
Abstract
A strict gluten-free diet is the only treatment for celiac disease, and it is especially challenging among adolescents. Participation in food-related activities and self-managing the chronic health condition involve use of cognitive skills. This cross-sectional study examined how executive functions might be associated with participation in food-related activities. Adolescents aged 12–18 years (N = 65; Mage = 14.67) with celiac were interviewed about participation, and their parents completed an executive function questionnaire. Poorer participation significantly correlated with poorer executive abilities. Identifying executive function profiles may contribute to understanding and advancing resourceful daily functioning and participation in daily food-related activities.
Introduction
Celiac disease (CD) is an immune-mediated enteropathy caused by ingestion of a protein “gluten” found in wheat, rye, and barley. Almost 1% of the world population is affected by CD, and following a strict lifelong gluten-free diet (GFD) is the only accepted treatment thus far (Bascuñán et al., 2017; Howard and Urquhart-Law, 2014; Lindfors et al., 2019; Singh et al., 2018). Up to 60% of those with diagnosed CD are partially non-adherent, and among children and adolescents, nonadherence to the diet ranges from 19% to 56% (Hall et al., 2009; Lindfors et al., 2019). Adherence to a strict GFD is challenging, especially during adolescence, a time of the complex transition from childhood to adulthood that has unique health and developmental issues (Bascuñán et al., 2017; Hall et al., 2009; Holbein et al., 2018; Lindfors et al., 2019; Ludvigsson et al., 2016; Samasca et al., 2017; Wagner et al., 2015; World Health Organization, 2017). Adolescents expand their daily life activities to environments further away from their home circles, predominantly with peers (Vroman, 2015), for example, at social gatherings, outings, parties, sleepovers, trips camps, and eating out (Fishman et al., 2018; Meyer and Rosenblum, 2016; Rashid et al., 2005). Just like their peers, adolescents with CD have the same desire to be involved, engage and to eat with their peers, and to equally participate with them in a range of daily food-related activities (Ludvigsson et al., 2016; Meyer and Rosenblum, 2017a, 2018; World Health Organization, 2001).
While the home environment has been described as a safe setting without marked difficulties for adolescents with CD (e.g. Biagetti et al., 2013; Cederborg et al., 2012; Olsson et al., 2009), challenges when away from home, such as in social activities and on trips, are recurrent (Meyer and Rosenblum, 2017a, 2018). These adolescents need to know how to skillfully navigate a lifetime of social situations, many of which involve food-related challenges (Wolf et al., 2018). To maintain the GFD in a world comprising complex challenges related to food, while fully participating like their friends, they need to manage their GFD and find solutions to challenging situations in varied out-of-the-home environments. To do this, they use cognitive skills and self-control for effective and resourceful self-management (Bellini et al., 2011; Dawson and Guare, 2018; Meyer and Rosenblum, 2017a; Wolf et al., 2018). Self-management is the interaction of health behaviors and related processes, as well as the lifetime tasks of caring for oneself (such as managing a diet) and living well with a chronic condition (Lorig and Holman, 2003; Modi et al., 2012). Self-management includes a range of core skills such as decision-making, carrying out plans, and flexibility and problem-solving that support learning, remembering, planning, and deciding. These skills are defined as executive functions (EFs), and they are fundamental to efficient everyday life when confronted with new challenges (Center on the Developing Child at Harvard University, 2011; Dawson and Guare, 2018; World Health Organization, 2001). Understanding the possible impact of EFs on human behavior is important when a change in health behavior is needed (Reimann et al., 2020). Eating behavior involves EFs, especially when people need to carry out specific dietary requirements that require planning of meals and making decisions to select and avoid certain foods. Thus, carrying out the GFD may involve EFs when planning and making decisions about what to eat in food-related activities that occur in daily life (Dohle et al., 2018; Meyer and Rosenblum, 2017a). Research about the role of executive control in eating behavior has emerged over the past decade, yet not necessarily related to CD (Houben et al., 2018). Research involving various behavioral constructs concerning how adherence to the GFD occurs and self-management among populations with CD is also emerging, as is research related to the critical transition from childhood to adulthood (Clerx et al., 2019; Kothe et al., 2015; Ludvigsson et al., 2016; Sainsbury et al., 2018). However, this study focuses on the executive control involved in the management of food-related activities specifically among adolescents with CD who keep to the GFD in everyday life, in light of the unique challenges during this transitional period (Ludvigsson et al., 2016).
