
Abstract
Background
Purpurin are naturally occurring anthraquinones derived from the roots of Rubia species. Purpurin is a red-colored bioactive compound commonly used as a food colorant. In ancient times, Rubia species plants were used in Chinese medicine to treat rheumatoid arthritis. Research studies have proven purpurin exerts antimicrobial, neuromodulatory, antigenotoxic, anti-inflammatory, anticancer, and antioxidant effects. The present investigation was proposed to evaluate the efficacy of purpurin against myocardial infarction in rats.
Materials and Methods
Purpurin was pretreated in healthy adult male rats and subjected to a myocardial infarction with isoproterenol to assess the cardioprotective effect of purpurin. CRP, total protein, and uric acid levels were quantified to analyze the efficacy against myocardial infarction. Cardiac functional markers and antioxidant levels were measured to evaluate the role of purpurin on isoproterenol-induced myocardial infarction. Further to prove the cardioprotective efficacy of purpurin cardiac tissue ATPases and electrolytes were assessed in the experimental animals. The anti-inflammatory property of purpurin was analyzed by quantifying proinflammatory cytokines. Histopathological analysis of cardiac tissue was to confirm the protective effect of purpurin against isoproterenol-induced myocardial infarction.
Results
The present investigation demonstrated the significant protective effect of purpurin by decreasing the levels of CRP, uric acid levels, and total protein levels in myocardial infarction-induced rats. It restored the cardiac functional markers and glutathione system in the cardiac tissue of myocardial infarction-induced rats. It increased the levels of cardiac ATPases and reinstated the electrolytes in the cardiac tissue of myocardial infarction-induced rats. Purpurin significantly demonstrated an anti-inflammatory and cardioprotective effect that was evidenced with histopathological analysis.
Conclusion
Our findings prove purpurin suppresses the proinflammatory response of isoproterenol treatment and exerts a cardioprotective effect in myocardial infarction-induced rats.
Introduction
Cardiovascular disease (CVD) is an umbrella term for heart and circulatory diseases, which includes myocardial infarction, stroke, ischemic heart disease, cardiomyopathy, and atherosclerosis (Lindstrom et al., 2022, pp. 2372–2425). Previously, CVD tended to be prevalent in the geriatric population; due to the changes in lifestyle, socio-economic, behavioral, and environmental and behavioral changes younger population is also now prone to CVD. Hypertension, hyperchlosterol, and obesity were commonly associated with increased risk in cardiac patients. Worldwide for the past few decades, CVD has been the leading cause of mortality. About one-third of global deaths are reported to occur due to CVD, and about 20.5 million mortalities were registered in 2021 alone (Tsao et al., 2022, pp. e153–e639).
Myocardial infarction that is often referred to as a heart attack develops due to the obstructive blood flow to the myocardium. The coronary blockade causes ischemic tissue necrosis and cardiac muscle degeneration (Zhang et al., 2023, p. 131). Cardiac tissue undergoes extensive remodeling in post-myocardial infarction attacks affecting the function of the heart (Pluijmert et al., 2020, p. 16601). Hyperlipidemia, oxidative stress, inflammation, and plasma membrane integrity depletion are the pathogenesis of myocardial infarction (Pullaiah et al., 2021, p. 43). Past two decades advancement in the pharmaceutical field had declined the 1-year mortality rate of myocardial infarction, but no improvement was observed in the 5-year survival rate. Beta-blockers, vasodilators, acetylcholine esterase (ACE) inhibitors, anticoagulants, and calcium channel blockers were prescribed to treat myocardial infarction. Even though these treatments had brought moderate success, side effects were observed on long-term medication (Machaj et al., 2019, pp. 147–155).
Phytodrugs, such as aspirin, digoxin, ephedrine, lovastatin, and reserpine, are proven to be effective in treating vascular disease. Bioactives possess multiple cellular mechanisms of action that ameliorate hypertension and artherosclerosis causing myocardial infarction (Gao et al., 2012, pp. 3–10). These phytodrugs are not only potent but also cost-effective alternatives to allopathic drugs. The bioactive components in phytodrugs effectively treat disease without causing side effects even in long-term medications (Tabassum & Ahmad, 2011, pp. 30–40). Pupruin, anthraquinone naturally occurs in the roots of Rubia cordifolia, a perennial herb widely distributed in Europe, Africa, and Asia (Singh et al., 2021, pp. 2418–2428). Purpurin possesses immense pharmacological properties like neuromodulatory, antioxidant, anti-inflammatory, and antigenotoxic. It is used to treat traumatic bleeding, amenorrhea, hematemesis, pain, swelling, and so on (Kim et al., 2022, pp. 2580–2592; Nam et al., 2017, p. E265). In the present investigation, we evaluated the cardioprotective effect of purpurin in rats-induced myocardial infarction with isoproterenol.
Materials and Methods
Experimental Animals
The current investigation was performed with healthy adult albino Wistar rats. The rats were procured from the institutional animal facility after obtaining ethical clearance from the institutional ethics committee. The rats were housed in a clean polypropylene cage bedded with rice husk. Before initiation of the experiment, the rats were acclimatized for a period of 10 days in the laboratory condition maintained at 25 ± 2°C room temperature, 55 ± 5% relative humidity, and 12 h light/dark cycle. Rats were fed with a laboratory rat pellet diet and water ad libitum. Only the experimental procedures approved by the ethical clearance were performed, and the rats were treated with utmost care and concern.
