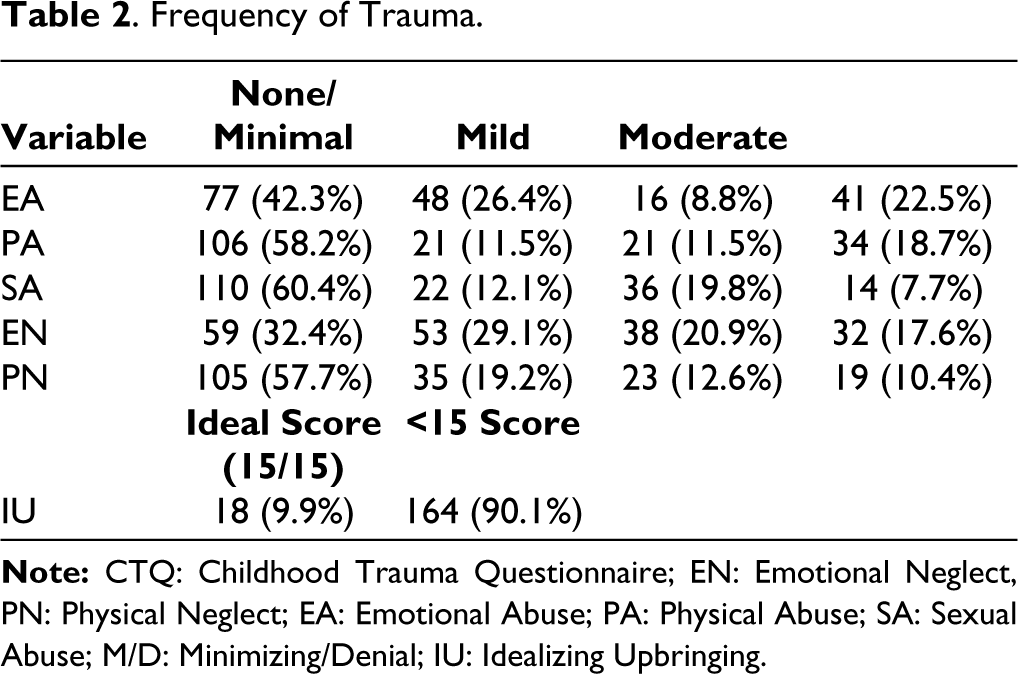
Table 2 provides a comprehensive overview of the frequency of trauma experienced by the study participants, categorized into different levels of severity for various types of childhood trauma, including EA, PA, sexual abuse (SA), EN, and physical neglect (PN). The data indicate that a substantial proportion of adolescents reported experiencing some level of trauma. Notably, for EA, 22.5% of participants reported severe trauma, while 42.3% reported none/minimal trauma. In the case of PA, 58.2% of adolescents reported none/minimal trauma, while 18.7% experienced severe trauma. For SA, 60.4% reported none/minimal trauma, and 19.8% experienced moderate trauma. EN was reported as none/minimal by 32.4% and as severe by 17.6% of participants, while PN was reported as none/minimal by 57.7% and as severe by 10.4% of participants. Additionally, a noteworthy proportion of participants (90.1%) scored below the ideal score of 15 on the idealizing upbringing (IU) scale, indicating a significant number had experiences inconsistent with an idealized childhood. The key findings reveal the prevalence and varying degrees of childhood trauma in the study population, underscoring the need for further investigation into its impact on emotional regulation and externalizing symptoms among adolescents.
Frequency of Trauma.
