
Abstract
Background:
The coronavirus disease 2019 pandemic represents an unprecedented traumatic stressor to mental health. Psychological distress is considered a reliable proxy for psychopathology and can be negatively influenced by childhood trauma through sensitization effects. Emotion dysregulation has been proposed as a potential mediator of this mechanism. We aimed to test this hypothesis in a national Italian sample assessed in the early phase of the coronavirus disease 2019 outbreak.
Methods:
We investigated the relationship between psychological distress and childhood trauma in 500 healthy participants assessed through a survey-based study, after the coronavirus disease 2019 pandemic lockdown in Italy. Levels of psychological distress and history of childhood trauma were obtained using the Kessler-10 (K10) and the Childhood Trauma Questionnaire, respectively. We used bootstrapped mediation analysis to test the mediator role of emotional dysregulation, measured through the Difficulties in Emotion Regulation Scale, on the effect of childhood trauma on psychological distress.
Results:
In total, 190 (38%) reported psychological distress related to the coronavirus disease 2019 outbreak. Individuals with psychological distress experienced more childhood trauma, specifically emotional abuse (F = 23.51, df = 1, p < 0.001) and neglect (F = 10.98, df = 1, p = 0.001). After modelling the effect of emotional dysregulation, the impact of childhood trauma on coronavirus disease 2019-related psychological distress resulted in indirect effects and mediated by deficits in emotion regulation mechanisms (bootstrapped lower level of confidence interval = 0.345, upper level of confidence interval = 0.598).
Conclusion:
Childhood trauma is associated with increased vulnerability to the stressful effect of the coronavirus disease 2019 outbreak. Our data suggest that emotional dysregulation may represent a dimension mediating the impact of childhood trauma on coronavirus disease 2019-related psychological distress and may be considered as specific target for interventions aiming at empowering resilience.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic represents an overwhelming stressor to mental health across the globe and will need timely interventions (Fiorillo and Gorwood, 2020; Moser et al., 2020; Sani et al., 2020; Xiang et al., 2020). Italy, particularly, was the first European country to face the COVID-19 emergency and to announce a nationwide lockdown that began on 9 March 2020 after an increase in total deaths of nearly 100% in the 48 hours before the restrictions (Lazzerini and Putoto, 2020). Previous data on collective adverse events showed that, unlike physical injuries, negative mental health outcomes may not be immediately apparent (North and Pfefferbaum, 2013). Individuals exposed to collective trauma may subsequently experience new-onset trauma-related psychiatric disorders, exacerbations of pre-existing psychopathology and/or psychological distress (Bell et al., 2019; North and Pfefferbaum, 2013).
Psychological distress, measured through specific instruments, is considered a reliable proxy for mental health status and a screener to determine whether clinical assessment or intervention needs to be addressed (Kessler et al., 2002). It has been used in community surveys since the end of World War II as a first-stage psychiatric screen, and thereafter largely adopted in national health surveys to assess severity of dimensional psychological symptoms (Nishi et al., 2018; Sunderland et al., 2011).
Among early stressors, childhood trauma (CT) has emerged as one of the most important risk factors for psychiatric disorders (Copeland et al., 2018; Hailes and Yu, 2020), including mood, anxiety and post-traumatic stress disorders (PTSD) (Janiri et al., 2019; Lewis et al., 2019). Early adverse events have been associated with increased suicide risk (Janiri et al., 2018; 2020a; O’Neill and O’Connor, 2020), negative psychosocial/functional outcomes and physical health conditions (Copeland et al., 2018; Hailes and Yu, 2020; Pandey et al., 2020). Distinct types of traumatic experiences (i.e. sexual, physical, emotional abuse and neglect) differently impact on multiple psychiatric disorders, modulating independently their clinical expression (Hailes and Yu, 2020). CT may also exacerbate negative responses to subsequent traumatic events. Specifically, previous national surveys reported a ‘sensitisation effect’ of CT on collective traumas, such as a pandemic, pointing out that childhood exposure correlates with worse outcomes (Breslau et al., 1998; Garfin et al., 2020).
