
Abstract
Background:
Electroencephalography (EEG) has been used to research individuals with autism spectrum disorder (ASD). Such individuals are known to have a higher prevalence of EEG abnormalities and seizures. Extended EEG recordings, particularly those including sleep, are known to significantly improve the yield of these abnormalities. However, obtaining extended sleep recordings without sedation in autistic individuals is challenging. This study explores practical and feasible protocols for recording EEG in awake and sleep states in children and adolescents with ASD.
Methods:
Extended EEG recordings using detailed sleep deprivation and recording protocol were done.
Results:
132 children and adolescents with ASD and sleep deprivation completed extended EEG recording in natural sleep. Only nine autistic children required melatonin along with sleep deprivation.
Conclusions:
Extended EEG recording can be achieved by following a rigorous sleep deprivation protocol that is customized, along with providing an autism-friendly recording room environment. This is important in identifying and increasing the yield of epileptiform discharges. We also propose technical guidelines and considerations for EEG recording in children and adolescents with ASD.
Introduction
Children with autism spectrum disorder (ASD) are known to have an increased prevalence of electroencephalography (EEG) abnormalities (30–60%) and seizures (10–30%).1, 2 They also have sleep disorders, behavioral problems, and cognitive deficits. Standard clinical EEG is usually done for a duration of 20–30 minutes, and most studies on ASD also utilize brief, awake EEG recordings. But there is substantial evidence that the yield of epileptiform discharges improves significantly with extended recordings that include sleep state.2–6 However, extended sleep EEG recording in children with low-functioning ASD and multiple medical and neurological comorbidities presents immense practical challenges. These children are restless and frequently have hypersensitivity, which can interfere with EEG lead application and recording. Sleep deprivation is a commonly used method for inducing daytime sleep in children. Medications such as triclofos, chloral hydrate, promethazine, and melatonin have also been used. In this article, we report and recommend practical and feasible protocols for recording EEG in awake and sleep states in children and adolescents with ASD and propose technical guidelines and considerations for this cohort.
Methods
This study was conducted at an advanced center for research that caters to children with ASD and neurodevelopmental disorders in India. Children with ASD who were referred for EEG investigation were included in this report. Institute Ethics Committee approval was taken for the study (IEC No. 379/2021). Data were collected from the EEG recordings that were conducted consecutively for 132 children with ASD between July 2020 and December 2021. Diagnosis of ASD was based on ICD-10 and DSM-5 criteria and confirmed by an expert clinician (child psychiatrist, child psychologist, developmental pediatrician) with more than 10 years of experience working with those who have neurodevelopmental disorders.
EEG recording was done on a 64-channel Philips Geodesic EGI 400 system. The recording was performed with a saline-based net electrode system that can be easily applied in one step (Supporting Figure 1) and conforms to the standard international 10–10 system of electrode placement. The net system of electrodes was chosen to minimize the time needed to initiate the recording in these children, who are usually restless.
Recording duration ranged from a minimum of 60 minutes to a maximum of 180 minutes (median time of 120 mins). This was done to include awake and sleep recordings of EEG. NREM sleep is known to impact the likelihood of seizures and increases the yield of interictal epileptiform discharges as sleep is a state of hyper-synchronization of neural pathways related to sleep. 7 Most children needed between 30 and 60 minutes to fall asleep after initiating recording. The recording ended by 180 mins in almost all cases as the child/adolescent would spontaneously wake up from sleep. All children had a recording of awake and NREM stages 1, 2, and 3 of sleep. All EEGs were reviewed and reported by a neurologist with expertise in epilepsy and clinical neurophysiology.
Details of our “CARE ADD EEG sleep deprivation protocol” are as follows:
The child/adolescent is sleep deprived for at least 4 hours the previous night depending on their usual sleep routine and age (e.g., if a child habitually sleeps at 9 pm and wakes up at 7 am, we would request parents to wake the child up by 3 am). The child/adolescent is engaged in favorite activities early morning, along with 60 minutes of outdoor time (walking/playing in the park). At 8 am, a hot water bath is given. The child/adolescent is well fed 30–45 minutes before the recording. Sleep is avoided during the commute to the hospital. Coffee, chocolate, high-sugar beverages, and other foods that may interfere with sleep are avoided. If needed, a favorite blanket, soft toy, or other play items helpful to facilitate natural sleep are advised to be brought. The person who usually puts the child/adolescent to sleep at home is asked to be present in the recording room. This person (mostly the mother) can also co-sleep on the cot along with them if needed. Some younger children are also breastfed/bottle fed after the application of the net to help them fall asleep. Sometimes, the child’s favorite music/video is downloaded and played. Dim/no light is to be maintained in the recording room. Room temperature is kept between 22 °C and 26 °C to prevent discomfort. Recording usually starts at 9.30 am. If the child/adolescent does not sleep, a break with more outdoor time is given and recording is done after a midmorning snack or after lunch. In younger children who take an afternoon nap routinely, recording is scheduled in the afternoon, after lunch, along with sleep deprivation and active morning hours. If all these strategies fail, tablet melatonin 0.1 mg per kg body weight dose is given as a regular release oral tablet, typically 3–6 mg.
