
Abstract
Celiac disease (CD) is characterized by clinical polymorphism, with classic, asymptomatic or oligosymptomatic, and extra-intestinal forms, which may lead to diagnostic delay and exposure to serious complications. CD is a multidisciplinary health concern involving general medicine, pediatric, and adult gastroenterology, among other disciplines. Immunology and pathology laboratories have a fundamental role in diagnosing and monitoring CD. The diagnosis consists of serological testing based on IgA anti-transglutaminase (TG2) antibodies combined with IgA quantification to rule out IgA deficiency, a potential misleading factor of CD diagnosis. Positive TG2 serology should be corroborated by anti-endomysium antibody testing before considering an intestinal biopsy. Owing to multiple differential diagnoses, celiac disease cannot be confirmed based on serological positivity alone, nor on isolated villous atrophy. In children with classical signs or even when asymptomatic, with high levels of CD-linked markers and positive HLA DQ2 and/or DQ8 molecules, the current trend is to confirm the diagnosis on basis of the non-systematic use of the biopsy, which remains obligatory in adults. The main challenge in managing CD is the implementation and compliance with a gluten-free diet (GFD). This explains the key role of the dietitian and the active participation of patients and their families throughout the disease-management process. The presence of the gluten in several forms of medicine requires the sensitization of physicians when prescribing, and particularly when dispensing gluten-containing formulations by pharmacists. This underlines the importance of the contribution of the pharmacist in the care of patients with CD within the framework of close collaboration with physicians and nutritionists.
Introduction
Celiac disease (CD) is an immune-mediated systemic disorder triggered by gluten consumption, occurring in genetically predisposed individuals.1–3 Gluten refers to insoluble cereal proteins, including prolamins found in wheat (gliadins), rye (secalins), barley (hordein), and oats (avenins). However, the amino acid sequences inducing CD-associated immune reactions are less prevalent in avenins, which explains the tolerance of small amounts of oats by patients with CD. 4
Unlike CD, recently described gluten sensitivity is characterized by negative serological tests and the absence of villous atrophy, and despite the presence of intestinal or extra-intestinal symptoms, it can be resolved by a gluten-free diet (GFD).5,6
In spite of the classical symptoms strongly suggestive of CD, the last decades have seen the emergence of asymptomatic, oligosymptomatic, or extra-intestinal often misleading forms; hence, the diagnostic delay and the risk of potentially serious complications7–10 can be avoided by implementing GFD.8,11 In addition to medical care for patients with CD, the role of the nutritionist is essential in initiating and adhering to implementing GFD. Physicians and pharmacists often fail to check for gluten when prescribing and dispensing medications; yet, it is frequently a component in the solid phase of certain galenic forms. Therefore, these drugs represent a potential source of hidden gluten. 12
The aim of this review is to shed light on the diagnostic, nutritional, and medicinal aspects of CD with an emphasis on practical issues in the management of celiac patients.
Epidemiological data
The overall prevalence of CD among the general population varies from region to region; it fluctuates between 0.5% and 1% in Europe and North America,6,13,14 and surprisingly ranges from 2% to 3% in Finland and Sweden. 15 High rates are recorded in North Africa, Middle East, and Asia-pacific regions. 16 Similarly, the prevalence of the disease is reported to be high in Arab countries, reaching 3.2% in Saudi Arabia, due to dietary habits such as excessive consumption of barley and wheat, and to a higher frequency of DR3-DQ2 haplotypes. 17 It is probably underestimated in South East Asia and Sub-Saharan Africa, and is almost unknown in many other countries. 18
The disease is more prevalent, with large discrepancies between series in the so called high risk groups, such as type 1 diabetes (1–12%);19,20 auto-immune thyroid disease (2–6%);16,21 Down syndrome (2–6%);22,23 auto-immune hepatitis (3–7%);24,25 Turner syndrome (4–5%);26,27 CD first-degree family members (10–20%);28,29 individuals with iron deficiency anemia (3–15%);29,30 patients with osteoporosis (1–3%), 29 and many other clinical conditions.16,28
In addition, The incidence of CD has significantly increased over the past 30 years, from 2–3 to approximately 9–13 new cases per 100,000 inhabitants per year. 31 This likely reflects a fortuitous discovery of non-classic and asymptomatic forms of the disease through serological testing.10,13,29 Indeed, sero-epidemiological studies suggest that for each diagnosed CD case, there could be 3–7 undiagnosed cases. 32
Immunopathologic aspects
The pathogenic process of CD, as described in Figure 1, takes place in five main steps: (1) the glutamine residues of the ingested gliadin are converted into glutamates by tissue transglutaminase. (2) The modified gliadin is taken up by antigen-presenting cells carrying Human Leukocyte Antigen (HLA)-DQ2 or DQ8, thus activating gliadin-specific CD4+ T cells. (3) These cells produce pro-inflammatory cytokines, such as interleukin (IL)-15, IL-21, and interferon-gamma (IFNγ), and allow specific anti-gliadin and anti-transglutaminase responses. (4 and 5) IFNγ and IL-21 induce a massive release of IL-15, which leads to the proliferation and survival of intraepithelial lymphocytes (IEL), the activation of which alters epithelial cells, thus provoking villous atrophy.7,33

Simplified immunopathological mechanism of celiac disease (adapted from 7 ).