Emotion dysregulation is defined by difficulties in several areas, including the ability to monitor and evaluate emotional experiences, modulate their intensity or duration, and adaptively manage emotional reactions in order to meet situational demands (Gratz and Roemer, 2004). Abnormalities in emotion regulation are implicated in response to trauma and have been linked to many psychiatric disorders (Sheppes et al., 2015). CT exposure may influence emotion regulation mechanisms (Chu et al., 2019; Dunn et al., 2018). Accordingly, recent studies proposed emotion dysregulation as a psychological dimension mediating the association between early traumatic experiences and the risk of psychiatric symptoms in adulthood (Aas et al., 2017; Janiri et al., 2020b; McLaughlin et al., 2020).
In the light of the observations set out above, we decided to test whether there is a specific relationship between CT and the psychological distress related to COVID-19, and whether different types of past traumatic experiences differently contribute to this relationship. Furthermore, we sought to tackle the issue of whether the effect of CT on psychological distress is mediated by emotional dysregulation.
To test these hypotheses, we used data from 500 healthy participants assessed in the early phase of the COVID-19 outbreak in Italy.
Methods
Participants
The study was conducted through an online survey, starting on 10 April 2020 and ending on 13 April 2020. This time-line was chosen in order to assess participants’ response during an early phase of the COVID-19 outbreak, after Italy lockdown following the government decree of 9 March 2020, and the World Health Organization (WHO) characterization of COVID-19 as a pandemic (11 March 2020). During this period, the total COVID-19 confirmed cases and deaths were 147,577 and 18,849, respectively (Italian Civil Department). The snowball sampling method was employed to recruit participants (Coleman, 1958; Goodman, 1961). An initial subset of invitees (five participants) was selected in order to ensure broad representation of age, gender, occupation, education level and geographic location. This subset of participants then forwarded the questionnaire to five referrals whom they considered suitable for the survey. This second subset forwarded the survey in the same way and so on, until data saturation. The survey was anonymous, and confidentiality of information was assured. To motivate study participation, a detailed explanation of study purpose, including the need to carry out research in order to prevent and treat the psychological burden that could emerge amid the COVID-19 pandemic, was provided to participants before they started survey completion. Participants aged 18–75 years, living in Italy for at least 4 weeks from February 2020, with adequate command over written and spoken Italian language, and with at least 5 years of education, were eligible for the study. Respondents were excluded if they were non-Italian language speakers, were currently hospitalized, reported a history of mental disorder and/or could not complete the online survey independently. The study followed the European Survey Research Association (ESRA) guidelines. All participants completed the questionnaire online via EUSurvey. The study was approved by the Agostino Gemelli University Hospital Foundation IRCCS-Catholic University of the Sacred Heart of Rome Ethics Committee and was undertaken in accordance with the Principles of Human Rights, as adopted by the World Medical Association at the 18th WMA General Assembly, Helsinki, Finland, June 1964 and subsequently amended at the 64th WMA General Assembly, Fortaleza, Brazil, October 2013. A total of 544 individuals responded to the survey, of which 500 were included in the final sample. Previous sensitivity analysis (Faul et al., 2007) suggested that with N = 500 the power was = 0.90 to detect a minimally interesting effect size of δ = 0.2 (α = 0.05; two-tailed).
Assessment
A dedicated, self-report questionnaire was adopted to collect main demographic and epidemiological characteristics (age, gender, educational level, occupation, marital status, geographic location), medical variables (lifetime history of chronic diseases, family history of psychiatric disorders) and information on lockdown conditions (living alone, living close to the family, change in working activities, working on frontline and having had direct contact with confirmed cases).
Psychological distress
We employed the Kessler 10 Psychological Distress Scale (K10) (Kessler et al., 2002) to assess the psychological impact of the COVID-19 outbreak. K10 is a 10-item questionnaire intended to yield a global measure of distress based on questions about anxiety and depressive symptoms experienced during the most recent 4-week period. Items are rated using a 5-point Likert-type scale ranging from 1 (never) to 5 (always). Score may range from 10 to 50. Low scores indicate low levels of psychological distress, whereas high scores indicate high levels of psychological distress. Consistent with previous validation studies (Andrews and Slade, 2001; Kessler et al., 2003), we adopted the cut-off score of > 19 to detect the likelihood of presence of psychological distress. The psychometric reliability of K10 makes it attractive for use in general-purpose health surveys (Kessler et al., 2002).
