
Abstract
Schizencephaly is an uncommon congenital malformation of the central nervous system. It affects the development of the cerebral cortex. It is characterized by a gray matter–lined cleft filled with cerebrospinal fluid that extends from the pial surface to the ventricle. Types are open and closed lip. Etiology can be due to localized ischemia in periventricular germinal matrix, an extreme variant of cortical dysplasia, and autosomal recessive gene involvement. Age of detection ranges from 8 months to 30 years. Scientific literature regarding the association between schizencephaly and psychosis is scarce. Here, we present the first adolescent case in the literature of a 16-year-old female child with schizencephaly and psychosis.
Introduction
Malformations of the central nervous system are often associated with neurological and psychiatric symptoms. 1 Schizencephaly is a rare congenital disorder with an incidence of 1.54 cases per 100000 births. 2 It is defined as a gray matter–lined cleft filled with cerebrospinal fluid extending from the pial surface to the ventricle. This could be due to abnormal neural migration during the first or second trimester. 1 Subtypes include closed and open lip. Open lip manifests as epilepsy or personality disorder, whereas closed lip is usually asymptomatic. Common etiological factors are localized ischemia in periventricular germinal matrix and extreme variant of cortical dysplasia. Common age of detection ranges between 8 months and 30 years. 3 Here, we present the case of an adolescent girl with closed-lip schizencephaly and psychosis. Previously, very few cases of adolescents with schizencephaly and psychosis have been reported from India, and there are no previous reports from northeast India.
Case Report
A 16-year-old girl, who speaks Bengali, belongs to a low socioeconomic status from a rural background in Assam, and is currently not pursuing formal education, was brought to the outpatient psychiatric clinic. For the past four months, she had been talking and laughing to herself, had not been doing household chores, and had been refusing to take the cows to pasture, which she used to do in the past; she began to have sleep initiation and maintenance difficulties, became dull and withdrawn, and refused to communicate. This was her first episode. When she went out to pasture with the cattle, she would return within an hour or two, sometimes mumbling to herself, and trying to undress when others were present; her mother would instruct her to go into the house to change. These symptoms appeared gradually and were progressive in nature. Her functioning began to deteriorate, so she was brought to our hospital. She never had any mood elation; there were no crying spells, no death wishes, no suicidal thoughts, and no involuntary movements; she did not hear any voices and was not anxious.
Birth and Developmental History
She was the oldest of three siblings. She was born from normal full-term vaginal delivery. The postnatal period was uneventful. There was no history of childhood seizures, jaundice, or chronic illness requiring hospitalization. There was no known history of vaccination. At the age of two or three years, she was noted to hold her right arm in a fixed, flexed position and had difficulty performing some fine motor actions with it, although there were no gross deficits. At about six years of age, she was enrolled in school. She showed poor academic performance and had difficulty writing and speaking. She attended school until the fifth grade, but then dropped out because of her poor performance and because she had to go to a nearby town for high school, to which her parents objected.
After dropping out of school, she helped her mother with the housework. She tended the cattle, cooked, and went shopping to get things. There were no psychiatric or neurological disorders in her family. General physical examination and neurological examination revealed flexed posture of the right arm, with a power of 3/5, hypertonia, brisk reflexes, and impaired functioning. However, in the left arm, bulk, power, tone, and reflexes were normal. Sexual development and secondary sexual characters were appropriate for age.
Mental Status Examination
She was thinly built, partially cooperative for the interview, and partially kempt. She made gaze contact, but it was not sustained. Her speech rate, volume, and tone were low. There was mumbling. However, when asked, she denied having any thought or perceptual disturbances. She described her mood as val lagise (feeling better). Her affect had a flat and narrow range. Her judgment was impaired. Her insight was grade 1; she denied having any problems. The Kiddie Schedule for affective disorders and schizophrenia was used, and the score was 3 for psychosis. Psychological assessment with the Bine–-Kamat test revealed average intelligence.