The new face of CD
CD status has gradually changed from a rare enteropathy to a common systemic disease, and as a clinical chameleon, the CD presents in symptomatic, asymptomatic, potential, and refractory forms affecting all age groups. 34
In its classic form, the disease usually starts at the age of 6 months, a few weeks after introducing gluten into the diet. It manifests as chronic diarrhea with abundant stools, accompanied by anorexia and apathy. Other clinical symptoms such as recurrent vomiting, anorexia, chronic constipation, growth or puberty delay, short stature, and irritability, are fairly characteristic and require prompt screening for the disease. 35 Physical examination often shows abdominal meteorism, signs of undernutrition, loss of muscle and fat tissues, a break in the weight curve, and sometimes, slower growth in height. However, non-classic forms are more frequent than classic ones, with extra-intestinal symptoms (Table 1), thus suggesting CD.36,37 Even obese children may have CD, which undoubtedly contributes to the failure and delay of diagnosis. 38

Electroencephalography abnormalities: spike/sharp wave discharges, especially in the occipital lobes and in the central-temporal sites, and in diffuse distribution.
In adults, most patients with CD do not present with diarrhea, but rather “atypical or extra-intestinal” symptoms such as anemia, osteoporosis, dermatitis herpetiformis, abdominal pain, and neurological disorders. 45 Furthermore, in children and adults alike, serological testing should be routinely ordered in the presence of clinical conditions with a high potential for association with CD (Table 1).
The classical forms of CD are characterized by different laboratory findings such as anemia due to iron and/or folate deficiency, hypoprotidemia, hypoalbuminemia, decreased prothrombin time, and vitamin K-dependent factors, and lowered cholesterol mainly related to lipid leakage in the stool.46,47 In fact, biological abnormalities, such as hypocalcemia and hypophosphatemia with decreased alkaline phosphatase owing to vitamin D malabsorption, or hypertransaminasemia, may be the only suggestive signs of CD.48–50
Immunoserological tests
Immunoserological tests are excellent diagnostic and monitoring tools for CD; they allow for the identification of patients at risk of developing the disease, better selection of patients requiring intestinal biopsy, and monitoring adherence to GFD.47,49,51 These tests aim to detect auto-antibodies recognizing two main antigens:
- Transglutaminase 2: targeted by anti-tissue transglutaminase 2 (anti-TG2) and anti-endomysium (EmA) Abs, which are very sensitive and specific for CD.51–54
- Gliadin: targeted by the conventional anti-gliadin Abs, which are now obsolete owing to their low sensitivity and specificity. However, Abs against deamidated gliadin peptides (DGP) perform just as well as anti-TG2.55,56
Immunobiological diagnostic approach
In daily practice, when CD is suspected, whether symptomatic or not, or in high-risk individuals, the first line of screening is based on the detection of IgA anti-TG2, followed if positive by EmA, a highly specific marker, which improves the positive predictive value (PPV) of serological tests.57–60 Indeed, the simultaneous positivity of several tests makes the diagnosis of CD very likely.61,62 In addition, a combination of IgA anti-TG2 with IgG anti-TG2 allows the exclusion of CD potentially occulted by IgA deficiency.57,58,63 Additionally, the PPV of these tests in populations at low risk for CD depends on antibody titers. Low titers (less than three times the cut-off) in asymptomatic patients should be retested after 3–6 months under a gluten-rich diet before considering endoscopy and biopsies.2,57 Moreover, the sensitivity of these tests is lower in children under 2 years of age; therefore, besides IgA anti-TG2, IgA DGP testing is recommended for this age group.39,64
As a reproducible, non-invasive, and highly sensitive test, the salivary anti-transglutaminase testing is a promising screening tool for CD.65,66
Notably, serological tests can be falsely negative in certain circumstances as listed in Box 1.