CT
We used the short form of the Childhood Trauma Questionnaire (CTQ) to measure adverse childhood events. This is a 28-item, retrospective, self-report questionnaire (Bernstein et al., 2003) that investigates traumatic experiences in childhood; there are five possible answers, which range from ‘never true’ to ‘very often true’ depending on the frequency of the events. The questionnaire assesses five types of trauma: emotional abuse, emotional neglect, physical abuse, physical neglect and sexual abuse. For each type of trauma, scores range from 5 to 25. Higher scores indicate greater childhood mistreatment. The CTQ has been used in both non-clinical (Bernstein et al., 1994) and clinical populations (Crosta et al., 2018; Janiri et al., 2019) and it has a high degree of reliability (Bernstein et al., 1994).
Emotional dysregulation
To assess deficits in emotion regulation, we used the Difficulties in Emotion Regulation Scale (DERS) (Gratz and Roemer, 2004), a 36-item self-report measure that assesses individuals’ typical levels of emotion dysregulation. Participants rate each item using a 5-point Likert-type scale (1 = almost never, 5 = almost always). Higher scores indicate greater difficulties regulating emotions. In prior studies, the DERS has demonstrated convergent validity with other established measures of emotion dysregulation, good test–retest reliability, excellent internal consistency and adequate predictive validity of several behavioural outcomes associated with emotion dysregulation (Gratz and Roemer, 2004).
Statistical analyses
We compared individuals with and without psychological distress related to the COVID-19 outbreak (COVID-19 STRESS group; COVID-19 NO-STRESS group) on demographic and epidemiological characteristics, medical variables and information on lockdown conditions on the basis of the chi-square test.
Distribution patterns of CT
For the first aims of this study, we focused on the distribution patterns of CT in COVID-19 STRESS group and in the COVID-19 NO-STRESS group. Therefore, we conducted a multivariate analysis of covariance (MANCOVA) using all the CT subtypes as dependent variables and the COVID-19 STRESS groups as independent factor, and age and sex as covariates. When the initial model was significant, we conducted a series of one-way analysis of covariance (ANCOVA) to test differences between groups on dependent variables with the same covariates. We used a statistical model corrected for multiple comparisons according to the Bonferroni procedure (p < 0.05/number of comparisons) to minimize the likelihood of type I statistical errors.
Mediation analysis
To test whether the correlations between CT subtypes and psychological distress total score are mediated by emotional dysregulation, we used the PROCESS macro for SPSS for mediation analyses (Hayes, 2013). Mediation implies a situation where the effect of the independent variable on the dependent variable can best be explained using a mediator variable that is caused by the independent variable and is itself a cause for the dependent variable. This means that instead of X (CT subtype) causing Y (psychological distress) directly, X is causing the mediator M (emotional dysregulation), and M, in turn, is causing Y. The causal relationship between X and Y in this case is said to be indirect rather than direct and the mediation model can be considered a full mediation model. The relationships between the independent variable, the mediator and the dependent variable are depicted in the form of a path diagram/model. For each path, the regression coefficients (betas) indicating the direction and magnitude of the effect of one variable on the other are shown. Mediation analyses were tested using a very conservative bootstrapping resampling procedure with bias-corrected confidence estimates. Bootstrapping is a strongly recommended process that treats the original sample as the population and resamples (with replacement) observations from within that sample thousands of times over in order to generate sample-based estimates of indirect effects and their standard errors (Holland et al., 2017). The 95% confidence interval of the direct and indirect effects was obtained with 10,000 bootstrap samples. Direct and indirect effects are significant if confidence intervals do not contain a zero value. A p value < 0.01 has been defined as significant. Additional analyses were undertaken to examine the effect of sex on the mediation model and are reported in the Supplementary material. All statistical analyses were performed using SPSS v. 25 (IBM Corp., USA).