Results
There were 132 individuals with ASD (110 male and 22 female) in the study. The age range was from 2 to 18 years (mean age 6.27, SD 3.46). Children and adolescents were from across the ASD severity spectrum (40% mild ASD and 60% moderate to severe ASD) as measured by the Indian Scale for Assessment of Autism (ISAA), Social Responsiveness Scale (SRS), or Childhood Autism Rating Scale (CARS). As our center is a tertiary care referral center, children are referred by various clinicians across the city for EEG, usually not employing the same assessment tools. The most common indications for EEG included a history of seizures, excessive hyperactivity, significant sleep disturbances, severe behavioral issues, and regression. Six children had a history of regression, and 21 had a history of seizure (Table 1).
Sociodemographic Profile.
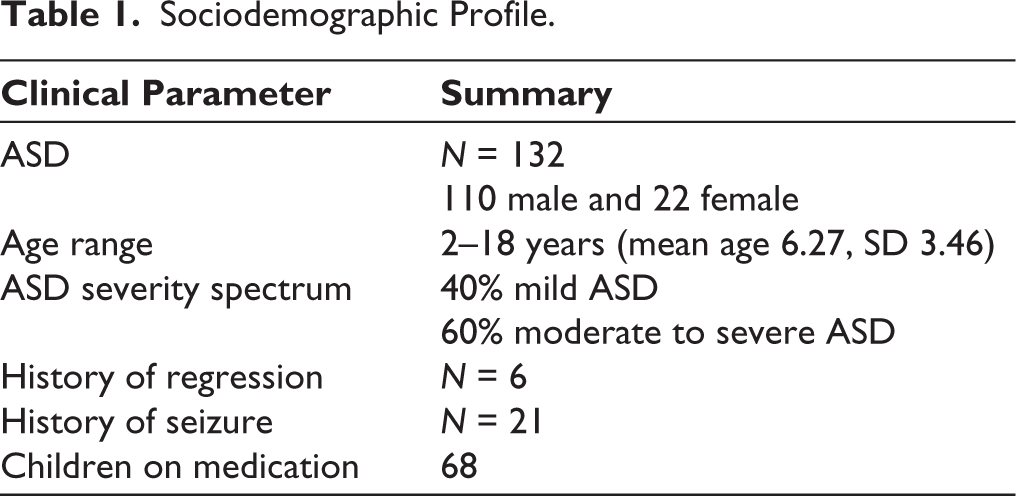
Of the 132 children with ASD, 68 were on medication for other associated behavioral issues and comorbidities. Medications included risperidone, atomoxetine, methylphenidate, clonidine, clobazam, levetiracetam, sodium valproate, clonazepam, and supplements. Patients were advised to continue their regular medications for the procedure.
Of the 132 children with ASD, 123 (93.1%) completed the extended EEG recording in natural sleep after sleep deprivation alone, without the need for medication (Table 2). Of the 132 children, 62 (47%) were given a morning appointment. Of these, 48 completed recording in the morning successfully. Eight children who had a morning slot had to be given a break and needed a full day for the EEG to be completed. Of these 8 children, 6 were given melatonin. Six other children had to be given a reappointment due to a failed attempt on the first day, which was successful on the re-recording day. Of these 6 children, 3 were given melatonin. Seventy (53%) children were given an afternoon appointment for recording. All those 70 children completed the recording successfully. None of the sleep-deprived patients had a seizure or status epilepticus.
Number of Children Who Underwent an EEG and Their Recording Scenarios in the ASD Group.