Possible false negative serological tests in celiac disease. 39

Rapid test screening for CD
Physiologically present in the intracellular compartment of erythrocytes, 67 TG2 made it possible to develop rapid tests based on a chromatographic method using an endogenous TG obtained from the erythrocytes of patients. However, the performance of the rapid tests remains slightly lower than that of serological tests.68,69 Several studies have demonstrated an interest in rapid tests showing a relatively good correlation with whole blood tests, and good positive and negative predictive values for ambulatory CD screening, particularly in the pediatric population. 70 They could, therefore, be used for diagnostic purposes by the physician, even in an office setting. 68
Role of the general practitioner in the management of CD
In their daily practice, general practitioners (GP) often encounter patients with CD, regardless of their location. These doctors must rely on specific diagnostic criteria; however, this is difficult because of the wide range of clinical manifestations that patients present with. 39
GPs must know which serological screening tests to order, how to interpret the results, and which patients are to be referred to a specialist. 39 Thus, according to the diagnostic algorithm proposed in Figure 2, they must refer to a pediatrician or adult gastroenterologist, any patient whose serological tests are positive, for further evaluation.

Immunoserological diagnosis procedure of CD.
Indeed, the presence of specific antibodies in patients with CD-like symptoms is not sufficient to establish diagnosis owing to many clinical and laboratory circumstances (Box 2) mimicking CD.40,71

HLA typing
CD is linked to a strong genetic predisposition, chiefly represented by the HLA-DQ2 and DQ8 systems, which have a high negative predictive value. In fact, less than 1% of patients with CD are negative for both HLA-DQ2 and DQ8, as these are present in approximately 95% and 5% of the cases, respectively, and sometimes both molecules are found in patients.2,72,74 HLA typing cannot be performed as a CD diagnosis tool, since approximately 30–40% of the general population carry HLA-DQ2 and/or DQ8 molecules, and only about 4% of them will develop CD.74–76 On the other hand, HLA-DQ2 and DQ8 typing can be useful when the results of the biopsy are uninformative, or in patients who had initiated GFD on their own prior to serologic testing. CD can also be ruled out in symptomatic patients with negative serological tests as well as in patients considered at high risk, such as first-degree relatives of a patient with CD.74,77
Histopathological diagnosis of CD
Pathologic diagnosis is established or confirmed according to the modified Marsh-Oberhuber and Corazza-Villanacci classifications, with different scales based on the number of intraepithelial lymphocytes, crypt hyperplasia, and villous atrophy78,79 (Table 2). The Corazza score has less variability and benefits from more agreement between pathologists. 77
Summary of the histological classifications commonly used for CD diagnosis. 72

>40 intraepithelial lymphocytes per 100 enterocytes for Marsh Modified (Oberhuber).
>25 intraepithelial lymphocytes per 100 enterocytes for Corazza.
In order to appropriately assess the histological abnormalities of CD according to commonly used criteria, it is recommended to correctly orient the endoscopic sampling (four to six staged biopsies of the bulb and/or the second duodenum) and to repeat levels of biopsy sections. In fact, an imperfectly oriented sample can give a false appearance of villous atrophy (VA).5,80
The major histological criteria of CD include VA of varying degrees with an increased number of IEL. These two signs, although nonspecific, strongly suggest CD and are associated with crypt hyperplasia and increased chorion cell density.81,82 However, VA and increased IEL can be associated with various pathologies, as listed in Box 2. 83 In addition, patients with an isolated increase in IEL with positive serological tests are considered as potential candidates for CD as an asymptomatic latent form, while in the majority of cases, the presence of lonely intraepithelial lymphocytosis does not correspond to CD. 84
On the other hand, almost all VAs associated with IEL, crypt compensatory hyperplasia, chorion hypercellularity (increased density of inflammatory cells and IgA plasma cells), and positive serological tests, correspond to silent forms of CD.81,85
What can we do without the intestinal biopsy?
