
Abstract
Background:
Children in India who have been diagnosed with celiac disease deal with a variety of challenges and difficulties as a result of their condition. Understanding their experiences is important to help the patients adapt better to the demands of celiac disease and gluten-free diet.
Methods:
The present study has used a constructivism paradigm as a study design. Participants were recruited through purposive sampling. In-depth telephonic interviews were conducted with 10 children with celiac disease. Thematic analysis was used to analyze the interview data.
Results:
The main themes and sub-themes that emerged from the data were emotional responses (the feeling of deprivation, the feeling of being different from others, the novelty of gluten-free diet leading to excitement), physical health impact (getting tired easily, delayed growth), social constraints (social limitations brought on by celiac disease, peer pressure to eat gluten, and non-acceptance of celiac disease by others), future concerns (uncertainty about the future, improved physical health, celiac disease cure, dependency on others), navigating dietary changes (fear of cross-contamination, food restrictions caused by celiac disease, non-availability of gluten-free food, and limited food options outside the home), coping strategies, and management of celiac disease (eat home-cooked meals, receiving support from family, and friends, adhering to gluten-free diet).
Conclusion:
Governmental organizations and experts in mental health must acknowledge the needs of Indian children with celiac disease. The need of the hour is to improve gluten-free product labelling and raise awareness of celiac disease.
Introduction
Children face different challenges and issues after the diagnosis of an illness. The challenges faced by children after the diagnosis of celiac disease (CD) are well understood in the Western context, but in the Indian context, there is a scarcity of research to understand the challenges and problems children face after getting a CD diagnosis.
CD is defined as a chronic autoimmune enteropathy of the small intestine that occurs due to exposure to gluten in genetically predisposed individuals. 1 Gluten is a protein found in wheat, barley, and rye, which can cause CD.
Anemia, anxiety, diarrhea, irritability, infertility, skin rash, and failure to thrive are the main symptoms of the condition in children. 2 In the first report from Ludhiana (Punjab), a questionnaire-based survey of 4347 school children (3–17 years) reported the prevalence of CD to be 1 in 310. 3 It has been found that Indian children with CD often have delayed diagnosis. 4 To avoid long-term complications, early diagnosis of CD is essential. 5
The only treatment available for CD is a lifelong gluten-free diet (GFD), a diet free from wheat, rye, and barley. However, adherence to GFD is not easy, it comes with a lot of challenges, issues, and burden for the patients and their families. 6 The psychological implications of having CD are often overlooked. After the diagnosis, that may be disturbing for most patients, but it is a sigh of relief for some who are looking for a name to the problem so that they can finally have a solution; starting a GFD, affecting family dynamics too, all need attention for better management and treatment of CD. At all ages, following GFD is a challenge, and eating out was found to be difficult for teenagers. 7 Maintaining adherence to the diet could cause social, cultural, financial, and practical difficulties for the adolescent age group. 8 Therefore, there needs to be an emphasis on the role of mental health professionals in helping patients to deal better with CD and its challenges; 9 to make their daily living more manageable; and to help them develop assertiveness to say no when needed and remove the stigma and lack of seriousness around this invisible disease. This needs to be tapped on especially in the Indian context.
The experiences of children with CD have not been thoroughly studied in India. For children with CD and their families, the lack of GF options outside home, combined with a lack of knowledge regarding CD, can present many difficulties.