Experimental Design
The acclimatized rats were grouped into four groups, each group consisting of six rats. Group I rats were treated orally with olive oil. Myocardial infarction was induced in Group II rats that were treated subcutaneously with 85 mg/kg of isoproterenol on the 29th and 30th days of the experiment. Groups III and IV were orally pretreated with 25 and 50 mg/kg bwt of purpurin for 28 days and subjected to myocardial infarction on the 29th and 30th days of the experiment.
On the completion of the treatment period, the rats were anesthetized, and using a capillary tube, the blood was drawn from the retro-orbital plexus. The rats were sacrificed, and the whole heart was surgically excised and cleansed with 0.9% cold saline.
Measurement of Body and Organ Weight
The body weight of the experiment animals was measured at the end of the treatment period before sacrificing the animals. The heart of the experimental animals was surgically excised, cleansed with saline, dried with tissue, and weighed using a digital weighing machine.
Biochemical Estimation
The total protein level in the serum of the experimental rats was quantified using Bradford Assay Kit, Thermo Fisher Scientific, USA. C-reactive protein and uric acid levels were estimated with ELISA and colorimetric kits were procured from Merck, USA. The experiments were performed in triplicates, and the levels were identified with a standard curve plot drawn with the OD value of known standard concentrations.
Quantification Cardiac Function Markers
Myocardial tissue homogenate was prepared with 0.1 M ice-cold phosphate buffer, pH 7.4. The tissue was homogenized and centrifuged at 12,000 × g for 20 min at 4°C. The supernatant was collected and utilized for analysis. Cardiac functional markers creatine kinase (CK), alanine transaminase (ALT), aspartate transaminase (AST), and gamma-glutamyl transferase (GGT) were quantified in both serum and heart tissue homogenate of the experimental rats using the commercially available ELISA kit, Abcam, USA. The assay was done as per the instructions provided by the supplier.
Assessment of Cardiac Glutathione System
The levels of glutathione S-transferase (GST), glutathione peroxidase (GPX), and reduced glutathione (GSH) were quantified in the heart tissue of experiment rats. A colorimetric assay kit procured from Merck was used to detect the levels of GST, GPX, and GSH. GST was estimated based on the reaction of the GST enzyme between GSH and the GST substrate, CDNB. The GST activity is measured at 340 nm, and it is directly proportional to the rate of increase in absorbance. GPX was measured by the NADPH consumption in the enzyme-coupled reaction. A decrease in the OD value at 340 nm was observed, which was directly proportional to the GPX activity. GSH levels were measured with the DTNB method, and the absorbance was measured at 412 nm which was directly proportional to the enzyme activity.
Quantification of Cardiac Tissue ATPase
Cardiac tissue sodium-potassium (Na+/K+), magnesium (Mg2+), and calcium (Ca2+) adenosine triphosphatases (ATPases) were quantified in the experimental rats. The ATPase levels were estimated with the commercially available kits procured from MyBiosource, USA. The experiment was done as per the instruction of the supplier and the levels.
Quantification of Electrolytes
The major electrolytes sodium, potassium, and calcium were measured in the serum of the experimental animals. The electrolytes were detected using the commercially available colorimetric kit, Elabscience. The assay was done as per the kit manual, and the final absorbance was measured at 405 nm for sodium, 450 nm for potassium, and 610 nm for calcium.
Detection of Proinflammatory Cytokines
Proinflammatory cytokines tumor necrosis factor (TNF)-α and interleukin (IL)-6 were quantified in the serum and cardiac tissue of the experimental animals using the ELISA kit purchased from Thermo Fisher Scientific, USA. Standard and the samples were added to the appropriate wells and incubated on a shaker at room temperature for 90 minutes. The solution was discarded and washed with wash buffer, and then the biotin conjugate was added for 60 minutes. The biotin conjugate was discarded, the streptavidin HRP solution was added, and incubated at room temperature for 45 minutes. The plates were washed, and the TMB substrate was added for 30 minutes. Finally, the reaction was stopped by the addition of the stop solution. The final absorbance of the sample was read at 450 nm, and the levels of inflammatory cytokines were calculated with a standard plot curve.
Histology
Histopathological changes in the cardiac tissue of the experimental rats were analyzed with hematoxylin and eosin staining techniques. The tissues were fixed with 10% neutral formalin and subjected to tissue processing with a series of alcohol. The processed tissue was embedded in paraffin wax and subjected to microtome tissue sectioning. Five micron-thickness tissue sections were stained with hematoxylin and eosin under the light microscope and assessed by a blindfolded pathologist.
Statistical Analysis
The data obtained were statistically examined using the software SPSS version 17.0. One-way analysis of variance (ANOVA) followed by Tukey test was performed, and the data were finally represented as mean ± standard deviation (SD) of triplicates. p < 0.05 was considered to be statistically significant.
Results
Effect of Anthraquinone Purpurin on Body Weight and Organ Weight
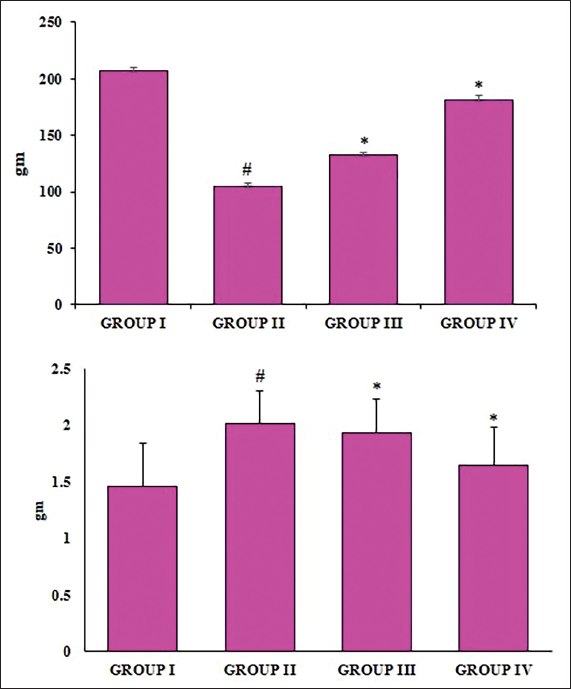
The change in the body and heart weight of the myocardial infarction-induced and purpurin-pretreated animals were examined, and the results are illustrated in Figure 1. A significant reduction in body weight was observed in the myocardial infarction-induced purpurin untreated rats compared to the control rats. Purpurin-pretreated rats showed a significant increase in body weight compared to the myocardial infarction-induced purpurin untreated rats. Heart weight was significantly increased in the myocardial infarction-induced rats, whereas purpurin-pretreated rats showed a significant reduction in heart weight. Compared to low-dose purpurin pretreated rats high-dose purpurin rats showed a significant increase in body weight and decrease in heart weight.