Results
A total of 500 individuals were included in the study. Demographic and epidemiological characteristics, medical characteristics and information on lockdown conditions are reported in Table 1.
Characteristics of the sample (n = 500).
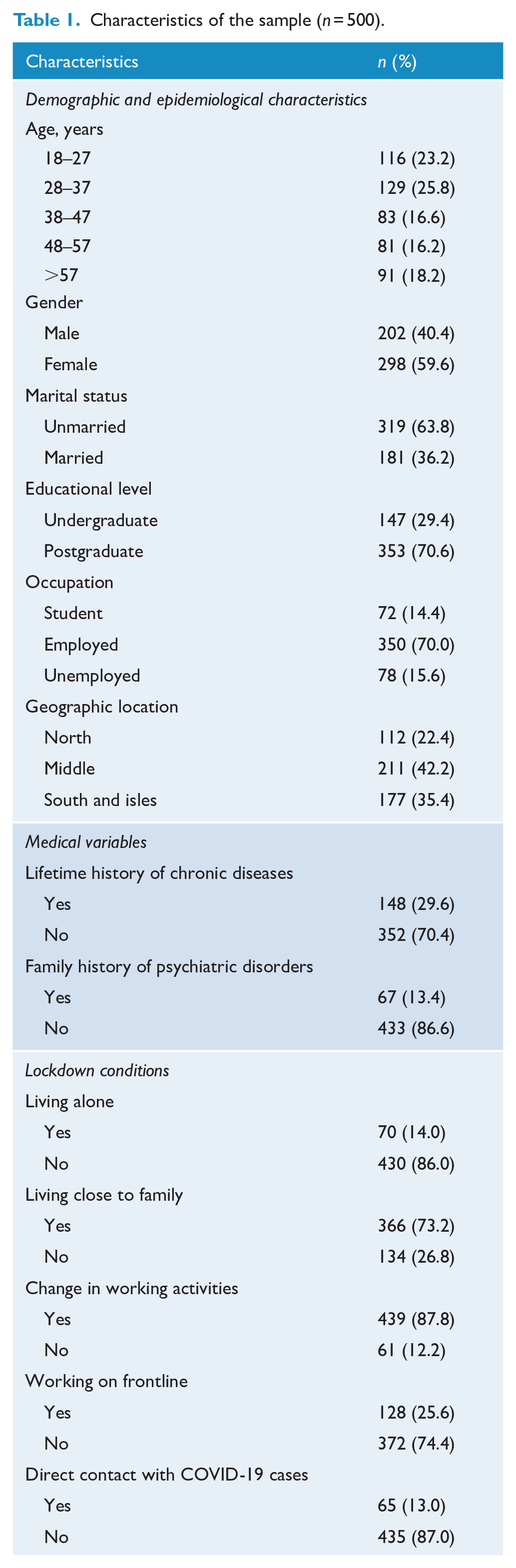
A total of 190 individuals (38%) reported psychological distress related to the COVID-19 outbreak. Individuals with and without psychological distress differ in sex (χ2 = 6.67, df = 1, p = 0.01), age (χ2 = 19.08, df = 4, p = 0.001) and marital status (χ2 = 5.10, df = 1, p = 0.02). Specifically, in the COVID-19 STRESS group, most participants were women (n = 127, 66.8%), were aged 28–37 (n = 58, 30.5%) and were unmarried (n = 133, 70%). The two groups did not differ for medical variables and information on lockdown conditions (further details in Supplementary material, Table S1).
Distribution patterns of CT
The MANCOVA, after controlling for age and sex, indicated a significant global effect (Wilks’ Lambda = 0.94, F = 5.49, df = 5, p < 0.001) of CT experiences on the two groups (COVID-19 STRESS; COVID-19 NO-STRESS). In particular, a series of ANCOVAs clarified that the COVID-19 STRESS group significantly reported more childhood traumatic experience than the COVID-19 NO-STRESS group with respect to emotional abuse and emotional neglect (Table 2).