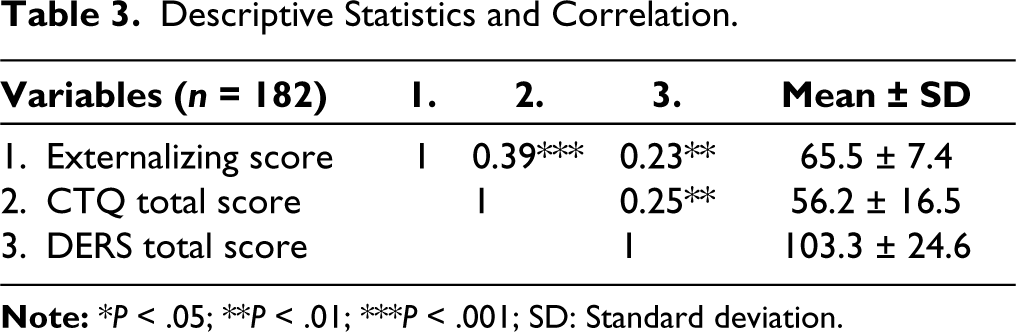
The results presented in Table 3 highlight the descriptive statistics and correlation coefficients among the variables for the study’s participants (n = 182). The mean ± standard deviation values for each variable are provided. The mean externalizing score was 65.5 ± 7.4. This variable exhibited statistically significant positive correlations with both the CTQ total score (r = 0.39, P < .001) and the DERS total score (r = 0.23, P < .01). The mean CTQ total score was 56.2 ± 16.5. A statistically significant positive correlation was found between the CTQ total score and the DERS total score (r = 0.25, P < .01). The mean DERS total score was 103.3 ± 24.6. Significant correlation coefficients suggest that higher externalizing scores were associated with higher levels of childhood trauma (as indicated by the CTQ total score) and greater difficulties in emotion regulation (as indicated by the DERS total score). Additionally, the positive correlation between the CTQ total score and the DERS total score suggests that higher levels of childhood trauma were linked with more challenges in emotion regulation.
Descriptive Statistics and Correlation.
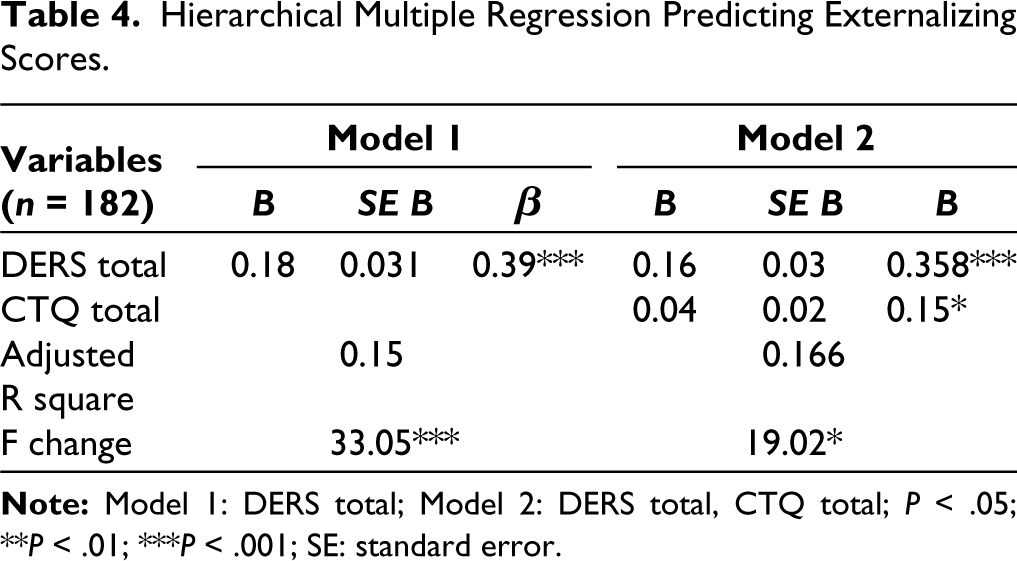
The results presented in Table 4 showcase the outcomes of hierarchical multiple regression analyses aimed at predicting externalizing scores among the study participants (n = 182). In Model 1, the inclusion of the DERS total score as the predictor yielded significant results. Specifically, a positive relationship was observed between DERS total and externalizing scores, where a higher DERS total score (B = 0.18, standard error [SE] = 0.031, β = 0.39, P < .001) corresponded to increased externalizing symptomatology. In Model 2, which incorporated both DERS total and CTQ total as predictors, DERS total retained its significant positive association with externalizing scores (B = 0.16, SE = 0.03, β = 0.358, P < .001). Additionally, CTQ total exhibited a positive but relatively weaker relationship with externalizing scores (B = 0.04, SE = 0.02, β = 0.15, P < .05). The adjusted R-squared increased from 0.15 in Model 1 to 0.166 in Model 2, indicating that the inclusion of CTQ total in Model 2 accounted for an additional portion of the variance in externalizing scores. The F change statistic was significant for both Model 1 (F = 33.05, P < .001) and Model 2 (F = 19.02, P < .05), suggesting that the predictors collectively contributed significantly to the prediction of externalizing scores. Overall, these findings highlight the substantial influence of difficulties in emotion regulation, as well as the supplementary role of childhood trauma, on the manifestation of externalizing symptoms among the studied adolescents. These findings suggest that DERS might be a significant mediator in the relationships of CTQ with externalizing scores.