In children with suspected CD, the current trend is the unsystematic use of intestinal biopsy. 86 Notably, the European Society of Pediatric Gastroenterology, Hepatology, and Nutrition has proposed a biopsy-free approach in symptomatic children meeting the following four criteria: typical clinical signs, anti-TG2 10-fold or more the upper limit of normal (ULN), positive EmA, and positive HLA DQ2 and/or DQ8.87,88
More recently, a group of experts assume that even asymptomatic children can be accurately diagnosed with CD without biopsy, but only on basis of high titers of IgA anti-TG2 (10-fold or more the ULN), positive EmA tests on 2 blood samples. They also consider that HLA analysis is not required for accurate diagnosis. 89 Conversely, intestinal biopsy becomes necessary in the event of clinical manifestations suggestive of CD with negative or discordant serological tests, associated with the positivity of HLA DQ2/8 typing.2,37,90,91 In addition, patients at risk of CD with positive anti-TG2 testing cannot be exempted from the intestinal biopsy. 86 In accordance with the above-mentioned guidelines, Husby et al. 86 highlighted situations where intestinal biopsy is unnecessary to diagnose CD, particularly in children (Figure 3).

Proposal for a CD diagnostic approach to overcome intestinal biopsy in symptomatic children with positive anti-TG2 (TG2-IgA) and EMA testing. In asymptomatic or at-risk children, the positivity of TG2-IgA antibodies should lead to a biopsy and histological analysis. Adapted from. 86
In all cases, the decision to perform or not biopsies in this category should be made collegially with the parent (s) and, if applicable, with the child. 92
In adults, the positivity of serological tests is insufficient to establish the diagnosis of CD, since false-positive cases are frequent in this group. 93 It is, therefore, necessary to complement the serological testing with an intestinal biopsy to confirm the disease before initiating a lifelong GFD.94–96
Diet and gluten-free products
GFD can only be prescribed once the diagnosis of CD has been made with certainty. 97 Rigorous adherence to the GFD results in the absence of functional symptoms within a few days and rapid weight gain. The diet also leads to the decrease or even the disappearance of the VA, thus, avoiding the occurrence of complications. 97
In general, GFD consists of excluding the four categories of cereals that contain gluten and any food derived from them. Patients with CD must, therefore, systematically exclude bread, pasta, pizza, pies, cakes, and other pastries made from wheat flour as well as industrial food products and preparations, whose composition may contain gluten.98,99 Moreover, patients should be encouraged to consume whole grain gluten-free foods (e.g. quinoa, gluten-free oats, and teff) and avoid gluten-free cereals (e.g. white rice and ground corn). 100
The GFD which seems easy in theory, is in fact complicated and difficult to follow, especially in nurseries and schools, restaurants, and even at home. 101 Gastroenterologists, pediatricians, and GPs must therefore convince the patient to follow this diet and emphasize the importance of its lifelong compliance.97,98 In this regard, the involvement of the dietitian in the care of patients with CD is fundamental.
When to refer a patient with CD to a dietitian
After confirmation of CD, the clinical conditions listed below (Box 3) require a systematic referral of the patient to an experienced dietitian as part of a collaborative approach.
Clinical conditions justifying the referral of celiac patient to the dietitian. 100

Role of the dietitian in the care of a patient with CD
The initiation of a GFD should preferably be entrusted to an experienced dietitian who is perfectly familiar with this type of diet that requires clear and detailed explanations, with particular attention to its pitfalls.9,100
During the first consultation, the dietitian explains the GFD and insists on the importance of complete and definitive exclusion of gluten from the diet.97,98
The ubiquitous character of gluten in foods requires providing the patients and their families with the most exhaustive possible list of authorized and prohibited foods. Table 3 presents the main categories of foods containing gluten that the dietitian should explain to the celiac patient and/or to his family.