Effect of Anthraquinone Purpurin on Body Weight and Organ Weight. Data were Analyzed with One-way Analysis of Variance (ANOVA) Followed by Tukey Test, and the Data were Finally Represented as Mean ± Standard Deviation (SD) of Triplicates. p < 0.05 was Considered to be Statistically Significant. #Control vs Myocardial Infarction Induced, *Myocardial Infarction Induced vs Purpurin Pretreated Rats.
Effect of Anthraquinone Purpurin on Biochemical Parameters
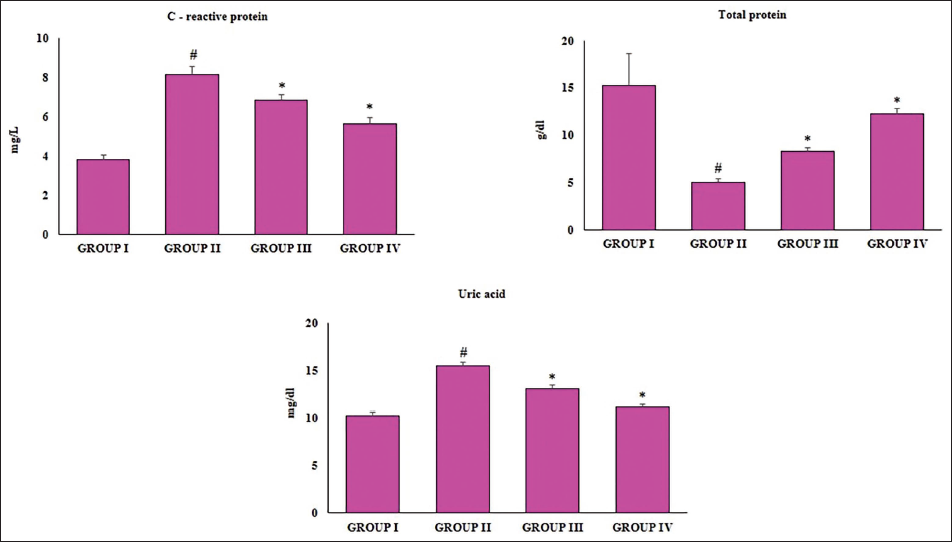
Figure 2 depicts the effect of purpurin on biochemical parameters of control, myocardial infarction-induced, and purpurin-pretreated rats. The hs-C-Reactive protein and uric acid levels were significantly increased in the ISO-treated myocardial infarction-induced rats compared to the control rats. Purpurin treatment significantly decreased the levels of C-reactive protein and uric acid in myocardial infarction-induced rats. The reduction in C-reactive protein and the uric acid in purpurin-treated rats was observed in a dose-dependent manner. The total protein levels were significantly decreased in the ISO-treated myocardial infarction-induced rats compared to the control rats. Both low- and high-dose purpurin pretreatment showed a significant increase in the levels of total protein.
Effect of Anthraquinone Purpurin on Biochemical Parameters. The Total Protein Level in the Serum of the Experimental Rats was Quantified using the Bradford Assay Kit, and C-Reactive Protein and Uric Acid Levels were Estimated with ELISA and Colorimetric Kits. Data were Analyzed with One-way Analysis of Variance (ANOVA) Followed by Tukey Test, and the Data were Finally Represented as Mean ± Standard Deviation (SD) of Triplicates. p < 0.05 was Considered to be Statistically Significant. #Control vs Myocardial Infarction Induced, *Myocardial Infarction Induced vs Purpurin Pretreated Rats.