Hierarchical Multiple Regression Predicting Externalizing Scores.
To confirm the mediating role of emotional regulation, we conducted mediation analysis using Hayes Process Macros 14 for the R statistical package 13 with an indirect bootstrapping approach with 5000 sampling iterations and a 95% confidence interval (CI). We calculated the P value for indirect mediation using a separate calculator. 15
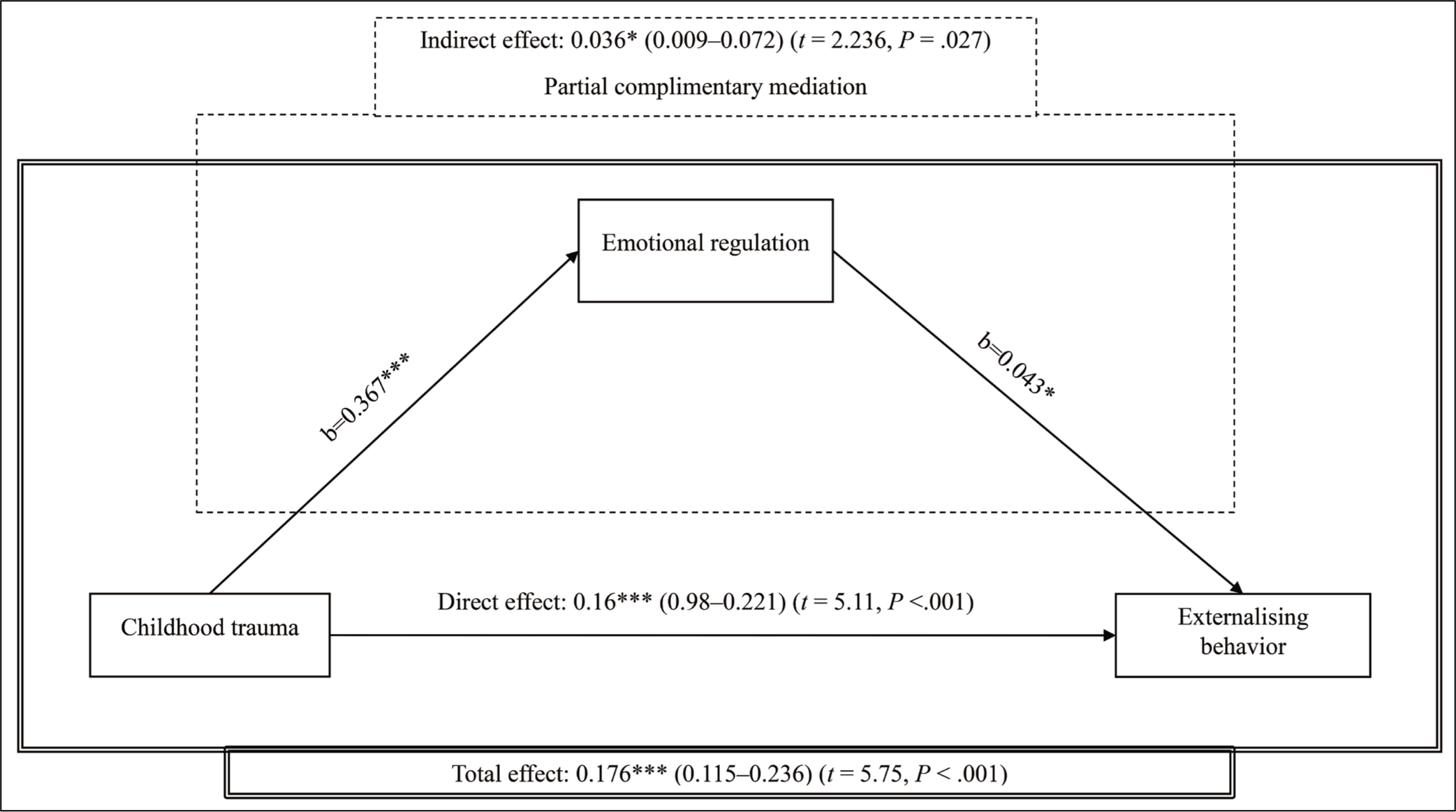
The results of the mediation analysis are summarized in Figure 2. In the mediation analysis model, the investigation of the relationship between childhood trauma scores and externalizing scores revealed compelling results. The total effect of childhood trauma scores on externalizing scores was observed to be statistically significant (B = 0.176, 95% CI = 0.115–0.236, t = 5.75, P < .001), indicating a direct influence of childhood trauma experiences on the manifestation of externalizing symptoms. Notably, even when DERS was introduced as a mediator in the analysis, childhood trauma continued to maintain a significant direct effect on externalizing scores (B = 0.16, 95% CI = 0.98–0.221, t = 5.11, P < .001). Importantly, the indirect effect mediated by DERS was also found to be significant (B = 0.036, 95% CI = 0.009–0.0723, t = 2.236, P = .0273). This implies that the relationship between childhood trauma scores and externalizing scores is not only directly influenced by the traumatic experiences but is also partially mediated by the difficulties in emotion regulation as assessed by the DERS. These findings suggest that difficulties in emotion regulation play a significant role in partially mediating the relationship of childhood trauma scores with externalizing scores. This mediation is complementary 16 rather than competitive, that is, both the direct and the indirect effects are significant and cause a change in the same direction.
Mediation Model with Emotional Regulation as Mediator for Childhood Trauma (*P < .05; ***P < .001).
Discussion
This study sought to unravel the intricate interplay between childhood trauma, emotional regulation, and externalizing symptoms among adolescents aged 13 to 19 years. Through a comprehensive methodology involving purposive sampling, rigorous assessment tools, and robust statistical analyses, this research contributes valuable insights into the psychological dynamics that underlie externalizing behaviors. The findings underscore the significance of both childhood trauma and emotional regulation difficulties in shaping the manifestation of externalizing symptoms. Mediating role of emotional regulation is substantiated in the study.