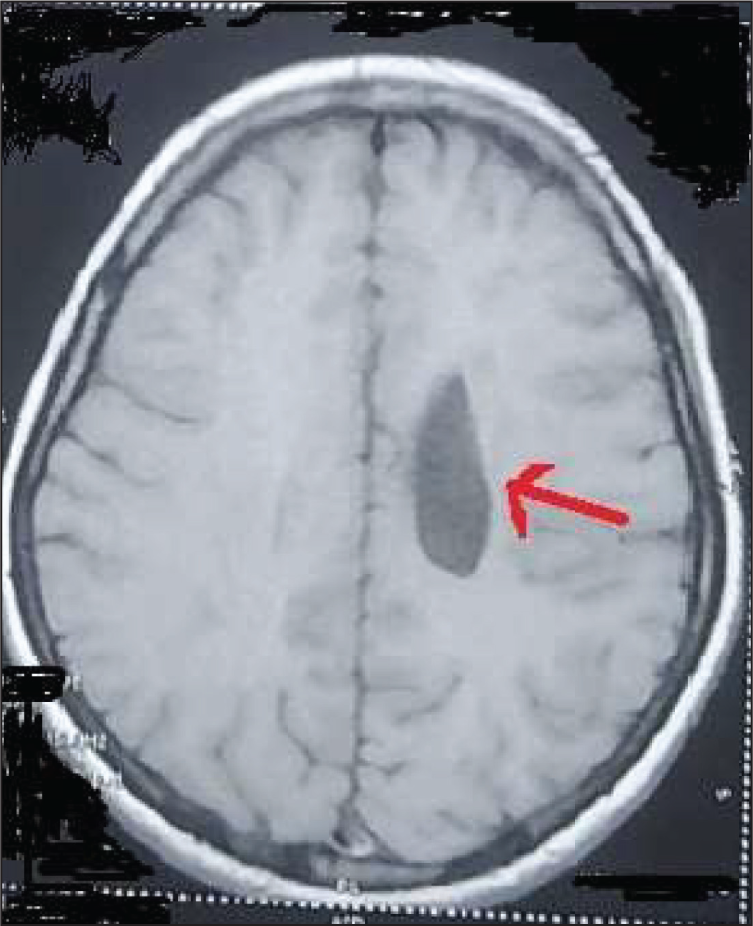
Routine tests such as a complete blood count, renal, liver and thyroid function tests, blood glucose levels, and electroencephalography were normal. Computed tomography of the brain showed some cystic lesions on the left side near the ventricle, and MRI confirmed the cystic lesions as schizencephaly (Figure 1).
Left-sided Closed-lip Schizencephaly.
Diagnosis in accordance with World Health Organization (WHO) multiaxial classification adapted from Rutter 4 was made.
AXIS-1: F06—organic psychosis—secondary to schizencephaly
AXIS-2: F81—mixed disorder of scholastic skills
AXIS-3: No mental retardation
AXIS-4: Q00–Q07—congenital malformations of the central nervous system (schizencephaly)
AXIS-5: No psychosocial problems
AXIS-6: Global assessment of functioning is severely impaired.
The patient was admitted to the ward and received one tablet of olanzapine (5 mg) once daily at night. She also received one tablet of lorazepam (1 mg) at night for sleep. During her stay in the ward, there were no abnormal behaviors and she was cooperative. After one week, her mumbling slowly decreased, and when the examiner questioned her about her behavior, she replied that she did not know the reason. Parents were given psychoeducation about the need for regular follow-up, the nature of the disease, and discharge. She was followed up twice. She showed no behavioral abnormalities and was coping well with the medications. After four months, she was no longer able to follow up. Consent was obtained from her, and the parents also gave their consent for publication of the photograph.
Discussion
Schizophrenia-like psychosis in schizencephaly can be considered as a pathology of neuronal connectivity and heterotopic brain matter, especially if it is in the pathways connecting the frontal and temporal lobes. 2 There may be an underlying ictal phenomenon that leads to psychosis. A few other reports suggest that defective intra-cortical connections and hypofocality in schizencephaly might contribute to psychosis. 5 Dominant hemisphere includes higher-order association areas, which integrate sensory information from different parts of the brain. This information is necessary for the inner representation of the outside world. Hence, when it gets disrupted, psychotic symptoms emerge. 2 In previous reports, lesions were predominantly unilateral but still bilateral distribution was also there. Left-sided lesions were commonly associated with psychosis, whereas patients with right-sided lesions reported mania with psychosis. 6 Involvement of the entorhinal cortex leads to mood disorders. 7 Earlier reports suggest that birth complications, mental retardation, postnatal hyperbilirubinemia, and family history of psychiatric disorders were the most common associations. But these were not present in our patient. Psychotic symptoms such as hallucinations and aggressive behavior were the most common symptoms on admission. Speech difficulties and unilateral or bilateral weakness were the most common deficits associated, and our patient also had unilateral weakness. Onset at puberty, sudden onset of aggressiveness and behavioral abnormalities, and mild weakness of the right upper extremity were the reasons for recommending brain imaging. A review of the literature by Philip Tylis 2 suggested that right-sided lesions presented as chronic psychosis with poor response to antipsychotic agents, whereas left-sided lesions presenting as first-episode psychosis responded satisfactorily to antipsychotics. The response was favorable in our patient too. Schizencephaly must be considered as a differential diagnosis in any patient with early-onset psychosis, seizures, and motor deficits. All cases discussed in the literature responded well to low doses of antipsychotics such as haloperidol, trifluoperazine, and risperidone. In spite of the above-mentioned evidence, we believed that an antipsychotic with sedation and appetite stimulation would be more beneficial for our patient; hence, olanzapine was chosen. This case is a classic example of the two-hit model hypothesis, where a first hit may be a neurodevelopmental defect that increases susceptibility to a second hit, leading to psychosis. 5 The literature search by Pawal et al revealed that only nine cases of schizencephaly with psychosis have been reported to date and three cases were from India. 6 The ages of the Indian cases were 20, 45, and 46 years. However, to our knowledge, this report is the first case of an adolescent from India.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was accorded Ethical Committee Approval with reference number EC/INS/2023-24/020. It was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
Informed assent and consent were obtained from the patient and her parents respectively.