Cardioprotective Effect of Anthraquinone Purpurin on Cardiac Function Markers
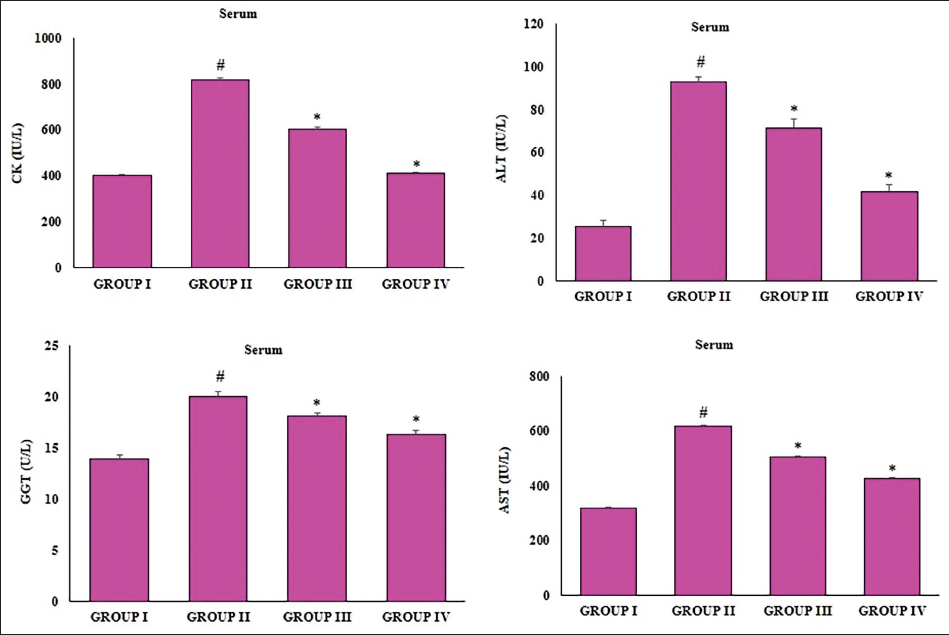
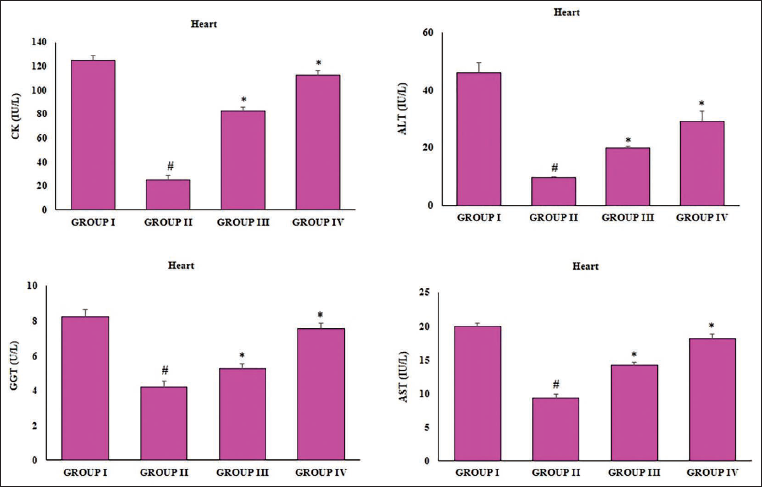
The cardioprotective effect of anthraquinone purpurin on the ISO-treated myocardial infarction-induced rats was assessed, and the levels are represented in Figures 3 and 4. Cardiac functional markers CK, ALT, AST, and GGT were quantified in both serum and heart tissue homogenate. Compared to the control rats the levels of CK, ALT, AST, and GGT were significantly increased in the serum and decreased in the heart tissue of the ISO-treated myocardial infarction-induced rats. Purpurin pretreatment suppressed the effect of ISO and significantly decreased the levels of cardiac function markers in the serum (Figure 3). Increased levels of cardiac functional marker levels were found in the cardiac tissue (Figure 4) of purpurin-pretreated rats compared to untreated myocardial infarction-induced rats.
Cardioprotective Effect of Anthraquinone Purpurin on Cardiac Function Markers in the Serum. Cardiac Functional Marker Levels in Serum were Quantified Using the ELISA Technique. Data were Analyzed with One-way Analysis of Variance (ANOVA) Followed by the Tukey Test, and the Data were Finally Represented as Mean ± Standard Deviation (SD) of Triplicates. p < 0.05 was Considered to be Statistically Significant. #Control vs Myocardial Infarction Induced, *Myocardial Infarction Induced vs Purpurin Pretreated Rats.
Cardioprotective Effect of Anthraquinone Purpurin on Cardiac Function Markers in the Cardiac Tissues. Cardiac Functional Marker Levels in Cardiac Tissue were Quantified using the ELISA Technique. Data were Analyzed with One-way Analysis of Variance (ANOVA) Followed by Tukey Test, and the Data were Finally Represented as Mean ± Standard Deviation (SD) of Triplicates. p < 0.05 was Considered to be Statistically Significant. #Control vs Myocardial Infarction Induced, *Myocardial Infarction Induced vs Purpurin Pretreated Rats.
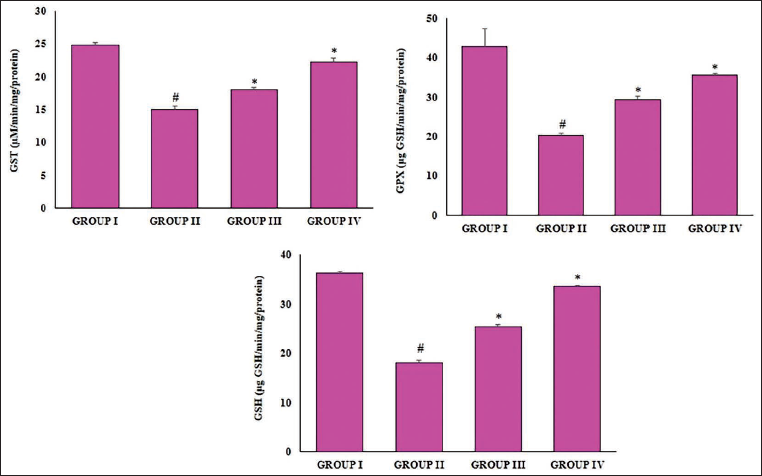
Antioxidant Effect of Anthraquinone Purpurin
The antioxidant system plays a key role in cardiac protection; therefore, the levels of GST, GPX, and reduced GSH were quantified in the heart tissue of experiment rats (Figure 5). The control rats showed 18 ± 0.9 units/protein of GST 58 ± 1.3 units/protein of GPX and 29 ± 0.8 units/protein of GSH, whereas it significantly decreased to 10 ± 0.3 units protein of GST, 37 ± 1.5 units/protein of GPX, and 12 ± 0.6 units/protein of GSH. A dose-dependent increase in GSH levels was observed after purpurin pretreatment. 14 ± 0.6 and 16 ± 0.8 units/protein of GST, 42 ± 1.3 and 48 ± 1.1 units/protein of GPX, and 17 ± 0.8 and 24 ± 0.7 units/protein of GSH levels were observed in 25 and 50 mg/kg purpurin pretreated rats, respectively.