Therefore, the aim was to explore how EF components might be associated with characteristics of participation in food-related activities outside the home among adolescents with CD. We hypothesized that adolescents with CD will exhibit a wide range of executive abilities and suspected deficits and will have a range of participation in food-related activity characteristics. We also hypothesized that significant correlations will be found between EFs and participation characteristics and that each adolescent will present their own unique EFs and participation profile.
Methods
Participants
The sample of 65 adolescents described in this article was part of a larger cross-sectional study in Israel that included 61 children (aged 8–11 years) and 65 adolescents (aged 12–18 years) diagnosed with CD. Participants volunteered for the original study by responding to advertisements via local celiac associations, local online support groups, and social media from February to September 2015. Inclusion criteria were a confirmed diagnosis of CD by a physician (as reported by parents) no less than 6 months prior to the study. Exclusion criteria were additional physical or neurological disabilities. Volunteers who responded to the recruitment call and were found eligible were included in the study. Written informed consent was obtained from both adolescents and their parents prior to their inclusion in the study. The study was approved by the institutional ethics committee (approval number 026/15). Hebrew versions of the following measures were administered.
Demographic assessment
Parents completed a demographic questionnaire about themselves and their children (e.g. age, sex, education level, CD health status). Parents were asked to rate their child’s level of adherence to the GFD on a 5-point Likert-type scale (1 = always to 5 = no adherence). Adolescents responded to a 4-item questionnaire about gluten intake in home and out-of-home settings, rated on a 5-point Likert-type scale (1 = never to 5 = all the time; Howard and Urquhart-Law, 2014).
EF assessment
Parents completed the Behavior Rating Inventory of Executive Function (BRIEF) questionnaire (Gioia et al., 2000). The BRIEF is an 86-item ecological parent-rating scale of the executive functioning in daily life of children aged 5–18 years. Parents rate the frequency in which each behavior described in each item occurs (3, often; 2, sometimes; and 1, never). The BRIEF provides eight clinical scales: inhibition, measures the ability to resist, to stop one’s behavior at the appropriate time; shifting, reflects the ability to shift, or flexibly move, from one situation or aspect of a problem to another according to the activity or situational demands; emotional control, measures the impact of EF problems on emotional expression and assesses the ability to modulate or control emotional responses; initiation, describes the ability to begin a task independently, create ideas, and use problem-solving strategies; working memory, assesses the ability to hold and manipulate information over a short time to complete a complex everyday life task; plan/organize, measures the ability to manage current and future-oriented task demands; organization of materials, measures orderliness of work, play, and storage spaces; and monitoring, assesses one’s own performance during or shortly after finishing a task and evaluates whether one keeps track of the effect the behavior has on others. A score of 65 or greater signifies potential clinical executive deficits. The BRIEF has been validated among healthy and clinical populations. Internal consistency ratings range from .82 to .98 (Gioia et al., 2000).
Participation assessment
To capture the actual real-world experiences of daily life with CD, adolescents were interviewed using the Celiac Disease-Children’s Activities Chart (CD-Chart; Meyer and Rosenblum, 2017b). The CD-Chart includes nine food-related activities that occur in the following: the social environment (e.g. eating out with friends), the close family environment (e.g. family meals and events away from home), and the trip environment (e.g. eating meals on overnight school trips). Activities are scored across six dimensions: (a) activity defines whether the child or adolescent engages in the activity, (b) frequency (how often), (c) preference/liking (how much the interviewee likes the activity), (d) preparation defines whether participation in the activity requires any special advance preparation, (e) involvement assesses the level of the child’s or adolescent’s involvement in the preparation process, and (f) self-determination reflects the degree of importance a child attaches to performing independently.
Procedure
Parents and adolescents provided demographic data via a secure web link. The CD-Chart was administered by the first author, a health professional, at each family’s home, while the parents completed the BRIEF. The data completed by the parents were examined by the first author, and any missing values were completed during the home visit.
Statistical analysis
Analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 23.0. Descriptive statistics, including means, standard deviations, and frequencies, were used to describe continuous variables and frequencies. Data were normally distributed, and assumptions for parametric tests were checked. Continuous variables were compared using t tests, and the standardized difference between two means was indicated using Cohen’s d. Multivariate analysis of variance (MANOVA) was used to test for group differences in EFs, and univariate analyses of variance (ANOVAs) were calculated to examine the source of the significance. The data revealed participants with and without potential executive deficits. Consequently, to differentiate between these different executive characteristics, the EF data are presented prior to the participation data in the following “Results” section. Pearson chi-square values determined associations between EFs and participation measures. Statistical significance was defined with an alpha level of .05.