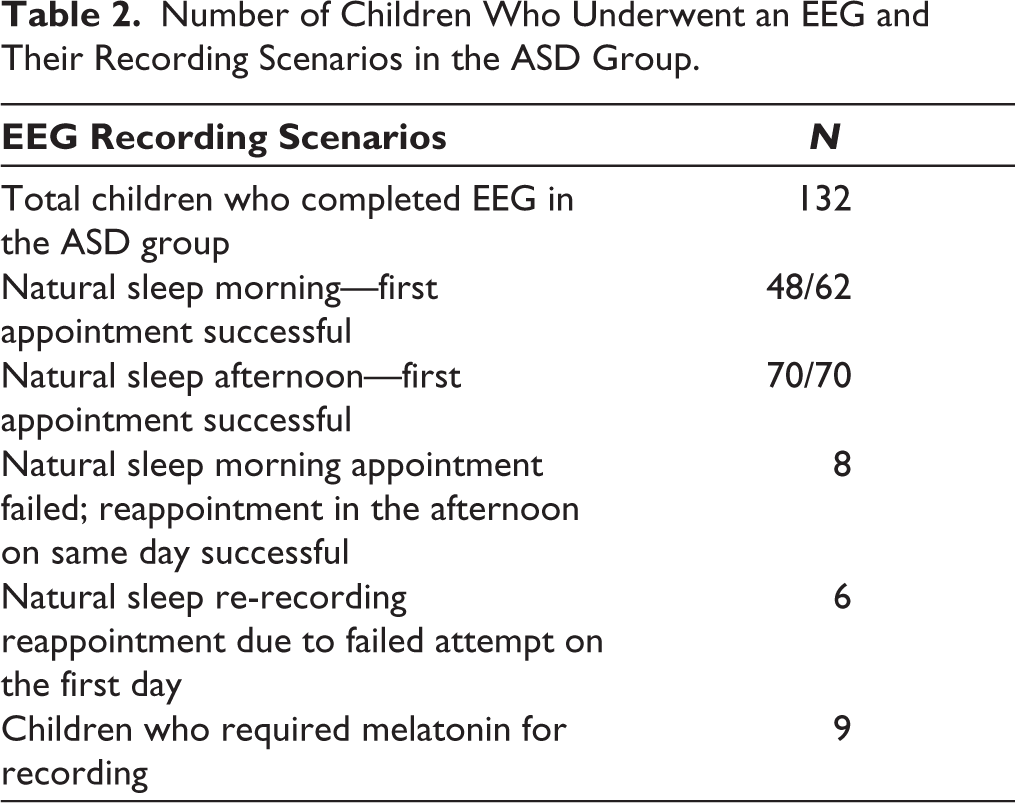
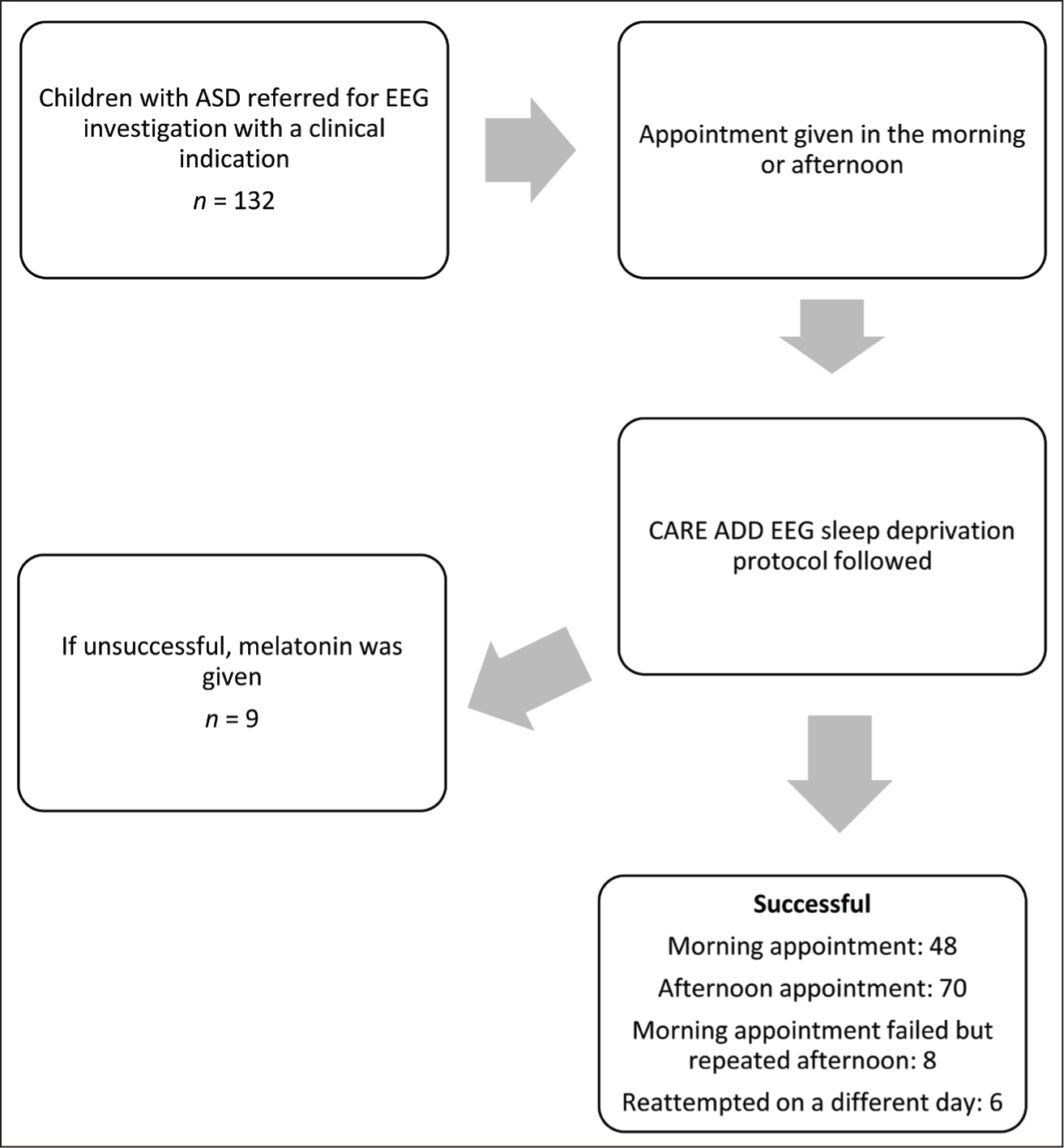
Figure 1 represents the study flowchart.
Study Flowchart.
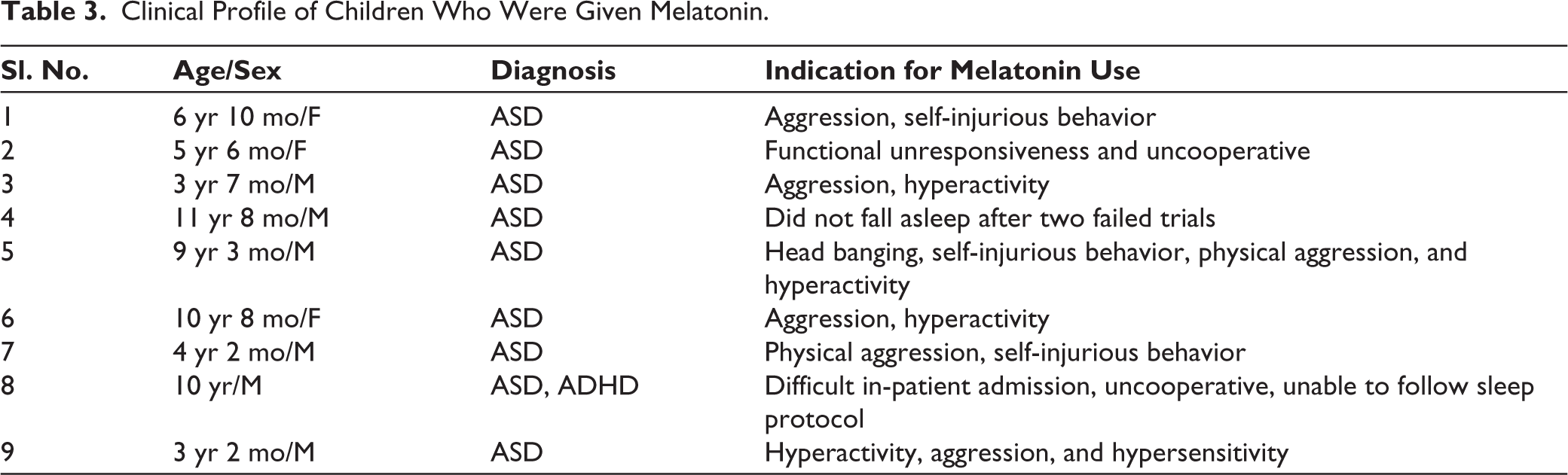
Of the 132 children with ASD, 9 needed melatonin. Most children had one of the following difficulties: significant sensory hypersensitivity to wearing the EEG electrode net, anxiety, and agitated in the recording room; hyperactive, self-injurious behavior and aggression, and could not be otherwise effectively managed in the recording room (Table 3).