Distribution patterns of childhood trauma subtypes in COVID-19 Stress group (n = 190) and COVID-19 No-Stress group (n = 310).
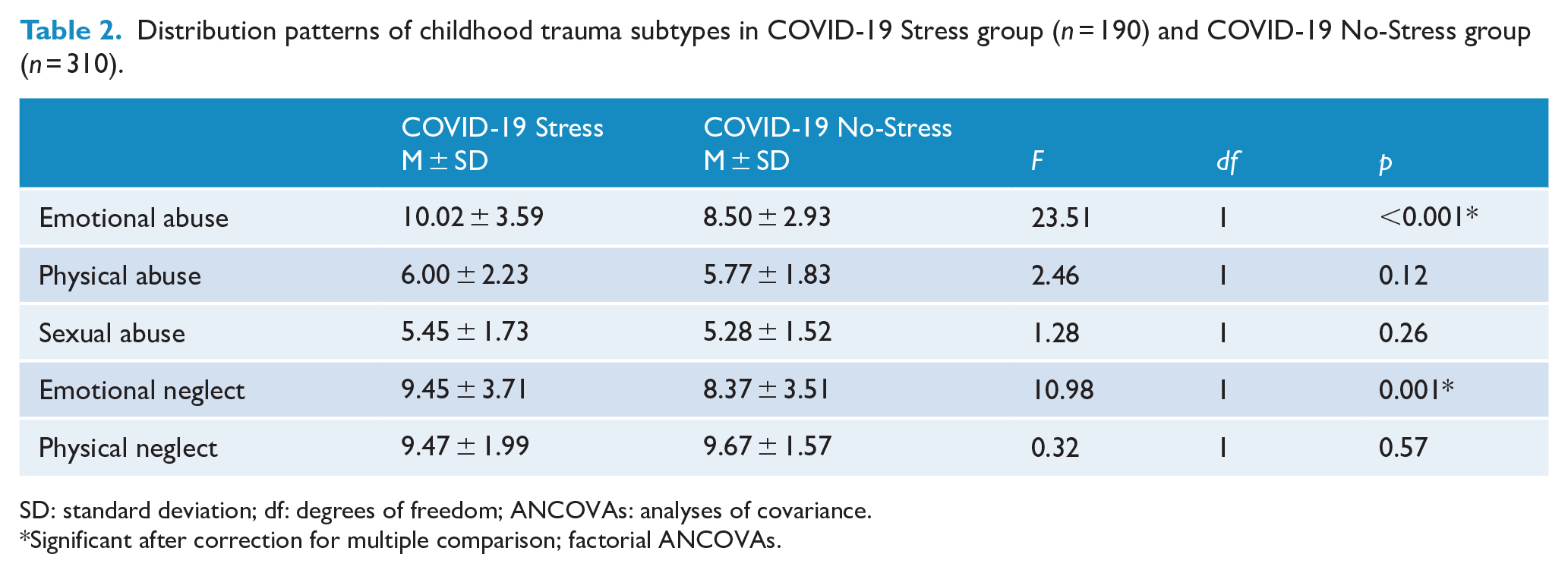
SD: standard deviation; df: degrees of freedom; ANCOVAs: analyses of covariance.
Significant after correction for multiple comparison; factorial ANCOVAs.
Mediation analysis
For the mediation analysis, we focused on the association between emotional abuse/neglect and psychological distress related to the COVID-19 outbreak. Because no association was observed between sexual abuse, physical abuse/neglect and psychological distress, no mediation model was required (see Supplementary material, Table S2).
Regarding the relationship between emotional abuse and COVID-19-related psychological distress, we found that emotional abuse was positively related to emotional dysregulation, which in turn was positively related to psychological distress (Figure 1). Under the bootstrapped 95% confidence interval, the significant indirect effect was 0.465 and did not contain 0 (lower level of confidence interval [LLCI] = 0.345, upper level of confidence interval [ULCI] = 0.598). Conversely, we found no significant direct effect of emotional abuse on COVID-19-related psychological distress (LLCI = −0.34, ULCI = 0.24). Therefore, we observed that the causal relationship between emotional abuse and COVID-19-related psychological distress was indirect, rather than direct, and the model could be considered a full mediation model.