Results
Participants included were 65 adolescents (43 girls, 22 boys) aged 12–18 years (M = 14.67, SD = 1.77), who attended 6th–12th grades (M = 8.94, SD = 1.94) in mainstream schools. Demographic and health characteristics are presented in Supplemental Table 1. Primarily, each BRIEF (Gioia et al., 2000) scale score was calculated for the entire sample of adolescents (N = 65). Mean scores of all eight EF scales for the entire sample were within the clinical cutoff (i.e. <65), indicating no potential clinical EF deficits (see Supplemental Table 2). No significant differences were found between boys and girls, and no associations were found between the EFs and the current age, age at diagnosis, years since diagnosis, mother’s years of education, additional family members diagnosed with CD, or adherence.
Although mean scores of all eight EF scales for the entire sample were within the clinical cutoff, careful observation revealed a wide scale score range indicating potential clinical EF deficits among more than 20 children in varied EF scales. Thus, to deepen our understanding, the sample was divided into two subgroups. Subgroup A (n = 39; 66.7% females), participants without potential clinical EF deficits in any BRIEF scale according to the clinical cutoff (i.e. all scales scores were below 65). Subgroup B (n = 26; 65.4% females), participants with potential clinical EF deficits in one or more BRIEF scales according to the clinical cutoff (i.e. one or more score of 65 or higher). No significant differences were found between the two subgroups in any of the demographic or the health variables that appear in Supplemental Table 1.
Although the mean BRIEF scale scores do not represent potential EF deficits, the adolescents in Subgroup B had potential deficits in one or more BRIEF scale (see Supplemental Table 2). For example, 50% of the adolescents had difficulties with shifting and 31% had difficulty in planning/organizing. Comparing the EF scores in the two subgroups (A and B) indicated a significant difference in all the BRIEF scale scores, with higher scores (poorer functioning) in all scale scores among the adolescents with potential EF deficits (F(1, 63) = 9.01, p < .000,
Initially, associations between the demographic variables and participation characteristics were examined for the entire sample. No significant correlations were found between the CD-Chart participation outcomes and the adolescents’ current age, age at diagnosis, years since diagnosis, mother’s years of education, or additional family members diagnosed with CD, and there were no significant differences between boys and girls. Most of the adolescents participated in all the CD-Chart food-related activities and required special preparation before their participation. Core dimensions of the CD-Chart in activities outside of the close home environment are presented in Supplemental Table 3.
Analysis revealed significant difference in self-determination in the social environment. The adolescents in the group with potential EF deficits (Subgroup B) reported a substantially higher degree of importance to perform independently (t(63) = −.270, p = .01, d = 1.15).
Significant negative correlations were found for the entire sample between the social environment and trip environment CD-Chart dimensions and the BRIEF shift and initiate scores. The negative correlations, presented in Supplemental Table 4, indicate that higher scores on the BRIEF scale (i.e. poorer executive functions) correlate with poorer participation according to the CD-Chart. To identify further how the different EFs relate to participation, correlations were calculated separately for each subgroup (A and B) where significant negative correlations were found. The BRIEF scales and CD-Chart dimensions with no significant results in any group are not listed in Supplemental Table 4.
To demonstrate the clinical meaning of the correlations between EFs and participation, individual BRIEF and CD-Chart data of two participants with potential EF deficits are presented in Table 1. “David” is a 15-year-old 9th grader and “Rachel” is a 17-year-old 12th grader; both were diagnosed with CD 3 years before the study. Their EF profiles are demonstrated in Figure 1.
Examples of BRIEF and CD-Chart correlations: two participants with potential executive function deficits.
