
Abstract
X-linked adrenoleukodystrophy (ALD) is a demyelinating neurodegenerative disease of the brain with neurological manifestations in the majority of cases. However, a small proportion of cases also present solely with psychiatric symptoms. Here, we discuss the case of a 13-year-old boy presenting with mood symptoms, behavioral changes, and cognitive impairment. A neurodegenerative disease was suspected based on the atypical findings in history and abnormal neurological examination. Neuroimaging and pathogenic variations in the ABCD1 gene confirmed the diagnosis. Thorough history and detailed examination remain the cornerstone in arriving at the right diagnosis, aided by need-based advanced investigations.
Introduction
Leukodystrophies are inherited disorders of the white matter in the brain characterized by demyelination and variable clinical presentation. X-linked adrenoleukodystrophy (ALD) is characterized by progressive demyelination and adrenocortical insufficiency. The fatty layer (myelin) that protects nerves in the brain and spinal cord tends to degrade in this ailment (a condition called demyelination). The childhood cerebral form of XL-ALD typically occurs in 1 in 21000 boys between the ages of 4 and 10 years, and the most common neurological symptoms are dementia and behavioral changes. 1 Cerebral ALD (CALD) is caused by a mutation in the ABCD1 gene on the X-chromosome and affects 35%–40% of boys with ABCD1 gene mutation. Since the mutation is carried on the X-chromosome, girls are highly unlikely to manifest CALD. Boys with CALD begin showing symptoms between the ages of 4 and 10 years, symptoms primarily being behavior problems, aggression/withdrawal, poor memory, academic decline, and difficulty reading, writing, and understanding speech. A gradually progressive condition may lead to vision problems, seizures, deafness, poor coordination, etc. 1 Psychiatric signs and symptoms as the initial manifestation of ALD are less commonly seen. These may range from behavioral changes, learning difficulties, developmental issues, personality changes to anxiety disorders, hallucinations, and cognitive impairment. We discuss the case of a boy with neuropsychiatric manifestations of XL-ALD.
Clinical Case
A 13-year-old boy presented to the child and adolescent psychiatry outpatient department (OPD) of a tertiary care teaching institute with complaints of academic decline and hyperactivity for four years. He was second in birth order, born to nonconsanguineous parents with uneventful antenatal period and a history of smooth perinatal transition. There was no family history of psychiatric and neurological disorders. He met age-appropriate milestones, and there Were no problems reported during the early stages of his development. Further, detailed psychiatric evaluation revealed that his interaction with family members was gradually decreasing from nine years of age. He refused to go to school, became irritable, and cried if persuaded. Few days later, he revealed that a few older schoolboys were forcing him into oral and anal sexual activity for the past few weeks. For the next two to three weeks, he appeared sad and repeatedly told his parents that the boys had wronged with him, but he could not fight back. His parents talked to school authorities and changed his school. They also filed a police report but struck a compromise and did not proceed with legal procedures. He started to visit the new school and appeared better, but gradually over the next few months, he stopped showing interest in academics and refused to read and write. He did not play with his elder brother at home nor sit at one place and kept roaming about all over the house. Parents had to persuade him to do activities of daily living, and he got irritable when asked to do any minor household chores. He started copying the scenes and dialogues from movies he watched during those days. He would jump on the furniture, as if copying action scenes. He failed in grade 4 but was unconcerned. His teachers informed that in class he did not sit, read, or write and did not even interact with other children. By 10 years of age, he was seen to be masturbating multiple times a day, at times even in front of family members. He watched pornographic content on the phone and did not stop even when scolded. He also started to demand items like rifles and told his parents that he would become a don and kill all bad people. He told his cousins that he will help them if they are in any trouble and seemed to be rather boastful. He became defiant and hit and abused family members without any remorse. He was seen to behave weirdly by sitting with dogs outside his home, talking to them, or throwing stones at them. If people from the neighborhood stopped him from doing so, he abused them as well. On a few occasions, he set clothes and bedsheets on fire but did not accept that he did any wrong despite being punished by parents. He was also seen to be eating more than usual and demanded food items frequently. During the night, he was observed to be pacing in the house and had difficulty in initiating as well as maintaining sleep. However, he would be energetic all day and would not get tired even after sleeping less than his usual self. During the COVID-19 pandemic lockdown and thereafter, the above-mentioned issues kept on escalating day by day. He discontinued studies completely, and whenever he was forced to read or write, he made a lot of mistakes as if he had forgotten everything and was not able to understand any subject. He also lost 4–5 kg of weight despite eating more food.