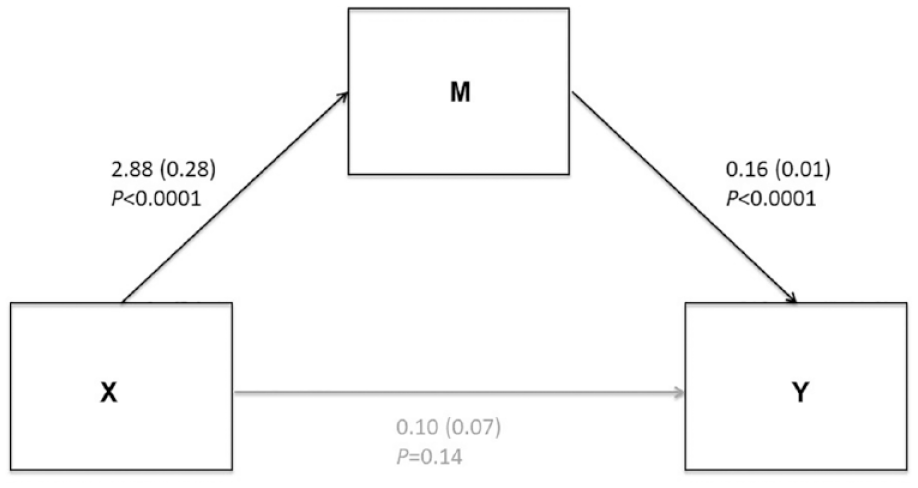
The indirect effect of Emotional abuse on COVID-19-related psychological distress.
Similarly, we found a full mediation model explaining the indirect relationship between emotional neglect and COVID-19-related psychological distress. Emotional neglect was positively related to emotional dysregulation, which in turn was positively related to psychological distress (Figure 2). Under the bootstrapped 95% confidence interval, the significant indirect effect was 0.348 and did not contain 0 (LLCI = 0.247, ULCI = 0.464). Conversely, we found no significant direct effect of emotional abuse on COVID-19-related psychological distress (LLCI = −0.118, ULCI = 0.122).
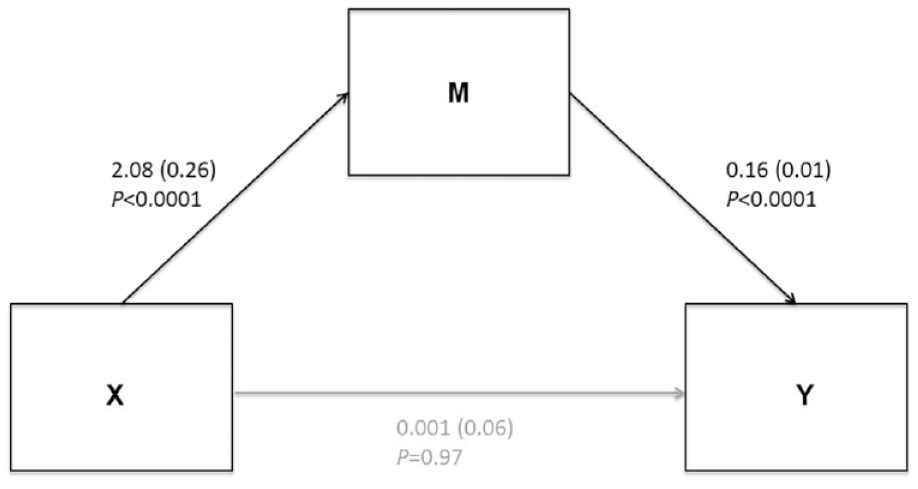
The indirect effect of Emotional neglect on COVID-19-related psychological distress.
Additional analyses confirmed the same model in men and women (see Supplementary material, Figures S1 and S2).