CD was also found to be associated with an increased risk of developing depressive and disruptive behavioral disorders which were present particularly before the initiation of GFD. 10 It was suggested that routine check-ups should be conducted by physicians to evaluate children and adults with gluten-related disorders for psychiatric manifestation. 11 An early detection of mental health problems in children with CD is important. 12
Many Indian families with a celiac child face difficulty avoiding cross-contamination, and they encounter significant difficulties when dining out, attending events, and school. 6 Educating patients about a disease and its associated challenges can help them to cope and adapt with the disease efficiently by increasing their health literacy. 13
Since manufactured GF products are more expensive than their non-GF equivalents, the lack of GF items and the additional cost might make the situation more troublesome for the patients and their families. 14 On the other hand, the stigma associated with the disease can play havoc on the psychological well-being of the patient. The GFD-associated stigma is found in adolescence. 15
There is some research regarding the dilemmas experienced by women and men in their everyday lives in relation to CD. One hundred and ninety-five dilemmas were experienced by the patients diagnosed with CD, which were identified in the domains of travelling, purchasing GFD items, at work, and having food at home and outside. 16 A dilemma in this study was defined in terms of a puzzling or uncomfortable situation that is perceived by the patient as disrupting their everyday life. For example, several participants in the study mentioned that when they could not eat the food offered due to its gluten content, or if alternative gluten-free options were not available, they often felt isolated and lacking in competence. They experienced a deeper sense of connection when sharing the same meals. 16
Eighty dilemmas were also reported in three areas namely, food situations at school, meals at home, and meals outside. The authors concluded that children with CD undergo strong emotions associated with GFD. 17 In adolescents, the transition to adapt to CD and GFD is a continuous process. Support was found to be crucial when adjusting to this transition. 18
The aim of this study was to understand the experiences of children aged between 8 and 17 years living with CD in India. We have examined both the social and food-related experiences of children diagnosed with CD. The social and food-related experiences of children are closely intertwined due to the significant role that meals play in social interactions and bonding. Sharing meals with family, friends, and peers often serves as a foundation for building relationships, fostering communication, and strengthening social connections.
Additionally, the role of mental health and the psychologist’s contribution in India is not well understood in the context of CD, especially compared to the impact of a nutritionist. With this study, we hope to emphasize the importance of studying issues related to CD from a psychologist’s perspective in the pediatric CD population in India. We believe that this work will motivate others in the mental health domain to investigate each aspect related to CD in detail.
Materials and Method
The present study has used constructivism paradigm as the basis of the study. Constructivism philosophical paradigm understands the phenomenon from the experiences of the research participants, and the researchers also construct the meaning of the phenomenon through their subjective experience as well as that of the research participants. This study was conducted using a qualitative technique since it allows for a greater understanding of the experiences of the individual.