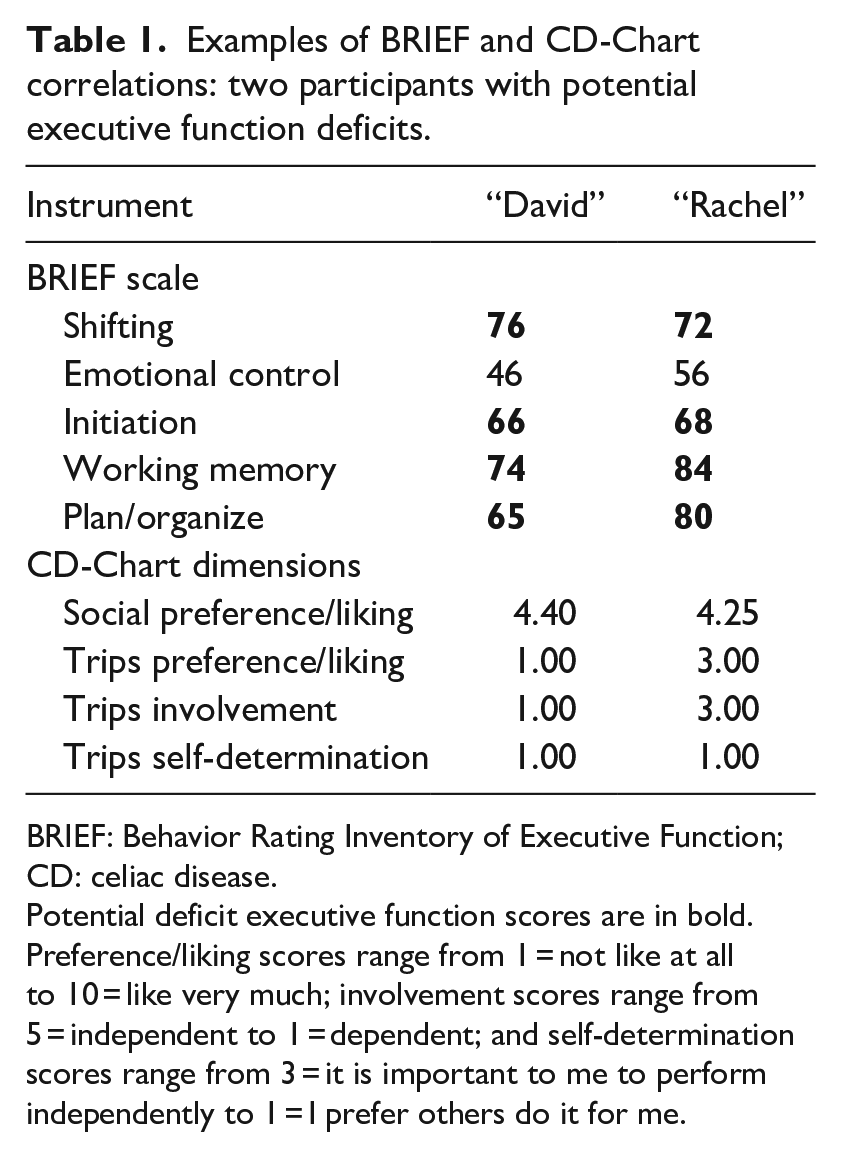
BRIEF: Behavior Rating Inventory of Executive Function; CD: celiac disease.
Potential deficit executive function scores are in bold. Preference/liking scores range from 1 = not like at all to 10 = like very much; involvement scores range from 5 = independent to 1 = dependent; and self-determination scores range from 3 = it is important to me to perform independently to 1 = I prefer others do it for me.