A detailed developmental history revealed that he would toe-walk intermittently during early childhood, but it was never considered a problem by the family members and, thus, was never evaluated. However, the family recalled that since his behavioral problems had increased, they saw him walking on toes more often. Academically, he had been an average student until four years, when a gradual disinterest was noted along with associated decline and behavioral changes thereafter.
The interview and mental status examination showed that he was engaging in reciprocal interaction although his activity levels were increased and had an inappropriate affect. He was constantly smiling and picking the skin of his toes and putting it in his mouth. His speech was clear and coherent, but his comprehension was poor and he gave irrelevant answers and had impaired higher mental functions in terms of immediate/remote memory, comprehension, concrete thinking, and judgment, with poor insight.
He had an average IQ of 72 on the Malin’s Intelligence Scale for Indian Children (MISIC; verbal quotient 72 (ranging between 68 in digit span and 77 in comprehension); performance quotient 71 (ranging between 68 in block design and 75 in picture completion)), which did not correspond to his earlier academic performance. A neurological examination revealed bilateral lower limb spasticity, hyperreflexia, ankle contractures, and diplegic gait. He had normal anthropometry, no neurocutaneous markers or organomegaly, and a normal fundus. Rest of the systemic examination was within normal limits.
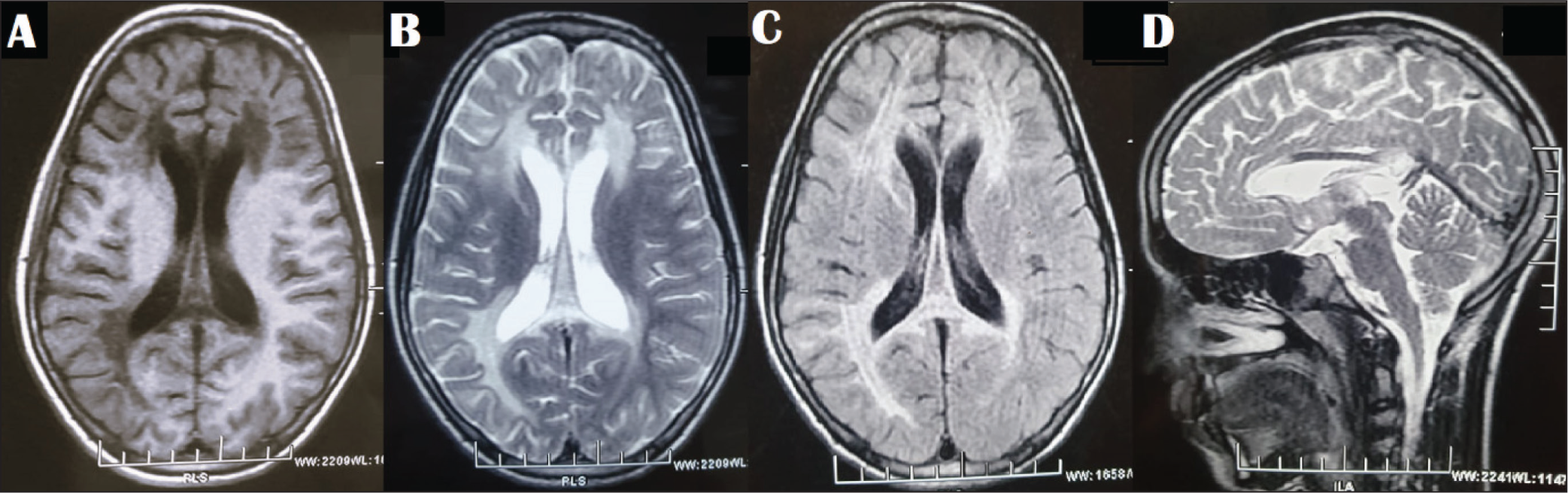
Based on the information available and the physical and neurological examination, a provisional clinical diagnosis of spastic diplegia secondary to a static insult (may be hypoxic ischemic insult) in the perinatal period with mood disorder (i.e., mania-like symptoms) and borderline intellectual functioning was considered, but it necessitated etiological workup for the neurological findings. Oral olanzapine (2.5 mg/day) was started for behavioral disturbances. Blood investigations (hemogram, renal function test, liver function test, and thyroid function test) were within normal limits except vitamin D level, which was deficient and for which vitamin D supplementation 60,000 IU weekly for eight weeks was advised. MRI brain revealed symmetric, signal changes in the periventricular and subcortical white matter in the bilateral frontoparietal and right temporo-occipital areas and genu and splenium of the corpus callosum (Figure 1A–D). A diagnosis of leukodystrophy such as X-linked adrenoleukodystrophy (XL-ALD) and late-onset metachromatic leukodystrophy was considered. Clinical exome analysis revealed a hemizygous 3′ splice site variant in the intron 8 of the ABCD1 gene. A final diagnosis of ALD with neuropsychiatric manifestations and past history of depressive disorder was considered. Psychoeducation of family members regarding nature, course, and prognosis of XL-ALD was done and olanzapine continued. The patient was again referred to pediatric genetics and pediatric neurology for further investigations and management; however, since the family members understood that the condition had no treatment and could not be reversed, they dropped out of follow-up without visiting any of the departments. They were contacted telephonically when they informed that they were taking homeopathic treatment for his condition and did not wish to come back.