At the second consultation (scheduled 1 month after the first), the dietitian will answer questions related to any difficulties the patient may encounter, and ensure that a balanced diet is maintained and the weight is regained. The dietitian must also inquire about the social integration of the patient into the new lifestyle, and about the implementation of meals, particularly in nurseries, schools, and in the workplace.
The following consultations are usually coupled with a medical follow-up of the patient at 3 and 6 months, and then once a year. However, they can be more frequent depending on patient needs. 98
To ensure smooth progress of GFD, the dietitian is in charge of educating the patient or his family to:
1- Avoid the risk of contamination by gluten-containing products through the following precautions Gluten-free products should be meticulously separated from those containing gluten, reserving an appropriate space in the pantry and the refrigerator Work surfaces, appliances, toasters or bread makers, cooking utensils, and dishes used to prepare other meals should be thoroughly cleaned before use, or should preferably not be used Frying baths should only be used for breaded products or donuts.97,100,102
2- Read the product labeling carefully:
Patients with CD should be encouraged to routinely read product labels to check for the presence of cereals containing gluten; some ingredients may even change over time. It is also necessary to be vigilant toward foods sold in bulk or catering products.99,103
In addition, terms found on the labels of many products indicate that some ingredients contain gluten and should not be consumed; for example, starch from wheat, barley, rye, or oats; unleavened bread (wheat flour); kamut (ancient wheat), bulgur; malt, and others. A precise list of terms appearing in the composition of a product, which indicate the presence or absence of gluten must also be made available to the patients and their families.4,97,103 A comprehensive list of ingredients and additives that may contain gluten is provided in Table 4, making it easy to identify gluten in food products through their labels.

Medical follow-up for patients with CD
A strict follow-up and a multi- disciplinary approach are needed to ensure harmonious growth and prevent CD-related complications. 38 As summarized in Table 5, the medical follow-up is generally based on clinical evaluation, serological testing, nutritional assessment, bone density measurement, liver and thyroid exploration, intestinal biopsy and cancer screening.
Guidelines for medical monitoring of patients with celiac disease. 40

Patients with CD should be examined at least twice during the first year after diagnosis, to monitor clinical and biological manifestations, nutritional status, body mass index (BMI), serological tests, and to assess compliance with GFD.2,72,74 BMI can be a reliable reflection of the impact of GFD on the nutritional status of celiac patients: underweight patients typically gain weight and overweight or obese patients lose weight. 38 The efficiency of a GFD is thus attested by clinical and biological improvement (1–3 months), the negativity of specific Ab tests, and the regression of histological abnormalities (12 months).3,105,106 Regular monitoring of serology makes it possible to detect diet deviations, whether voluntary or not; and patients whose serological tests do not improve should be reassessed for continued exposure to gluten.40,72,97
One of the most controversial aspects of CD is the value and the timing of the intestinal biopsy when monitoring the disease. To better appreciate the evolution of intestinal damage, a biopsy is generally recommended 1–2 years after GFD initiation. However, intestinal healing is often slow, incomplete, and age-dependent.70,107 Moreover, intestinal biopsy remains essential if symptoms persist. 70
In general, the management of CD must include a nutritional assessment in order to detect deficiencies such as autoimmune thyroiditis (T3, T4, TSH, anti-thyroperoxidase, and anti-thyroglobulin antibodies) and justify replacement therapy (hemoglobin, albumin, calcium, folate, vitamin B12, zinc, magnesium, and vitamin D). 9
It is also recommended to evaluate bone mineral density during the first year of follow-up, using densitometry.9,72
In the pediatric population, the late childhood is particularly critical for the conduct of GFD. In fact, this diet impacts daily life and can be a source of frustration or even depression, and often experienced as “dissocializing,” especially among adolescents.101,108 Closer follow-up by both the specialist and the dietitian is, therefore, necessary to re-explain the disease and its complications, to understand the difficulties of the adolescent in accepting the diet, and to help them overcome social or academic constraints, thus, preventing potential abandonment of the diet. 109
On the other hand, the transition to adulthood is often a period of slackening during follow-up, and sometimes of GFD. Consequently, the orientation toward the adult specialist becomes necessary to ensure continuity in care and avoid the insidious installation of serious complications, mainly, osteopenia and fracture osteoporosis, increased risk of autoimmune diseases (type I diabetes, thyroiditis, and others), hypofertility, or even sterility, neuropathies, and particularly the risk of cancers such as adenocarcinomas and intestinal lymphomas.3,11,108
Medicines are a potential source of gluten concealment, which is commonly introduced into the solid phase of drugs such as tablets and pills when the starch used is extracted from wheat, rye, and/or barley, serving as a diluent or binder.12,103 Starch is also used as a carrier for controlled or sustained-release dosage forms as well as to form nanoparticles, nanogels, and microcapsules. 110 The excipients of some drugs may also contain gluten in small quantities, especially those based on wheat starch, wheat germ oil, wheat bran, wheat flour, barley bran, and vegetable amylase, which can be extracted from barley. 104 The type of excipients can also be different between generic and branded drugs, and those with a known effect (lactose and gluten) must be indicated in the leaflet intended for patients. 111 Thus, even if the brand name is determined to be gluten-free, the gluten-free status of each generic must be verified by the pharmacist and the celiac patient as well.