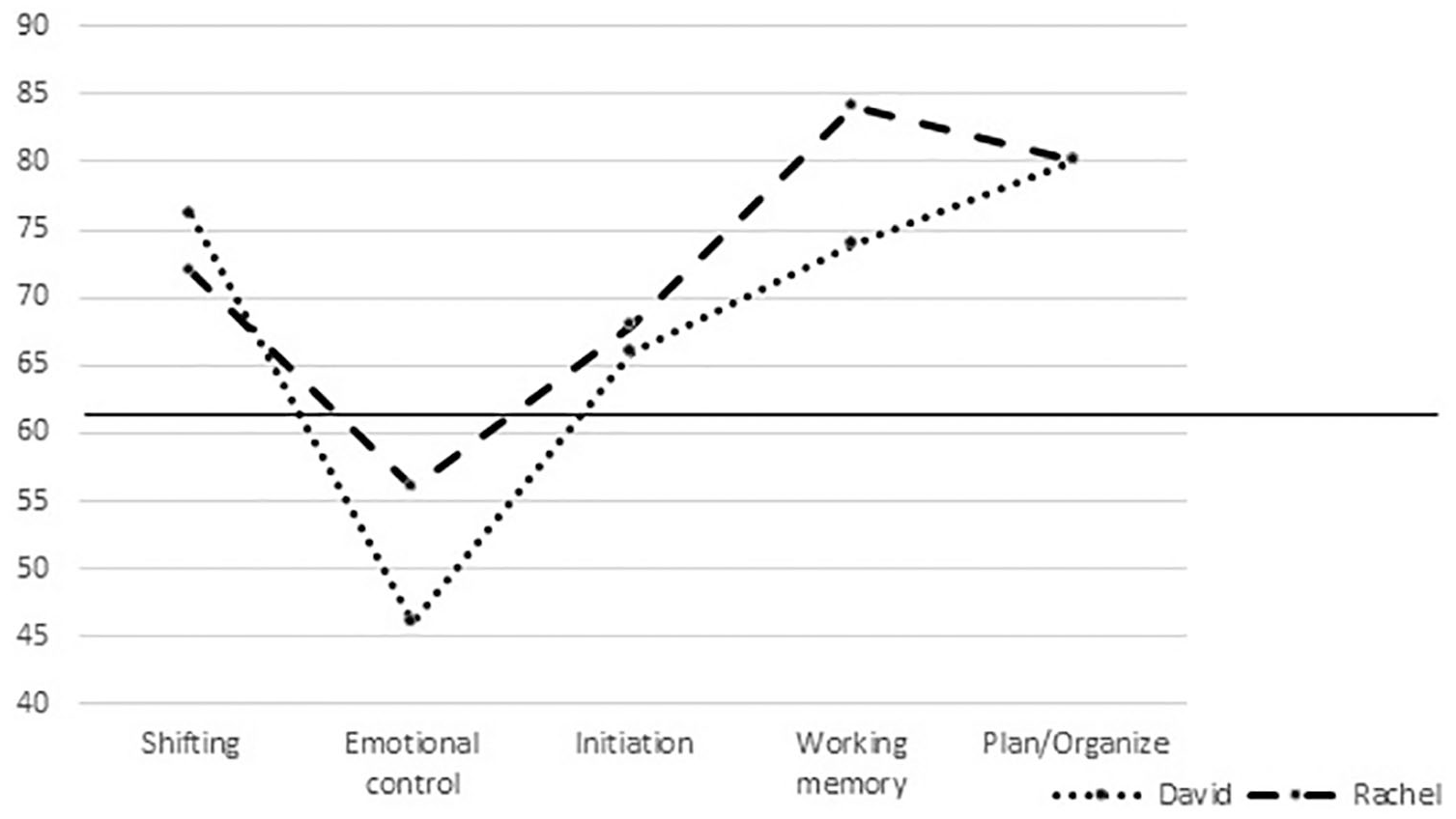
Examples of executive function scores: “David” and “Rachel.”
“David” and “Rachel’s” scores (Figure 1) demonstrate that although both have typical emotional control (below the solid cutoff line), they each present potential EF deficits in the BRIEF scales that correlated in this study with the participation characteristics (see Supplemental Table 4). They have similar initiation deficits, but “Rachel’s” working memory is substantially poorer than “David’s,” and “David’s” shifting abilities are slightly poorer than “Rachel’s.” They similarly rated a low preference/liking of participation in food-related activities in their social and trip environments. Although both prefer someone else to conduct the required pre-preparation before participating in food-related activities on trips, “Rachel” receives only some help from others in the preparation process and “David” is entirely dependent on others (Table 1).
Discussion
This study explores core self-management executive skills and presents associations with participation in food-related activities among adolescents with CD. The study’s findings ruled out relationships between the various demographic variables and the measures used in this study or differences between boys and girls, thus accentuating the importance of the associations between EFs and participation characteristics for individual adolescents.
The high rate of reported adherence in the current study, which differs from previous results (Errichiello et al., 2010; Ludvigsson et al., 2016; Newton and Singer, 2012), may be because all participants were volunteers from middle-class to upper-middle-class families, who may have a tendency for better adherence (Shah et al., 2014). Also, although self-reports are considered the best source of information for measurement of nutrition and health behaviors (Zingone et al., 2018), self- or parent-report bias may affect the reported adherence. Furthermore, the study focused on EF characteristics and associations with daily functioning while adhering to the diet and not merely adherence.