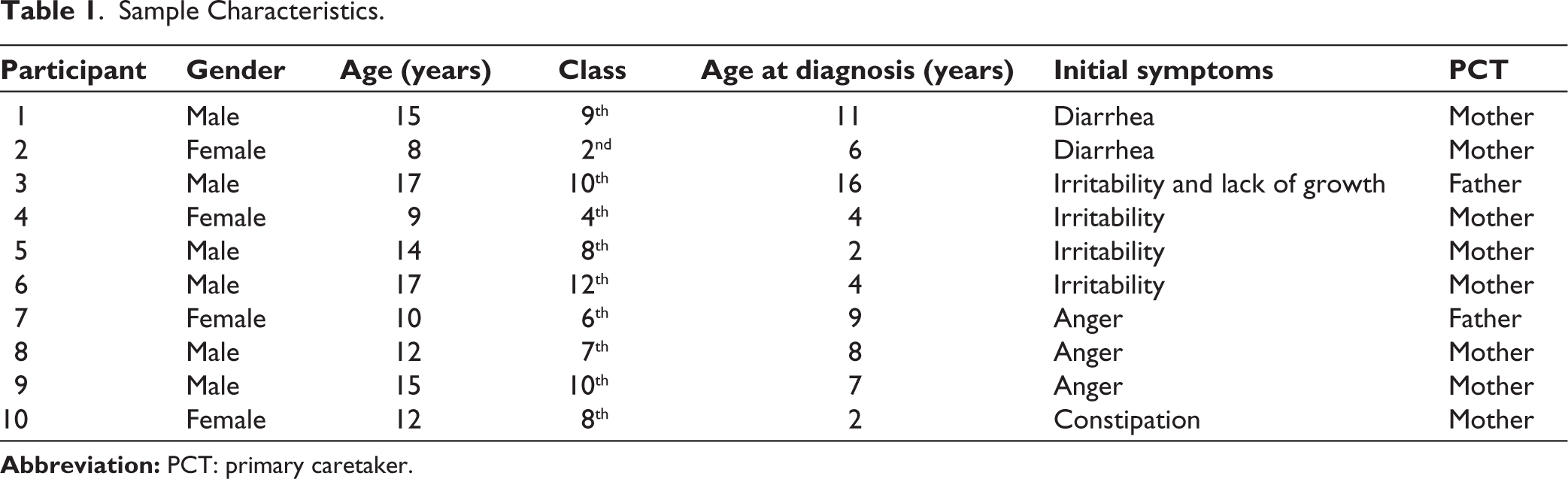
Participants were recruited from a pool of 50 children with CD from a celiac-related event at Ram Manohar Lohia Hospital, New Delhi, and Indraprastha Apollo Hospital, New Delhi. Inclusion criteria included (1) diagnosis of CD, (2) between 8 and 17 years of age, (3) on GFD for at least a year, and (4) without any psychiatric illness, cognitive deficits, or intellectual disability. The satisfactory performance in class as per their age group was viewed as an indication of the absence of any cognitive impairment. Parents of the eligible patients were contacted by phone to confirm their interest in the study. Only ten participants gave their consent to participate in the study. The study was conducted with ten children from Delhi/NCR who had been previously diagnosed with CD. Out of ten children, six were boys and four were girls. The mean age of the participants was 12.9 years (Table 1).
Sample Characteristics.
A qualitative interview was designed to explore significant life experiences, fostering a collaborative process between the interviewer and participant to construct knowledge and understand subjective viewpoints. The researcher maintained self-awareness through reflection to mitigate subjectivity and personal biases. Initial interview questions were deliberately broad, organized into thematic areas to provide an overview of the topic and align with research objectives. As the researcher gained deeper insights into the participant, questions evolved to elicit detailed responses. While some questions and responses overlapped, the emphasis remained on actively listening to participants’ stories.
The construction of interview schedule was based on literature review, interaction with celiac experts, gastroenterologist, dieticians, parents, and children. They were invited to the Royale Kalindi Hospital, New Delhi, before the interview. A rapport was built with the interviewee prior to the interview. Informed consent was obtained, replies were kept anonymous, and they were given the choice to refuse participation in the study; all requirements were fulfilled for ethical conduct outlined by the APA (7th edition). 19
The participants were interviewed in-depth over the phone. Due to the COVID outbreak, participants were hesitant for a face-to-face interview so telephonic interviews were conducted. Each interview lasted for around 25–30 min. Participants and their parents were informed of the study’s aim and were assured that their participation was completely voluntary and that they were free to discontinue at any moment. Every interview was performed by the same author.
Telephonic interviews were held, recorded, and then transcribed. Responding to immediate requirements, the questions were altered and left open-ended and a probe was used.
Some of the terms and words that were believed to be extremely native to the culture were written down verbatim by the researcher in her notes. In case of any questions, participants also received the primary investigator’s contact details. To ensure beneficence, after the data collection, all participants were given information on the different advantages of GFD. The data were then examined using thematic analysis.
An example of an open-ended question from the interview schedule is “How has the disease affected your life?”
The interview schedule was divided into different areas such as effect of CD on their lives, diagnosis of CD, challenges of CD, management of CD, present and future concerns, and challenges of GFD.