Unfortunately, drug manufacturers may not disclose the source of the starch used or indicate whether their products are free from gluten contamination. 12 Indeed, all medicines can be made gluten-free since alternatives to starch can be used during production. This highlights the importance of adopting a new policy for the manufacture of gluten-free drugs by pharmaceutical companies and excipient producers. 12
Since 2017, Food and Drug Administration (FDA) has issued a draft guidance on Gluten in Drug Products and Associated Labeling, recommending to drug manufacturers a statement to include in their labeling when truthful and properly supported: “Contains no ingredient made from a gluten-containing grain (wheat, barley, or rye)”. 112
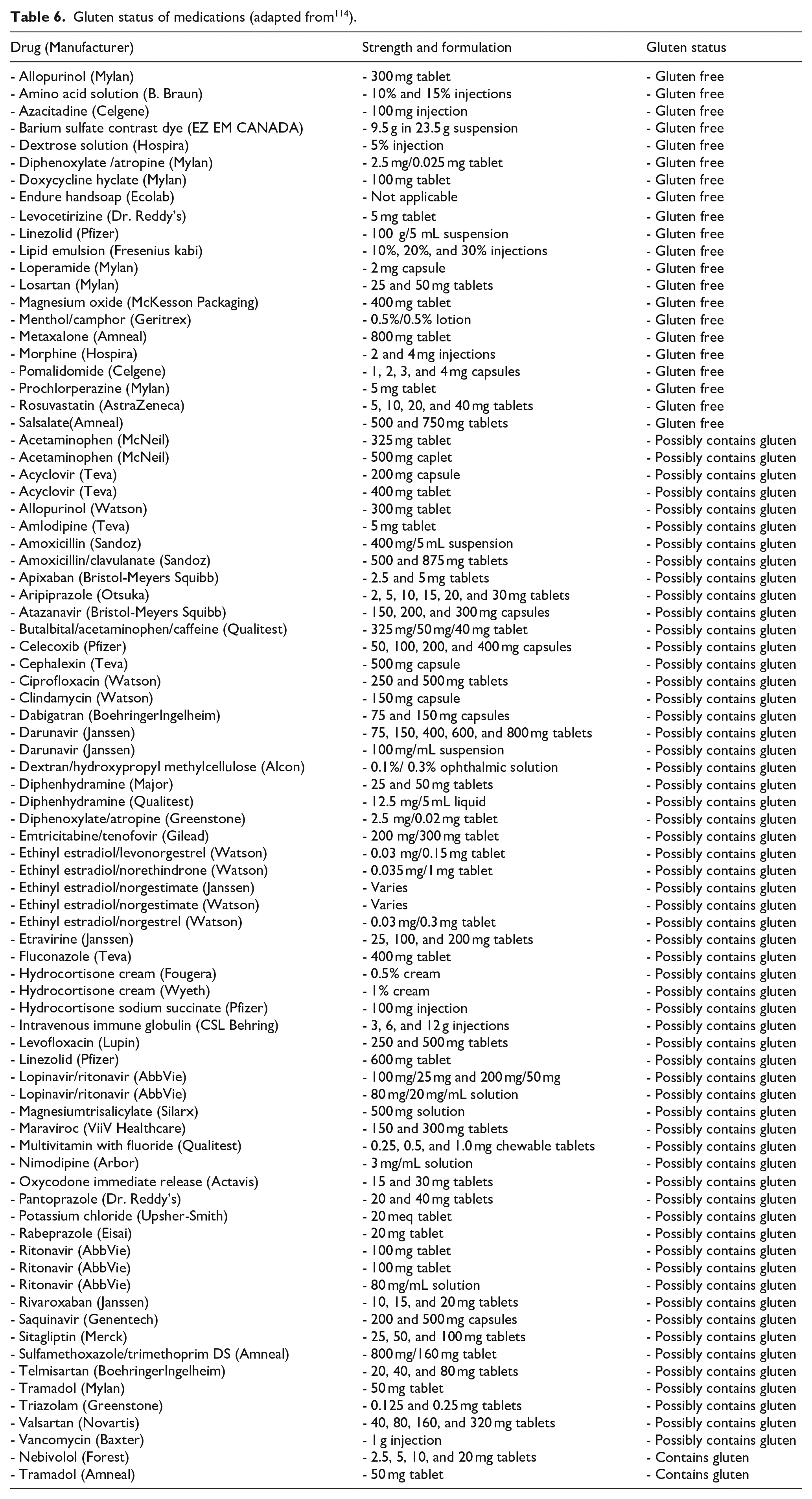
Hence, the pharmacist has an essential role in the management of gluten-intolerant patients. He must check whether the medicine contains gluten, even in very small quantities, especially in excipients. The following components indicate the presence of gluten in the drug: starch, glycerol starch, starch glycolate, carboxymethyl starch, partial hydrolysate of hydrogenated starch, modified/soluble/pregelatinized starch, precooked/processed wheat germ oil, wheat bran, barley, and vegetable amylase. An exception is made for the specialties of Maxilase® or Megamylase® (possibly extracted from barley), which have been authorized by the French association of gluten intolerants after investigations in pharmaceutical laboratories. 113 Box 4 reports a non-exhaustive list of medications containing gluten, drawn from the Vidal dictionary, indicating both the generic and the brand name. A complementary list of drugs that may or may not contain gluten depending on the concentration and formulation of the drug is displayed in Table 6. Indeed, the generic name of drugs may differ depending on the country of origin and distribution. These lists must also be regularly updated with the development of new generic drugs. Thus, both pharmacists and patients with CD should constantly check the composition of the drugs. 