Clinical Profile of Children Who Were Given Melatonin.
Of the 132 EEG recordings, 44 (33.3%) were reported as abnormal by the neurologist. Also, 38 children had epileptiform discharges, predominantly posterior quadrant (occipital-parietal and posterior-temporal) and 4 children had interhemispheric asymmetry. Of the 44 children with abnormal EEG, 28% had ASD with a history of epilepsy and 72% had ASD without epilepsy. During the awake state, only 15% of the 44 children had epileptiform discharges, and in the additional 85%, epileptiform discharges were only seen in stages 1 and 2 of NREM sleep. In one child who had ASD with cerebral palsy and epilepsy, along with occasional spikes in awake EEG, a CSWS/ESES pattern was seen in sleep. Once IEDs were detected, all children were referred back to the clinical team for further evaluation and management. Children with frequent IEDs were started on anti-epileptic drugs. Others were managed with behavioral therapy or relevant interventions depending on the clinical history and indication for EEG.
Discussion and Implications
In our study, extended sleep EEG in children with ASD was feasible with sleep deprivation alone in the vast majority (93.1%) using the protocols and techniques described above. Also, EEG abnormalities were similar to those reported by other studies on ASD with and without clinical epilepsy.1, 5, 8
Use of net electrodes, which can be quickly applied, greatly facilitated this process. With the traditional disc electrodes, the usual application time would have been 15–20 minutes. As the latency to sleep onset is as long as 60 minutes, patience and commitment on the part of the technician and the EEG team are crucial. We showed that even if one recording session fails, it is still possible to obtain a spontaneous sleep record with a second session. This is probably due to anxiety and sensitivity to the new, closed space and a different-than-usual recording environment. Scheduling the recording at noon from the outset may be less time consuming and more successful in obtaining spontaneous sleep EEG.
Persistent efforts to get sleep recordings are important because a substantial proportion (33.3% in this cohort) of these extended sleep recordings yielded significant abnormalities, mainly epileptiform discharges. However, this extended protocol is time consuming and limits the number of EEGs done each day.
Occasionally (in 5% of children), melatonin was required especially in the presence of sleep disorders, sensory issues, rigidity, poor adaptability, and severe behavioral issues where natural sleep could not be easily induced in the hospital settings. Our experiences with melatonin use were similar to those in the literature,5, 9 but this study was not designed to compare melatonin versus spontaneous sleep EEG.
Overnight recordings are recommended as ideal to identify epileptiform discharges in ASD and increase yield. 8 Though this is a limitation of our study, in clinical and research settings predominantly with children with moderate to severe ASD, and high patient load, it is not feasible to do overnight EEGs as a routine for these children. Our protocol allowed us to record spontaneous sleep EEG, which is superior to the conventional 20-minute recordings.
To the best of our knowledge, though there are natural sleep protocols for MRI recording in ASD,10–12 similar protocols have not been described for extended natural sleep EEG recordings in ASD in the literature. Such guidelines and protocols are important for centers that cater to these specific clinical populations.
Conclusion
To conclude, we propose the following guidelines on technical considerations and indications for EEG recording in children with ASD:
Children and adolescents with ASD and severe hyperactivity, behavioral issues, sleep disorders, and neuro-regression may be considered for EEG recording even in the absence of clinical seizures. The likelihood of identifying epileptiform discharges in this group is high. EEG recording must include sleep state to increase the yield of epileptiform discharges and, in some cases, an ESES/CSWS pattern. Either spontaneous sleep or melatonin-induced sleep may be acceptable for clinical purposes. For research purposes, spontaneous sleep is preferred to eliminate the confounding effect of medication. For spontaneous sleep records, scheduling the procedure at noon rather than in the morning is more likely to be successful. Using net electrodes is preferable to using disc electrodes to minimize the application time. The duration of the recording is 2–3 hours to ensure that adequate sleep stages are recorded. The sleep deprivation and recording protocols described above were successful in our experience. These may be considered by other labs with modifications suitable to their setting.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The study was accorded Ethical Committee Approval vide Ethics Committee of St. John’s Medical College Hospital No. 379/2021 dated October 28, 2021. The study was carried out in accordance with the principles as enunciated in the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written or verbal audio-recorded informed consent was taken from all the participants.