Antioxidant Effect of Anthraquinone Purpurin. The Levels were Measured in Cardiac Tissue with Commercially Available Colorimetric Kits. Data were Analyzed with One-way Analysis of Variance (ANOVA) Followed by Tukey Test, and the Data were Finally Represented as Mean ± Standard Deviation (SD) of Triplicates. p < 0.05 was Considered to be Statistically Significant. #Control vs Myocardial Infarction Induced, *Myocardial Infarction Induced vs Purpurin Pretreated Rats.
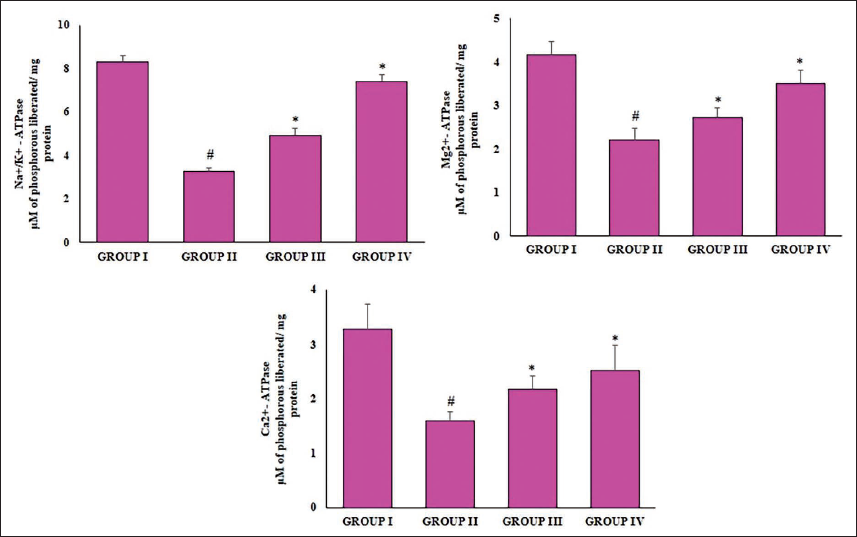
Effect of Anthraquinone Purpurin on Cardiac Tissue ATPase
Figure 6 illustrates the levels of cardiac tissue Na+/K+, Mg2+, and Ca2+ ATPases in the experimental rat. Isoproterenol treatment significantly decreased the Na+/K+ ATPase to 2.2 ± 0.05, Mg2+ ATPase to 2.9 ± 0.03 and Ca2+ ATPase to 0.7 ± 0.01 units/mg protein, whereas the control rats showed Na+/K+ ATPase to 5.8 ± 0.06, Mg2+ ATPase to 4.8 ± 0.08, and Ca2+ ATPase to 3.4 ± 0.07 units/mg protein. Pretreatment with purpurin significantly increased the levels of all the three ATPases. The increase in ATPase was observed in a dose-dependent manner; 25 and 50 mg purpurin treatment showed 3.4 ± 0.08, 5.1 ± 0.02 units/mg protein of Na+/K+ ATPase, 3 ± 0.04, 3.8 ± 0.01 units/mg protein of Mg2+ ATPase, and 1.5 ± 0.08 and 2.6 ± 0.06 units/mg protein of Ca2+ ATPase, respectively.
Effect of Anthraquinone Purpurin on Cardiac Tissue ATPase. The ATPase Level in the Cardiac Tissue of the Experimental Rat. The ATPase Levels were Estimated with the Commercially Available Kits. Data were Analyzed with One-way Analysis of Variance (ANOVA) Followed by Tukey Test, and the Data were Finally Represented as Mean ± Standard Deviation (SD) of Triplicates. p < 0.05 was Considered to be Statistically Significant. #Control vs Myocardial Infarction Induced, *Myocardial Infarction Induced vs Purpurin Pretreated Rats.
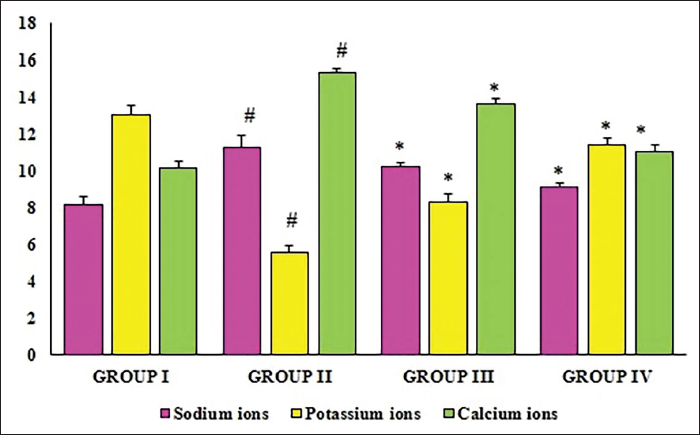
Effect of Anthraquinone Purpurin on Electrolytes
The major electrolytes sodium, potassium, and calcium were measured in the serum of the experimental animals and were quantified, and the results are depicted in Figure 7. The sodium and calcium ions were increased in the serum of myocardial infarction-induced rats compared to the control rats. Purpurin pretreatment significantly decreased the levels of sodium and calcium ions in dose-dependent manner. Purpurin pretreatment significantly increased the potassium ions compared to the myocardial infarction-induced rats.