Thematic analysis, as described by Braun and Clarke, 20 was the method used to understand the experiences of children with CD. The steps were: familiarity with the data, creating initial codes, searching for the themes, reviewing themes, and defining and naming them. 20
In this study, a data-driven approach was favored, prioritizing open-coding of the data instead of applying predefined coding frames. This method aimed to comprehensively capture the rich and nuanced experiences of the participants. 21 However, alongside this approach, a theory-driven method was also employed to identify patterns that aligned with existing theoretical frameworks. This combined approach allowed for a thorough exploration of the data while also considering established theories to enhance understanding and interpretation.
Results
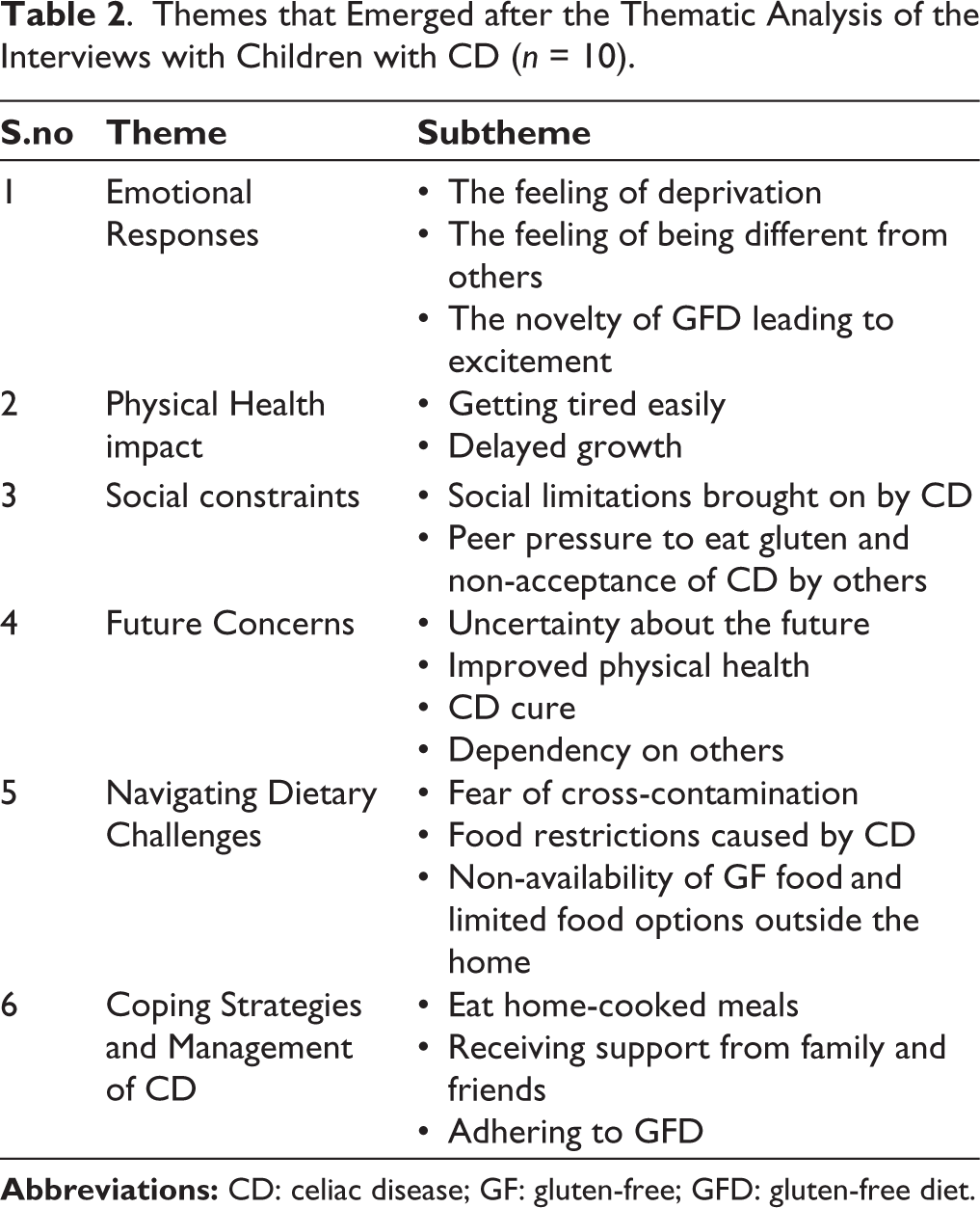
This study explored the lived experiences of children with CD in the Indian context. The participants explained their day-to-day life with CD. The findings revealed various issues and challenges experienced by children with CD. Thematic analysis was used to analyze the data. 20 The analysis of the data with children resulted in 6 themes and 17 sub-themes (Table 2).