113 Determining the gluten status of generic drugs is challenging owing to changes in manufacturers, drug shortages, and wholesale product variability. These factors make identifying the gluten content in generic medications difficult, even for the manufacturers themselves. 114 Additionally, even low gluten intake can irritate sensitive individuals. 104 In contrast, the ointment forms, effervescent tablets, drinkable drops, oral solutions, eye drops, suppositories, nasal drops, and injectable ampoules are gluten-free regardless of the specialty name. 113 Some medications are the only ones to contain the active principle, and the benefit/risk ratio of these drugs must therefore be evaluated by the prescriber before use or exclusion in any therapy.104,114

Gluten status of medications (adapted from 114 ).
To sum up, this overview suggested an integrated approach to the main practical aspects of CD (clinical and laboratory diagnosis; implementation and monitoring of gluten-free diet; delivering and use of gluten-free medications), which represent concerns for physicians, biologists, nutritionists and pharmacists during the process of CD management. However, as limitations, some aspects have not been or insufficiently developed, such as the role of innate immunity in the pathogenesis of CD, the comparative performance of serological testing, the seronegative and refractory CD and possible immunotherapeutic approaches. We have also been faced to the scarcity of scientific data related to drugs and gluten.
Conclusion
Despite its polymorphism with many differential diagnoses, CD benefits from a standardized diagnostic approach based on serology, intestinal biopsy, and possibly HLA typing. The management of CD is a multidisciplinary concern, involving general practitioners, different clinical and biological specialists, as well as dietitians and pharmacists.
The implementation and monitoring of GFD remains a challenge, which reflects the incontestable role of the dietitian as well as that of the pharmacist, considering the risk of the existence or concealment of gluten in the various stages of drug manufacturing.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.