Effect of Anthraquinone Purpurin on Electrolyte Levels. The Electrolyte Levels were Measured in the Serum of the Experimental Animals. The Electrolyte Levels were Estimated with the Commercially Available Kits. Data were Analyzed with One-way Analysis of Variance (ANOVA) Followed by Tukey Test, and the Data were Finally Represented as Mean ± Standard Deviation (SD) of Triplicates. p < 0.05 was Considered to be Statistically Significant. #Control vs Myocardial Infarction Induced, *Myocardial Infarction Induced vs Purpurin Pretreated Rats.
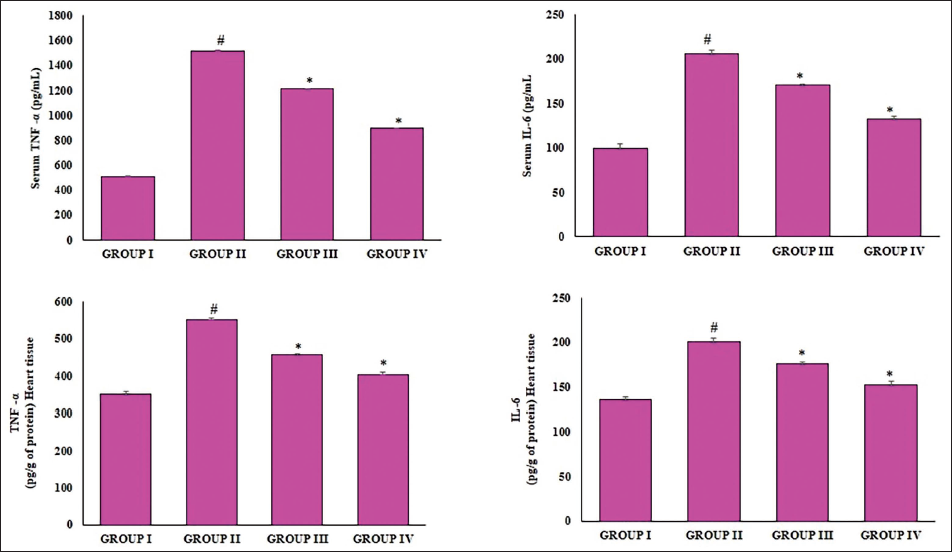
Anti-inflammatory Effect of Anthraquinone Purpurin
Figure 8 represents the levels of proinflammatory cytokine in the experimental rats. Isoproterenol treatment induced myocardial infarction in the rats, which was evidenced by an increase in proinflammatory cytokines TNF-α and IL-6 levels. The proinflammatory cytokines were significantly increased in both the serum and cardiac tissue of the experimental rats. Prupurin treatment significantly suppressed the inflammatory response induced by the isoproterenol and reduced the proinflammatory cytokines TNF-α and IL-6 levels in dose dose-dependent manner.
Anti-inflammatory Effect of Anthraquinone Purpurin. The Cytokines Level in the Serum and Cardiac Tissue of the Experimental Animals Using the ELISA Kit. Data were Analyzed with One-Way Analysis of Variance (ANOVA) Followed by Tukey Test, and the Data were Finally Represented as Mean ± Standard Deviation (SD) of Triplicates. p < 0.05 was Considered to be Statistically Significant. #Control vs Myocardial Infarction Induced, *Myocardial Infarction Induced vs Purpurin Pretreated Rats.
Cardioprotective Effect of Anthraquinone Purpurin
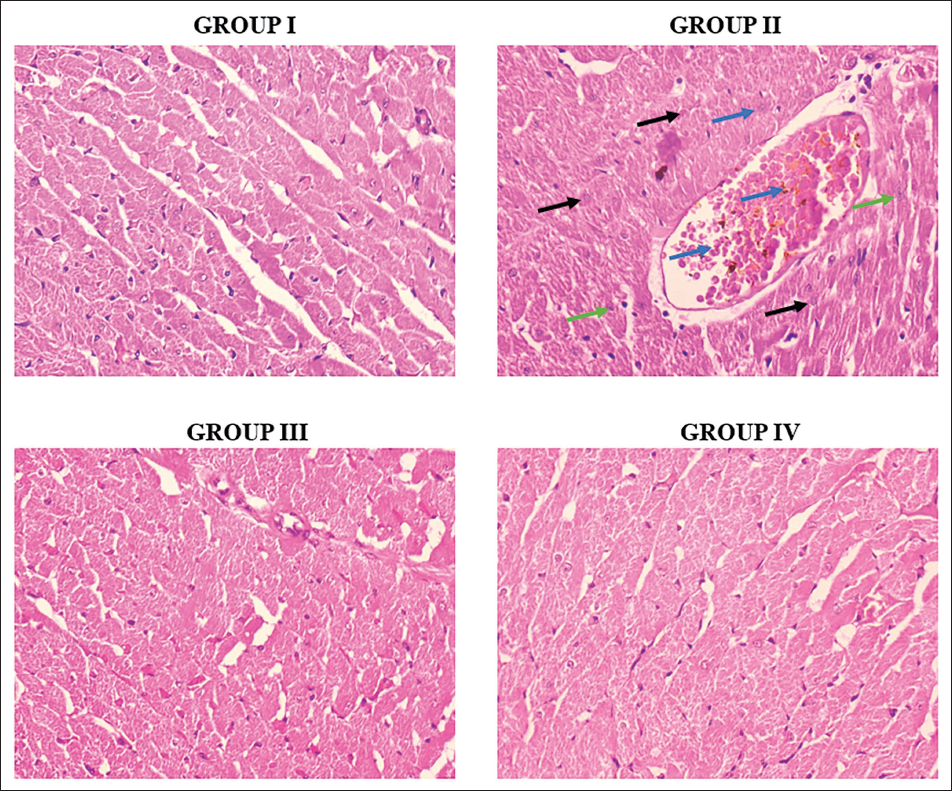
Olive oil-treated control rats showed normal cardiac tissue histoarchitecture with no edema or inflammatory cells, whereas the isoproterenol-treated cells showed infiltered inflammatory cells, necrotic cells, and signs of edema were observed (Figure 9). Compared to the myocardial infarction-induced rats, the purpurin pretreatment showed decreased necrotic cells, inflammatory cells, and decreased edema. 50 mg/kg bwt purpurin pretreated rats showed decreased myocardial tissue inflammation compared to the 25 mg/kg bwt purpurin pretreated rats (Figure 9).