Themes that Emerged after the Thematic Analysis of the Interviews with Children with CD (n = 10).
Theme 1: Emotional Responses
Emotional responses to CD include anxiety, depression, and stress due to the challenges of adhering to a strict GFD and treatment. Additionally, a few participants experienced excitement because of the novelty of the GFD, seeing it as a new and distinct way of eating.
Due to lack of food alternatives available to them and the social constraints imposed by GFD, the majority of children with CD reported feeling deprived. One participant commented “I used to have a problem when I couldn’t eat with everyone. Like if there are chocolates, everyone is eating; only I couldn’t eat them”. Deprivation further contributed to feelings of frustration, isolation, stress, anxiety, depression, and even resentment toward their condition and its dietary requirements.
When they could not participate in activities or eat like other healthy children, children said they felt different. One of the participants stated “Sometimes kids used to tease because of this (CD). They said that he can’t eat that, so nobody should give him that, he is different in the class”. Teasing can evoke various emotional responses such as feelings of embarrassment, shame, frustration, anxiety, depression, or anger due to being singled out or made to feel different. A participant further stated “When we go out, society sees us differently.” “We can’t tell everybody that I can’t eat wheat. I feel weird”. Overall, feeling “weird” in these situations can lead to a range of negative emotional responses related to social perception and acceptance.
Another response noted was enthusiasm due to the novelty of GFD, due to its new and distinct nature as a diet. “But first I experienced a little excitement that I will not be able to eat wheat”. On further asking what kind of excitement, the child responded “Like when a kid gets a new toy like that”.
Theme 2: Physical Health Impact
Participants commonly reported symptoms like fatigue, body pain, and abdominal discomfort, alongside concerns about delayed growth and peer comments on stature, further highlighting the condition’s adverse effects on health and well-being.
A participant reported an effect on the physical health as “I feel tired easily and I feel pain in my body”. Another participant reported effect of CD on physical health as “Earlier, when I used to do any work, I got tired, and my legs hurt a lot. Due to the pain in my legs, I used to come on the verge of crying.”
On asking a participant how his friends react to his delayed growth, he reported “Like they call me Chotu-Chotu (Short boy-Short boy).” One of the participants claimed that CD had a negative impact on his physical health “Like sometimes I get fever or abdominal pain. I feel tired easily sometimes. I have gained some height but not much”.
Theme 3: Social Constraints
“Social constraints” refer to the challenges participants encounter in social settings due to dietary restrictions, such as difficulty participating fully in gatherings involving food and feeling excluded.
On asking about the influence of CD on their life, one participant reported “I sometimes feel that I can’t go out like others are going.” He further added “It has affected by social outings”.
According to another participant “Yes, relationship gets affected. When there is a birthday party of a friend but I can’t party with my friend. I can’t share my lunch. I can’t take treat from my friends. They do not support me.”