The EF profiles emphasize the diversity in cognitive mechanisms among adolescents who need to self-manage their health condition efficiently. The EF scale scores reveal not only whether they have efficient or deficit EFs but also individual cognitive variances. To illustrate, 50% of the adolescents have potential deficits in shifting, yet daily life with CD involves changing situations that require flexibility (Gioia et al., 2000; Meyer and Rosenblum, 2016). For example, when arranging to eat out with friends, adolescents with CD may well choose a restaurant with GF options in advance. However, if arrangements change, adolescents with CD would need to shift from the original plan to find new applicable GF solutions. Managing the GFD requires planning, and this responsibility gradually transfers from parents to the adolescents themselves (Fishman et al., 2018). Nevertheless, in this study, 31% of the adolescents had potential deficits in their ability to plan and to manage current and future-oriented task demands (Gioia et al., 2000). They may encounter additional challenges to their peers without planning deficits when attempting to navigate food environments (Wolf et al., 2018). Current CD guidelines and recommendations do not consider EF abilities or potential deficits (Bai and Ciacci, 2017; Fishman et al., 2018; Ludvigsson et al., 2016; Zingone et al., 2018). However, because EFs are vital to managing health behavior, self-management becomes crucial for these adolescents (Dawson and Guare, 2018; Fishman et al., 2018; Modi et al., 2012; Suchy, 2009; Testa and Simonson, 1996).
The CD-Chart reflects the complexity of functioning in the daily activities of adolescents with CD (Meyer and Rosenblum, 2017b). The results indicate that the added responsibility of preparation does not limit the number of activities in which the adolescents participate. Instead, they appear to choose to invest the additional time and effort required (Poulsen et al., 2013). This aligns with typical desire to fit in with peers during adolescence (Vroman, 2015). However, the adolescents’ relatively low preference/liking for participating in food-related activities, alongside their high adherence level, may result from the additional effort required to prepare to take part with their friends and peers (Wolf et al., 2018).
Adolescents with CD experience a range of age-related characteristics and daily challenges (Fishman et al., 2018; Ludvigsson et al., 2016; Vroman, 2015). Initial results of the correlation analysis of the entire sample demonstrated that some BRIEF scores indeed correlate with certain CD-Chart dimensions. However, significant relationships were found in each of the subgroups between potential deficits in shifting, initiation, and working memory (BRIEF scales) and poorer preference/liking, involvement, and self-determination in food-related activities (CD-Chart). In addition, associations found between EFs and participation in the subgroup with typically developing EFs highlight the impact of more efficient EFs on adolescents’ daily participation in food-related activities, even within the norm. Interestingly, various correlation patterns were found in the two subgroups, even where no correlations were identified in the entire sample. This pattern may be related to the fact that better functioning in one EF domain does not automatically generate successful performance in all areas of health behaviors. In addition, the ability to withstand unhealthy behaviors, does not necessarily transfer to the ability to initiate selection of healthy choices (Allom and Mullan, 2014). This outcome may be attributed to the limited sample in this study and requires further exploration.
The finding that shifting abilities are associated with activity and participation functioning provides better understanding of the health behavior patterns. Given that CD presents many daily challenges for adolescents (White et al., 2016) and that potential shifting deficits may result in problem-solving difficulties difficulties (Dawson and Guare, 2018; Gioia et al., 2000), the ability to solve problems while shifting between changing circumstances is a vital skill. Adolescents with potential shifting deficits may have difficulties in problem-solving processes and require more support or be more dependent on others (Fishman et al., 2018). This reliance may cause the adolescents to dislike participating in such activities, as reflected by their lower preference/liking ratings of social and trip activities.
Relationships were also found between the importance attached to performing independently and to initiation in the group with potential EF deficits. Initiation is an EF that reflects a person’s motivation and willingness to engage in activities (Poulsen et al., 2013). Deficits in initiation can lead to the need for external prompts to begin an activity (Gioia et al., 2000). Surprisingly, associations between initiation and the level of involvement in preparation before participating in food-related trip activities (meaning poorer initiation is associated with less involvement) were found only among the adolescents without potential EF deficits. Possibly, the adolescents with potential initiation deficits are accustomed to receiving external prompts and assistance in other life activities and may overestimate their abilities (Steward et al., 2017). In general, adolescents strive to determine independence, and adolescence represents the developmental stage at which they are expected to acquire the skills needed to carry out adult roles (Bonikowsky et al., 2012; World Health Organization, 2017). Because adolescents with CD need to implement self-management skills to manage their health condition (Fishman et al., 2018), potential deficits in their initiation ability may possibly affect their ability to act independently and resourcefully when encountering challenges to their participation in daily life activities.