Discussion
To our knowledge, this is the first study to date to investigate CT as a risk factor for the psychological distress related to the COVID-19 pandemic. Participants were assessed in Italy in the early phase of the COVID-19 outbreak when the total COVID-19 confirmed cases and deaths exceeded 147,577 and 18,849, respectively (Italian Civil Department). The key findings were that around 38 in every 100 participants reported a form of psychological distress; the same group of individuals experienced more childhood traumatic events, specifically emotional abuse and neglect. Moreover, after modelling the effect of emotional dysregulation, the impact of CT on psychological distress resulted in indirect effects and mediated by difficulties in emotion regulation mechanisms.
The results provide additional support for societal concerns of stressful impact of the COVID-19 pandemic on mental health (Moser et al., 2020; Sani et al., 2020; Xiang et al., 2020). The rates of psychological distress observed in this study are comparable with those recently found in other samples assessed through the K10 (Ben-Ezra et al., 2020; Li et al., 2020; Moccia et al., 2020). Sex rates are also in line with meta-analytic evidences, showing higher rates of distress in females compared to males (Luo et al., 2020; Pappa et al., 2020).
Our study highlights that CT was more frequent in participants reporting COVID-19-related psychological distress. The link between CT and negative mental health outcome is well documented (Copeland et al., 2018; Hailes and Yu, 2020; Lewis et al., 2019). A recent prospective, population-based cohort study specified that CT exposure was associated with higher risk of adult psychiatric disorders (odds ratio for any disorder, 1.2; 95% CI = [1.0, 1.4]) and poorer functional outcomes (Copeland et al., 2018). Moreover, large population studies identified CT as a specific risk factor for suicidal thoughts and behaviours (Janiri et al., 2020a; O’Neill and O’Connor, 2020). This could be potentially relevant, because, although there are still no data available on COVID-19 and suicide, objective social isolation and subjective feelings of loneliness are associated with a higher risk of suicide (Sani et al., 2020).
The relationship we found between CT and COVID-19-related psychological distress could be explained by the ‘sensitization effects’. Seminal contributions suggested that exposure to CT increases vulnerability to the effects of later stressful life events (Heim and Nemeroff, 2001; Koenen et al., 2007; McLaughlin et al., 2010). Data from large populations-based samples (McLaughlin et al., 2010) and longitudinal cohorts (Koenen et al., 2007) specified that CT may sensitize individuals to psychopathology by lowering their tolerance to subsequent stressors. This hypothesis has been explored in national surveys on collective traumas, demonstrating that previous stressors may sensitize people to an exogenous event like a salient collective trauma (Breslau et al., 1998; Garfin et al., 2020). An extensive literature has developed over time on the association between CT exposure and chronic dysregulation of the physiological stress response system (Heim and Nemeroff, 2001; Schalinski et al., 2019). Alterations in hypothalamic–pituitary–adrenal (HPA) axis mechanisms, in cortisol response to an acute stressor and in total cortisol production have been observed among adults with a history of CT (Heim and Nemeroff, 2001; Schalinski et al., 2019). According to the stress sensitization hypothesis, early life trauma altered the regulation of these stress-sensitive systems, leading to an in increased impact of subsequent exposures (Heim and Nemeroff, 2001).