When the child could not eat with other people, it was also evident that the child felt alone. “Everybody sits together to have food but I can’t eat with them, I can’t eat. Everybody eats first then my food is cooked. So, I don’t sit with them. They keep eating their food and I eat separately”. In the words of another participant “If somebody brings food at home like gol gappe (savory snack eaten with spiced water), bread pakoda (bread fritter with potato filling), samosa (savory with stuffed fried potato pastry) I also feel like eating then I go inside the room and sit in a corner. I try to ignore. I use my mobile if there is a party going outside.” Eating snacks like gol gappas and bread pakodas, popular South Asian street foods involves navigating several cultural components. Gol gappas are often consumed in social settings, such as street food stalls or family gatherings. Sharing and enjoying this snack with others is a common cultural practice, fostering social bonds and community connection. However, individuals with CD may need to refrain from consuming these foods due to their gluten content, which can lead to feelings of exclusion or isolation in social gatherings where such foods are central.
Pressure created by others for eating gluten and non-acceptance of CD by others was recognized as a challenge of CD by few participants. As reported by a participant “If somebody forces us to eat then we eat by mistake”. Another participant stated “I don’t eat, they keep insisting eat a little but I never eat”.
Theme 4: Future Concerns
The “Future Concerns” theme in CD highlights individuals’ apprehensions about the condition’s trajectory, encompassing uncertainties about its management, worries about physical health and growth, concerns regarding a potential cure, and dependencies on others, notably in food preparation away from home.
A small number of participants expressed uncertainty about their future, including how they would handle their CD. One of them stated “If I will not get a job then it will be a big problem, what will happen. I will not be able to make friends and will not get a job…Like I can’t see my future”.
Participants also reported a future concern regarding their better physical health including growth. One participant stated “I am concerned about my height and abdominal pain. My classmates are all taller than me”.
CD cure was also found to be a concern of few participants. Participants wanted a permanent cure for CD in the near future “I think what will happen in the future. What will happen in the future… It will be cured or not, what problems will be there?”
Another concern that emerged was dependency on others. A participant stated “When I grow-up and go out for a job then I can’t eat roti (wheat flatbread) or wheat. Now mom makes it as I am small, who will make it for me outside the home?”
Theme 5: Navigating Dietary Challenges
“Navigating dietary challenges” entails balancing the intricacies of sticking to a stringent gluten-free regimen while ensuring a healthy diet. Participants in the study emphasized the challenge of balancing a strict GFD with nutritional needs, facing fears of cross-contamination both at home and outside. Limited availability and high costs of gluten-free foods in India added to the difficulty, sometimes leading participants to reluctantly consume gluten when alternatives were scarce.
Most participants believed that one of the biggest challenges to managing CD was the fear of cross-contamination within and outside the home. One participant reported “My utensils are separate but there is a constant fear”. A participant reported fear of cross-contamination outside the home as “There is a fear of cross-contamination. Most of the people outside say that the food is fine, it doesn’t have anything. I feel scared that it might contain gluten”. Another participant reported fear of cross-contamination as “I fear cross-contamination. I feel it is the main challenge”.
CD was also found to cause food restrictions mainly because of the fear of cross-contamination and non-availability of GF food items outside the home; palpability was a major concern “umm I can’t eat good things”. The major effect of CD on life as reported by one of the participants was not able to eat like others “Eating! Like others eat I can’t do that”. A participant said “My mother makes pakodi (gram flour or rice fried dumplings) and fills it in the tiffin. I feel like having other children’s tiffin”.
Non-availability of GF food and limited food options outside home emerged as another challenge. In the words of one of the participants “Like I can’t eat a lot outside”; the participant further added “Only I can eat limited things”. Being a new GF market, India has a limited and costlier supply of GF food. One participant reported that “Sometimes I eat gluten…when I am not able to find anything for me to eat then I have to eat gluten”. Another participant stated, “When going out then it is difficult to eat outside”.
Theme 6: Coping Strategies and Management of CD
Participants stressed the importance of coping strategies like eating home-cooked meals and receiving support from family and friends to manage CD. Adhering strictly to a GFD, even when dining out or traveling, was seen as crucial, highlighting the significance of following medical advice for optimal health.