Cardioprotective Effect of Anthraquinone Purpurin. Group I: Control, Group II: Myocardial Infarction Induced, Group III: 25 mg/kg bwt Purpurin Pretreated Myocardial Infarction Induced, and Group IV: 50 mg/kg bwt Purpurin Pretreated Myocardial Infarction Induced. Black Arrows: Inflammatory Cell Infiltrations; Blue Arrows: Myocardial Necrosis; Green Arrows: Myocardial Edema. The Cardiac Tissue of the Experiment Rats was Subjected to Hematoxylin and Eosin Staining. Representative Images of Hematoxylin and Eosin (H&E) Stained Cardiac Tissue Sections of Experimental Rats.
Discussion
CVD is one of the predominant diseases, attributing 40% of noncommunicable disease mortality. In the year 2019, about 17.9 million deaths were reported globally, which accounts for 32% of total global mortality. Myocardial infarction and stroke account for 85% of cardiovascular-induced mortalities. Obstructive blood flow to the heart causes biochemical alteration, lipid peroxidation, and antioxidant and ATPase depletion, which in turn leads to irreversible cardiac tissue damage (World Heart Report, 2023). Hence, treating patients with myocardial infarction tends to be a greater challenge for medical professionals all around the world. The present study was designed to evaluate the efficacy of a phytodrug purpurin against myocardial infarction induced in rats.
Myocardial infarction in rats was induced with isoproterenol, a synthetic β-adregenic agonist that causes alteration in the biochemical, functional, and histology of the rat’s cardiac tissue (Gupta et al., 2024, pp. 123–136; Rhana et al., 2022, p. 175134). Isoproterenol accelerates the synthesis of free radicals and calcium, dysregulates the cell metabolism, and alters the electrolytes and membrane permeability, thereby causing energy and oxygen depletion in the cardiac tissue (Angelovski et al., 2023, pp. 1–17). Myocardial necrosis induced by isoproterenol in animal role resembles the myocardial infarction pathology in humans (Wei et al., 2017, pp. 2007–2016). Isoproterenol-induced rats showed acute electrocardiographic and hemodynamic alterations that were like the myocardial infarction patients. Therefore, isoproterenol is a reliable myocardial infarction animal model that can be utilized to assess the cardioprotective effect of bioactive compounds (Khalifa et al., 2022, p. 174978). In the present study, isoproterenol-treated rats also showed biochemical and histopathological alterations that confirm the induction of myocardial infarction.
A dense microvascular system and increased interstitial flow rate cause the myocardium to be susceptible to edema formation. Myocardial edema is a pathological observed after a myocardial infarction attack. It is a predominant factor that induces damage to the cardiomyocytes and causes cell dysfunction, and remodeling (Vasques-Nóvoa et al., 2022, pp. 958–976). Hence, in the present investigation, we measured the body weight and heart weight of the experimental animals. Isoproterenol treatment significantly increased the heart tissue weight, confirming the induction of myocardial edema and it also decreased the body weight of the animals. But purpurin pretreated rats showed significantly decreased edema and increased body weight proving the cardioprotective effect.
C-reactive protein is a downstream marker during the acute phase of inflammation, and it is elevated in patients suffering from myocardial infarction (Reindl et al., 2017, pp. 640–649). High sensitivity C-reactive protein was reported to be elevated after myocardial infarction and tends to be at peak for the next 72 h. Uric acid, a purine metabolite product, also appeared to be elevated in patients with hypertension, stroke coronary heart disease (Dao Bui Quy et al., 2021, p. e17900). The increase in serum uric acid levels was directly proportional to the mortality rate of myocardial infarction patients (Rahimi-Sakak et al., 2019, p. 218). Purpurin pretreatment significantly decreased the myocardial infarction biomarkers hs-CRP, uric acid, and total protein in myocardial infarction-induced rats, which was found to be increased in purpurin-untreated myocardial infarction-induced rats.
During hypoxia conditions, the cardiac tissue membrane permeability gets dysregulated and releases enzymes such as CK, alanine aminotransferase, aspartate aminotransferase, and g-glutamyl transferase. These enzymes were found to be increased in the serum and decreased in the cardiac tissue, which is directly proportional to the necrotic cells. CK is a key biomarker for the diagnosis of acute myocardial infarction. The levels of CK, particularly the isoenzyme CK-MB, were observed to be elevated in the serum and decreased in the myocardium infarction cardiac tissue (Aydin et al., 2019, p. 218). Abnormal ALT/AST ratio was often observed in myocardial infarction patients. GGT activity is strongly correlated with the development of cardiovascular morbidity and mortality (Djakpo et al., 2020, pp. e279–e283). Hence, we quantified these biomarkers in the serum and the cardiac tissue of the experimental rats. As per the previous reports, the levels of CK, AST, ALT, and GGT were significantly increased in the serum and decreased in the cardiac tissue of the myocardial infarction-induced rats. Whereas the purpurin pretreatment significantly inhibited the isoproterenol-induced hypoxia condition thereby protecting myocardial cells from necrosis.