Working memory is crucial for performing multistage activities, such as daily tasks that become more complex in the transition from childhood to adolescence (Center on the Developing Child at Harvard University, 2011; Dawson and Guare, 2018; Meyer and Rosenblum, 2017a). Working memory is also a vital factor in a person’s ability to follow through long-term goals such as maintaining a healthy diet (Dohle et al., 2018). Deficits in working memory skills can compromise the way adolescents with CD cope with the growing complexity of food-related tasks and the constant need to retain and manipulate information about which food products are gluten free or not and which foods they should avoid eating (Wolf et al., 2018).
Unexpectedly, although participants expressed a clear need to prepare before participation in food-related activities, the EF skills of plan/organize and organization of materials did not correlate with the participation variables. For example, “David” and “Rachel’s” profiles show that “Rachel” has significant planning/organizing deficits. However, despite their potential EF deficits in some scales, both example adolescents obtained typical emotional control scores. Emotional control measures the impact of EF problems on emotional expression and assesses the ability to modulate or control emotional responses. There is growing evidence concerning the emotional impact of maintaining a lifelong diet (e.g. Biagetti et al., 2013; Howard and Urquhart-Law, 2014; Skjerning et al., 2014). Possibly, if the emotional control of these two adolescents had been measured alone (thus resulting in typical functioning), their daily struggles to overcome their daily challenges while managing their diet and participating in food-related activities would not have been identified. Future research may add relationships or reasons that shed light on this finding and further the understanding of challenges that those with and without potential EF deficits face.
This study has several limitations. Given the small sample size of the adolescents with potential EF deficits, the findings may not reflect the full range and specificity of executive challenges that adolescents with CD face. In addition, it may be advisable to administer the BRIEF-self-report version (Guy et al., 2004) in future studies that complements the parents’ form because of the importance of using self-report measures for children and adolescents with CD. Additional research that incorporates these assessment tools with a larger sample from multiple populations and centers is recommended. Future studies should explore further which EF components support or restrict the daily functioning of adolescents dealing with CD and how various potential EF deficits health condition.
Conclusion
Given the findings, we recommend considering EF assessment as part of the follow-up evaluation of adolescents with CD to identify EF resourcefulness in the self-management process or potential deficit. Collectively, initiation, shifting, and working memory are among the core skills to decision-making toward solving problems (Dawson and Guare, 2018), and they have a key role in resourceful self-management. The findings are in line with knowledge of the relationships between health behavior and EFs (Reimann et al., 2020). The results highlight specific preliminary relationships between EFs and actions the adolescents took while participating in various food-related activities (CD-Chart), even though the mean BRIEF scores in both groups were within the age-appropriate norm.
Supplemental Material
Supplemental_Table_1 – Supplemental material for Examining core self-management skills among adolescents with celiac disease
Supplemental material, Supplemental_Table_1 for Examining core self-management skills among adolescents with celiac disease by Sonya Meyer and Sara Rosenblum in Journal of Health Psychology
Supplemental Material
Supplemental_Table_2 – Supplemental material for Examining core self-management skills among adolescents with celiac disease
Supplemental material, Supplemental_Table_2 for Examining core self-management skills among adolescents with celiac disease by Sonya Meyer and Sara Rosenblum in Journal of Health Psychology
Supplemental Material
Supplemental_Table_3 – Supplemental material for Examining core self-management skills among adolescents with celiac disease
Supplemental material, Supplemental_Table_3 for Examining core self-management skills among adolescents with celiac disease by Sonya Meyer and Sara Rosenblum in Journal of Health Psychology
Supplemental Material
Supplemental_Table_4 – Supplemental material for Examining core self-management skills among adolescents with celiac disease
Supplemental material, Supplemental_Table_4 for Examining core self-management skills among adolescents with celiac disease by Sonya Meyer and Sara Rosenblum in Journal of Health Psychology
Footnotes
Acknowledgements
We thank the Israel Celiac Association for the assistance provided in recruiting participants and the adolescents and parents for devoting their time. We are grateful to Bar-El gluten-free products and Honigman fashion for donating the gift vouchers given to the participants. We express our appreciation to Sandra Zukerman for her assistance with the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.