The participants discovered that one method of managing CD was by eating home-cooked meals. One participant claimed that by eating at home, one can cope and manage CD by avoiding going out “Whatever I feel like eating, mommy makes it at home. So, I do not go outside. I eat any food item made up of rice. So, I avoid going out because of this”.
Having the support of family and friends was beneficial in managing and coping with CD “My friends never force me to eat, they help me”. According to another participant “My friends do not see me differently nor my family members”. Adhering to GFD was reported by many participants as a way to cope and manage CD “Best way…whatever diet a doctor suggests, follow that only. Ignore everything irrelevant”. A participant stated “A celiac should eat what is suitable for him”. The participant further added that “If you are going out then take your food along with you. Try to avoid eating outside food. If you are going on a trip then take gluten-free rusks and biscuits”.
Discussion
The findings of the present study revealed 6 themes and 17 subthemes. The findings provide an in-depth understanding of the lived experiences of children with CD in the Indian context. The six themes that emerged include emotional responses, physical health impact, social constraints, future concerns, navigating dietary changes, and coping strategies and management of CD.
The absence of gluten-free alternatives for children frequently causes both parents and children to feel deprived and at a loss. 22 It was discovered that the participants’ feelings were stimulated when they were not able to eat the same thing as others, particularly at home when sharing meals with others became difficult. 23
Additionally, it was noted that celiac patients had a feeling of being different and isolated, particularly during a break for lunch when no GF options were available. When consuming the same cuisine, the participants felt a greater sense of unity. 23 Commensality was found to play an important part in social processes. 24
It was found that the patients’ prevalent negative emotions were loneliness and frustration with regard to GFD. 23 It was emphasized that when eating moves from the social to the domestic area, the detrimental impacts of GFD become more obvious. 25
In this study, an unexpected emotion that surfaced was excitement due to the novelty of GFD. When told that he must adhere to a GFD, a participant claimed that he felt delighted. The family had never eaten a GFD before. The novelty of GFD to the family may have caused the child to be excited about trying a new meal and enjoying the diet like a new toy.
Children’s health was impacted by late and inaccurate CD diagnoses. Early diagnosis is important to avoid long-term complications of CD. 5 Health-related quality of life (HRQoL) was impacted by untreated CD. 26 Psychological problems like anxiety, depression, and fatigue were frequently experienced by untreated CD patients, but once on GFD, these symptoms go away in a few months. 27 Fatigue is present in many patients with untreated CD but adhering to diet can alleviate fatigue in many cases.28,29 It was also found that one-third of children with short stature have CD. 30 This highlights the importance of early diagnosis and treatment to improve children’s overall health and well-being.
In India, there are relatively small number of exclusively gluten-free restaurants, which are costly and not always located in every location. The absence of explicit GF labelling further exacerbates the problems. Due to the low level of public awareness of CD, the situation for celiac patients is challenging. Lack of public education was also found to be an important factor associated with the challenges found in patients with inflammatory bowel disease. 31 It was reported that difficulties are experienced by the CD patients in dining out and travelling. 32 Few participants reported that sometimes other people pressurize them to eat gluten containing food. It was found that the main reason for not following GFD was difficulty in peer relations, for instance, rejection by the peer group. 33 One of the difficulties faced by the participants was non-acceptance of CD by others. Educating about CD could help in changing the perception toward this disease, leading to its acceptance in the community. 22
The study’s participants also voiced some concerns about the future. Since there is currently no cure for CD, participants were unsure of their ability to manage their condition and what would happen if they did not adhere to society’s standards for ideal height or a typical diet. During the interview, a future concern for better physical health surfaced.