The observed sociodemographic characteristics of the participants provide a contextual backdrop to the study’s outcomes. The diversity in age, gender, education, family income, and living arrangements represents the heterogeneous nature of the adolescent group, enhancing the generalizability of the study’s outcomes. In our sample, the prevalence of EA and EN was high. In a systematic review, it was concluded that school-aged children experiencing neglect or EA may exhibit externalizing features and poor academic performance. 17 Previous research provides evidence that the prevalence of childhood maltreatment has a range of negative consequences that begin in childhood or adolescents and often last through adulthood with the presence of psychiatric history.18–20 Literature points towards trauma may precede psychiatric symptoms as well as strong association between childhood maltreatment and adult psychopathology.21,22 Our study signifies the pertinence of exploring these variables within this population. The prevalence of trauma and its association with development of psychopathology in the form of externalizing symptoms in our sample adds to the existing literature.
The correlation results reveal compelling patterns. The positive correlations between childhood trauma, emotional regulation difficulties, and externalizing symptoms illuminate their intertwined nature. Adolescents who experienced higher levels of childhood trauma were more likely to exhibit externalizing behaviors, and these behaviors were concurrently associated with greater difficulties in emotion regulation. It was observed in a five-year community-based cohort of adolescents that emotional reactivity and maladaptive responses to distress mediated the association between child maltreatment and both internalizing and externalizing psychopathology. 23 Literature also suggests that childhood maltreatment is a risk for developing externalizing psychopathology in children through disruptions in emotion regulation as the mechanism.24-27 A study interested in tracking longitudinal pathway linkages between child maltreatment, emotional regulation, and psychopathology found the important role of emotion regulation as a risk or a protective mechanism in the link between earlier child maltreatment and later psychopathology through its influences on peer relations. 28
Hierarchical multiple regression examined and unveiled a multi-layered relationship between emotional regulation, childhood trauma, and externalizing symptoms. Difficulties in emotional regulation emerged as a robust predictor of externalizing behaviors. 29 Empirical research broadly supports this position that poorer emotion regulation capacities were longitudinally associated with externalizing difficulties. Interestingly, the inclusion of childhood trauma as an additional predictor did not diminish the impact of emotional regulation difficulties but rather augmented the predictive capacity of the model. Childhood trauma also exhibited a direct but relatively weaker association with externalizing symptoms, underscoring its role as a contributing factor. Research tells that affective dysregulation can be mitigated by safe attachments, secure meaning schemas 30 ; however, in the presence of childhood trauma like EA or EN or parental violence the safe attachments are thwarted and result in difficulties in emotional regulation which can in turn lead to the development of psychopathologies.