Magnetic Resonance Imaging of the Brain (A) T2; (B) FLAIR Sections Showing Hyperintensities in the Periventricular and Subcortical White Matter in Bilateral Frontoparietal and Right Temporo-occipital Regions; (C) T1 Section Showing Hypointense Signal in the Same Areas, and (D) T2-sagittal Section Showing Involvement of the Genu and Splenium of the Corpus Callosum.
Discussion
Our case highlights the psychiatric presentation of XL-ALD, which slowly progressed to involve cognition and behavior. The cerebral form of XL-ALD should always be considered in a boy with new-onset neurobehavioral or neuropsychiatric presentation. Psychiatric symptoms include mania, psychosis, anxiety disorders, personality changes, hyperactivity, and cognitive impairment. 2
While analyzing the case, we noted that, although there was an underlying undiagnosed neurological condition, the psychiatric symptoms in the form of a depressive illness developed after the occurrence of the trauma of sexual abuse. During that period, his cognition and behavior were understood to be associated with the trauma. Later, he developed manic symptoms, which persisted too long, and this clinical picture merged with cognitive decline. Thus, an independent depressive disorder in the past with neuropsychiatric manifestations (manic symptoms, cognitive decline, disorganized behavior) of XL-ALD was considered as the final diagnosis.
The history of sexual abuse and the psychological reaction to it, followed by gradual cognitive decline and behavior changes, complicated the case conceptualization and dissuaded the authors to understand it as solely a neuropsychiatric presentation of XL-ALD. But a relatively long history of four years, gradually deteriorating and progressive behavioral changes, cognitive decline and physical examination findings of bilateral lower limb spasticity, hyperreflexia, ankle contractures, and diplegic gait raised concerns about the presentation being something more than a pure psychiatric illness. MRI brain findings of periventricular and subcortical white matter changes raised the suspicion of an underlying leukodystrophy, which was further confirmed by genetic testing.
The treatment of psychiatric symptoms is complicated by atypical or no response to the psychotropic medications and treatment emergent adverse effects in patients with neurometabolic disorders. However, a thorough knowledge of the drugs being prescribed and an understanding of the primary disorder, particularly the ways in which it might render the patient vulnerable to certain side effects, is helpful.
To summarize, careful history taking and thorough physical examination are important tools in the armamentarium of medical professionals, enabling picking up of seemingly rare cases in routine psychiatry outpatients. Presence of atypical psychiatric symptoms, neurological signs/symptoms, academic decline, and recent onset behavioral disturbances not better explained by nosological diagnostic entities should raise the suspicion for underlying organic pathology and should be corroborated by appropriate investigations and specialist referral. However, keeping the patient in the treatment loop still remains a challenge especially when families have to be informed about the poor prognosis and non-curable nature of the condition.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent and Ethical Approval
Informed consent was taken from the parents for publication of this case report. Adequate precaution has been taken to mask the identity of the patient.