It was discovered that having good physical health was related to having higher professional possibilities. Concern for more rapid physical development was important since it prompted comparisons with peers and helped one win their approval. The patients’ health was impacted by cross-contamination or GFD non-compliance. Children frequently complained of fatigue, slow growth, and chronic abdominal pain. In children, the most common symptoms were short stature, fatigue, and headache. 34
Participants raised yet another future concern about CD treatment. Currently, there is no cure for CD, and the only available therapy is a GFD for the rest of one’s life, which poses a number of constraints for the patient. 35
Following a GFD can be extremely challenging due to nutritional deficiencies associated with the diet, high costs involved, and negative psychosocial impact. 36 The patients require the long-awaited CD miracle drug to be free from all GFD-related problems. The participants’ ability to manage in the future, particularly after marriage, may be connected to the desire for permanent CD treatment. CD and a need to adhere to a GFD were found to have a substantial effect on dating and intimacy. 37 The need to follow GFD was found to be associated with negative emotions like anger. 38 It is also important to educate the children regarding GFD to make them independent when they go out for higher studies or work. Adherence to GFD requires patient education, follow-up, and motivation. 39
It was found that in adult celiac patients there was an apprehension about gluten contamination. Even after it was proven that their food was gluten-free, the patients would still occasionally check it. The participants were afraid of developing gluten intolerance symptoms. 16 Inadvertent non-adherence to GFD was found when a gluten-free product gets contaminated with gluten and inadvertent non-adherence is more common than non-adherence on purpose. 40
Participants in this study who were aware that even their utensils were separate and that their family took every precaution to prevent cross-contamination nonetheless expressed a dread of it. This concern existed even if the food was cooked by family and friends. 16
Another challenge the participants encountered was the lack of food options away from home. There is a dearth of knowledge regarding gluten-free food in India, and packaged GF food products are either hard to find, expensive, or not checked for gluten. 22 It is quite difficult to find gluten-free alternative of a savory snack. Restricted product choice was important in the management of CD in daily life as taste and variety in GF products was difficult to find. 19 Non-availability of GF food outside affects travel, occupation, and profession. 6
Another theme that developed was coping strategies and management of CD. Eating only home-cooked food would also cut down on the trouble of double-checking any suspicious food, greatly reducing the need for ongoing CD monitoring. The most disturbing dilemma of management of daily life in celiac patients was being constantly on call that was related to checking food which they ate and constantly worrying about doing anything wrong. 16 Home cooking was found to be an important tool of GFD management. 41
Adolescents with CD were found to benefit from peer support in terms of their quality of life (QoL), reduced social isolation, and enhanced positive coping. 42 Family processes play an important role in the adherence to GFD. 43 Acceptance and support from family and friends make it easy for the patients to manage their CD.
Adhering to GFD emerged as another strategy. GFD adherence was found to be linked to better QoL in CD patients. 44 The participants were aware that properly following GFD will help them control and lessen their symptoms.
In conclusion, the present study provides an in-depth understanding of the lived experiences of children with CD in the Indian context. This study fills an important gap that existed in the field of pediatric celiac population in India due to the scarcity of literature on the difficulties faced by children with CD in India. The study advances our understanding by focusing on what it is like for children with CD in India and highlights the importance of mental health in the management of CD.
The findings will broaden our understanding into the challenges and problems children with CD face in India. It will also help doctors, nutritionists, policy makers, and especially mental health professionals to address the issues and challenges faced by children with CD. The findings can also help to design effective interventions for addressing the challenges and issues of living with CD.
In the present study, telephonic interviews were conducted due to the COVID outbreak. Future studies can focus on conducting face-to-face interviews. The sample was drawn from Delhi/NCR region but future studies can include samples from other parts of India.
Footnotes
Acknowledgements
We thank the Indian Council of Social Science Research, Celiac Support Organization and Royale Kalindi Hospital, New Delhi for their support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
The study was approved by the Ethical Approval Committee, Vivekananda College, University of Delhi (Ref.no. 2/2023). The study was carried out in accordance with the ethical principles of the American Psychological Association and the Declaration of Helsinki.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was part of a postdoctoral research supported by the Indian Council of Social Science Research.
Statement of Informed Consent and Ethical Approval
Informed consent was taken from all the participants as well as from their parents.