The mediation analysis provided a nuanced understanding of the mechanisms underlying the observed relationships. The significant direct effect of childhood trauma on externalizing symptoms underscores the enduring impact of early adverse experiences on behavioral outcomes. 31 Importantly, the significant indirect effect through emotional regulation difficulties highlights the role of emotional regulation as a mediator in the relationship between childhood trauma and externalizing behaviors. This finding signifies that, while childhood trauma exerts a direct influence on externalizing symptoms, it also operates through emotional regulation difficulties, further amplifying the understanding of the pathways through which childhood trauma manifests in psychopathology. A developmental perspective on externalizing spectrum disorders offers that age-expected gains in emotion regulation are not achieved by children who are reared under conditions of adversity. 32
The implications of these findings are pivotal for clinical practice and intervention strategies. Recognizing the complex interplay between childhood trauma, emotional regulation, and externalizing symptoms, mental health professionals must adopt comprehensive assessment approaches that address both trauma history and emotional regulation capacities. Early identification and targeted interventions for emotional regulation skills may serve as preventive measures, mitigating the risk of externalizing behaviors among adolescents. Emotional regulation can prove to be beneficial in managing externalizing behavior evidenced by literature such as emotion regulation training has a positive impact on the adaptive emotion regulation strategies of adolescents with externalizing problems. 33
Integrating evidence-based interventions that enhance emotional regulation skills, such as cognitive–behavioral therapy (CBT) and dialectical behavior therapy (DBT), into clinical practices can potentially alleviate the impact of childhood trauma and its associated externalizing symptoms. 34 A meta-analysis demonstrated the effectiveness of CBT in children and adolescents with externalizing disorders and showed that substantial effects can be obtained in routine care across different formats (i.e., individual or group), with varying degrees of parental involvement. 35 Furthermore, implementing trauma-informed care models, which emphasize safety, empowerment, and trust, could prove beneficial in providing a supportive environment for trauma survivors while concurrently addressing emotional regulation challenges. 36 A focus on emotion regulation strategies has the potential to optimize treatment for trauma outcomes in externalizing disorders.
While this study advances our understanding of the relationships under investigation, several limitations warrant consideration. The cross-sectional design hampers the establishment of causal relationships among variables. Longitudinal studies could provide insights into the temporal dynamics of these associations. The reliance on self-report measures might introduce bias and shared method variance. Future research could incorporate multi-informant and multi-method assessments. The study’s focus on a specific clinical population and a particular geographical area might limit the generalizability of the findings. Additionally, the exclusion of adolescents with severe mental illnesses may have influenced the observed relationships. Type and severity of trauma can influence psychopathology which was not focused on the current research. Influence of protective factors like healthy parenting, resilience which could influence emotion regulation is not considered. Furthermore, the influence of protective factors, such as healthy parenting and resilience, which can play a significant role in shaping emotion regulation, was not considered.
In conclusion, this study emphasizes the pivotal role of emotional regulation in shaping the relationship between childhood trauma and externalizing symptoms. These findings hold crucial implications for clinical interventions that seek to alleviate the impact of trauma and facilitate emotional regulation skills, ultimately fostering better mental health outcomes for adolescents grappling with externalizing psychopathology. Adolescence is an age marked with emotional difficulties and in presence of trauma the coping resources and emotional capacities might be challenged; thus, it is important to take into consideration any presence of trauma of any kind for understanding the emotional challenges and help the adolescents build age-appropriate emotional skills. Emotion regulation is a transdiagnostic concept and therapies focusing on enhancing these skills can be beneficial across disorders.
Footnotes
Declaration of Conflict of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
The study was accorded Ethical Committee Approval vide Ethics Committee of Institute of Human Behaviour and Allied Sciences 2022/5/14/V-2 dated 9-6-2022. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki. Written Informed Consent was taken from all the participants.