Although the exact pathways linking CT to later stress vulnerability remain to be identified, in this study we clarified that the impact of CT on COVID-19-related psychological distress is indirect and mediated by alterations in emotion regulation. Specifically, we found that emotional abuse/neglect was positively related to emotional dysregulation, which in turn was related to psychological distress. The first part of the path (Figures 1 and 2) is in line with previous findings showing that CT is one of the primary determinants of emotion dysregulation (Chu et al., 2019; Dunn et al., 2018). Consistent with this framework, a recent study pointed out that early life stress events may shape emotion regulation mechanisms through an interaction with abnormalities in HPA axis (Hartling et al., 2019). Moreover, neurobiological findings showed a specific effect of CT on brain structures that are primarily implicated in emotion regulations (Janiri et al., 2019; Malhi et al., 2019a, 2019b, 2020a). The second part of the path (Figures 1 and 2) matches a considerable body of literature on the relationship between emotional dysregulation and negative mental health outcome (Sheppes et al., 2015). Deficits in affect regulation have also been observed in healthy individuals at risk for psychopathology and could influence the development of psychiatric symptoms in the context of negative life events (Malhi et al., 2020b; Sheppes et al., 2015). Taken together, these observations highlight the importance of emotional trauma (abuse or neglect) that can influence the capacity to regulate affects induced by subsequent stressful events. Furthermore, in our study, we found that individuals reporting or not COVID-19-related psychological distress differed in emotional abuse and neglect rather than in other subtypes of CT. This could be potentially explained by the specific impact of ineffective emotion regulation strategies on psychological distress that could, in turn, be more likely linked with early emotional trauma (abuse or neglect) rather than other types of CT.
Before presenting our conclusions, we must acknowledge some issues that might limit the generalizability of our results. First, the study has a cross-section design and lacks longitudinal follow-up. Because of the increasingly distressing situation, the mental health impact of the COVID-19 outbreak on the Italian general population could change during time. Therefore, long-term psychological implications of this population warrant further investigation. Second, the survey design involved online invitation rather than face-to-face random sampling. As a consequence, the condition of the population who cannot use network devices remains unexplored. Third, it was not possible to assess the participation rate since it is unclear how many subjects received the link for the survey. Fourth, the snowballing sampling strategy does not involve a random selection of the sample but rather a non-probabilistic procedure, so that participants’ suitability may not be controlled for once sample increases in size. Furthermore, the sampling procedure could not rule out motivational bias, according to which individuals who are more distressed may also be more likely to engage in the study. Finally, the reliability of the retrospective assessment of CT experiences, as assessed with the CTQ during adulthood, may be influenced by uncontrolled recall bias. Nevertheless, the CTQ is largely used and it is indicated as one of the best instruments for evaluating early stress events (Bernstein et al., 1994). Moreover, we did not find any significant relationship between severity of CT experiences and demographic characteristics considered as potential recall bias (further details in Supplementary material).
In conclusion, as the authors note earlier, more work is necessary to clarify risk factors associated with mental health negative outcomes related to the COVID-19 outbreak. Nevertheless, this study sets the foundation for future analyses using data from the Italian population. The findings reported have immediate and practical implications, as the indirect effect of CT on psychological distress is actionable and modifiable through specific interventions on emotion regulation mechanisms (Fava et al., 2016). Systematic approach to risk factors and case identification of COVID-19-related stress disorders is required. Interventions or policies aimed at empowering emotion regulation and resilience may have multifaceted effects on health and well-being during the COVID-19 pandemic (Fava et al., 2016).
Supplemental Material
sj-pdf-1-anp-10.1177_0004867421998802 – Supplemental material for Emotional dysregulation mediates the impact of childhood trauma on psychological distress: First Italian data during the early phase of COVID-19 outbreak
Supplemental material, sj-pdf-1-anp-10.1177_0004867421998802 for Emotional dysregulation mediates the impact of childhood trauma on psychological distress: First Italian data during the early phase of COVID-19 outbreak by Delfina Janiri, Lorenzo Moccia, Luigi Dattoli, Maria Pepe, Marzia Molinaro, Valentina De Martin, Daniela Chieffo, Marco Di Nicola, Andrea Fiorillo, Luigi Janiri and Gabriele Sani in Australian & New Zealand Journal of Psychiatry
Footnotes
Acknowledgements
We express our gratitude to all participants who contributed their time and effort to participate in this study during this difficult time.
Author Contributions
All authors conceived and designed the analyses. D.J., L.M., L.J., M.D. and G.S. did the analyses and drafted the output. All authors interpreted the data. A.F., L.D., M.P., M.M., V.D. and D.C. critiqued the output and contributed important intellectual content. All authors have read and approved the final version of the manuscript. G.S. serves as guarantor for the content of this paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
All participants provided their online informed consent. The study was approved by the local ethics committee on human research.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.