Cardiomyocytes are mitochondrial-rich cells that require immense energy and are prone to oxidative damage. Endogenous antioxidants, especially enzymatic antioxidants, play a vital role in oxidative stress-induced myocarditis (Tan et al., 2023, p. 131). The glutathione system including enzymes GPX and GPX effectively detoxifies xenobiotics and protects the cardiovascular system (Jaganjac et al., 2020, p. 1151). Kim et al. (2022, pp. 2580–2592) reported that purpurin exerted an antioxidant effect against cerebral ischemia in the gerbil hippocampus. It also downregulated the inflammasome formation via scavenging oxidative stress, thereby preventing cancer cell formation (Singh et al., 2021, pp. 2418–2428). In our study, purpurin-pretreated rats showed increased levels of glutathione later than the myocardial infarction.
The prime function of Na+/K+-ATPase in eukaryotic cells is to maintain the plasma membrane Na+ and K+ gradients. It regulates the cytosolic Na+ concentration and Na+/Ca2+ exchanger (NCX), thereby causing excitation and contraction in cells. Particularly in cardiomyocytes, it impacts the cytosolic Ca2+ levels to induce contraction of cells. Inhibition of Na+/K+-ATPase in cardiomyocytes increased the cytosolic calcium transients, cardiac output, and myocyte contraction. The dysregulated Ca2+ and Na+ transport occurs due to disturbance in Na+-K+ ATPase, causing loss of K+ and gain of Na+ by the cell (Cellini et al., 2021, pp. H650–H662). Purpurin pretreatment significantly increased the Na+/K+, Ca2+, and Mg2+ ATPase and decreased the sodium and calcium levels in the cardiac tissue of myocardial infarction-induced rats. It also increased the potassium levels, which confirms that purpurin treatment inhibited the isoproterenol-induced ATPase dysregulation in the cardiac tissue of rats and prevented the rats from myocardial infarction.
Inflammatory response occurs post-acute myocardial infarction and determines the size of infarct in cardiac tissue. The insistent synthesis of proinflammatory cytokines later in the myocardial infarction causes the remodeling of cardiac tissue, making it have key target for therapeutic drugs (Ong et al., 2018, pp. 73–87). Therefore, in the current investigation, we analyzed the anti-inflammatory role of purpurin on pleiotropic proinflammatory cytokines TNF-α and IL-6. TNF-α binds with its receptor and induces the secretion of apoptotic proteins, thereby promoting ventricular remodeling in myocardial conditions. It also stimulates the excessive accumulation of calcium, oxy radicals, and oxidoreductase in cardiomyocytes, which leads to cardiomyocyte necrosis (Wróbel-Nowicka et al., 2024, p. 760). Elevated levels of IL-6 in serum were observed in injured tissue for several weeks. In myocardial ischemia conditions during reperfusion, cardiomyocytes release increased levels of IL-6, which induces the neutrophils to synthesize ICAM-1, which damages the myocardial tissue (Martins et al., 2022, p. 2371). IL-6 elevation in cerebral ischemia rat model and CSF of stroke patients correlates with the volume of the infarct (Lazzarin et al., 2022, p. 2064). In our study, the isoproterenol treatment increased the levels of TNF-α and IL-6 in the serum and cardiac tissue of the rats. This may be the reason for infiltered inflammatory cells, necrotic cells, and signs of edema observed in the cardiac tissue of the myocardial infarction-induced rats. Purpurin effectually inhibited the secretion of both TNF-α and IL-6, thereby preventing cardiac tissue damage in rats treated with isoproterenol.
Conclusion
In summary, the results of our evaluation showed shown pretreatment with purpurin ameliorates myocarditis in myocardial infarction-induced rats. Purpurin significantly decreased the hs-CRP and uric acid levels and restored the cardiac functional markers and GSH system in the cardiac tissue of the myocardial infarction-induced rats. It also elevated the cardiac ATPases, K+, and inhibited the Na2+ and Ca2+ levels, thereby preventing excessive contractions in the cardiac tissue of myocardial infarction-induced rats. Purpurin, a potent anti-inflammatory drug, significantly decreased the levels of proinflammatory cytokines, thereby preventing cardiac tissue damage, which was evidenced by histopathological analysis. On the whole, our results prove that purpurin possesses a cardioprotective effect in rats, which can be subjected to further research to be formulated as a drug.
Summary
Hypertension, hyperchlosterol, and obesity were commonly associated with increased risk of CVDs.
Myocardial infarction, often referred to as heart attack, develops due to the obstructive blood flow to the myocardium.
Purpurin showed an anti-inflammatory and cardi oprotective effect in isoproterenol-induced myocardial infarction in rats.
Footnotes
Abbreviations
ACE: Acetylcholine esterase; ALT: Alanine transaminase; AST: Aspartate transaminase; ATPase: Adenosine triphosphatase; CK: Creatine kinase; CVD: Cardiovascular disease; GGT: Gamma-glutamyl transferase; GPX: Glutathione peroxidase; GSH: Glutathione; GST: Glutathione S-transferase.
AAcknowledgments
None.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
The experimental protocol for this study, was reviewed and approved by the Ruijin Hospital Animal Ethical Committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.