
Abstract
Rates of cerebral venous sinus thrombosis (CVT) misdiagnosis or at times delayed diagnosis and related outcomes have remained underexplore, and also there is less knowledge about the long-term outcome of patients with untreated cerebral venous sinus thrombosis (CVT). Long-term presentations of untreated CVT are rare. We hereby presenting series of four interesting patients of chronic CVT whose diagnosis was missed and how varied chronic presentations of untreated CVT appeared to neurology and how subtle radiologic features helped with correct diagnosis.
Introduction
Cerebral venous channel thrombosis (CVT) is one of the less suspected causes of stroke in young adults (mean age in the third decade with female accounting for two-thirds female preponderance) 1 constituting around 0.5%–2% of all stroke cases.2, 3 Complete or incomplete blockage of the major cerebral venous channels or the less common smaller feeding cortical veins involvement is the cause for thrombosis. In one autopsy series, venous thrombosis incidence is around 9.3% 4 suggesting that it might often be missed in life. If treated early, venous thrombosis has a much favorable prognosis. 5
Its varied but atypical clinical manifestations often result in misdiagnosis and makes delay in early diagnosis leading to potentially fatal consequences. Chronic CVT presentation is varied from intracranial hypertension to space occupying lesion (SOL) such as presentation and refractory epilepsy. In recent years, neuroimaging use has markedly reduced the misdiagnosis and missed cases. Magnetic venography (MRV) of cerebral veins remains the gold standard investigation of choice and very few require somewhat invasive Digital subtraction angiography (DSA). The author intents to analyze the delayed, missed, and disguised presentation of chronic CVT undergoing various referral, which delayed the timely treatment and lending into some non-reversible consequences.
We present four cases (two females and two males) who came in neurology OPD with diagnostic dilemma and later proved to be CVT cases. Their ages ranged from 39 to 65 years with a mean age of 39. The time from disease onset to admission to hospital ranged from 45 days to 18 months (mean of 30 days). The causes included anemia (one case); however, they are not identified in rest of the three cases till thrombo-check profile pending. The current series of four patients was conducted with a written informed consent from all the participants. Characterizing clinical features, headaches was present in all four patients. Bilateral papilledema with secondary optic atrophy leading to blindness were present in two patients, seizure disorders in one patient, and language problems with limb paralysis in one patient with added features of long-standing Benign Intracranial Hypertension (BIH) in other two patients.
Case Presentation
Case 1: An adult man had presented with a 3-month history of focal motor with secondarily generalized seizures with right hemiparesis and acute, severe headache, which completely improved in the next 3–4 weeks after treatment. After two weeks of apparently asymptomatic period, headache recurred with confused state with incomprehensible speech. He was treated in a local hospital and the headache completely relieved over next 3 weeks, but the confusion and speech impairment improved partially only, for which he was presented to AIIMS Bhopal neurology department for a second opinion. There was no history of hypertension, diabetes, smoking, prior transient ischemic attacks or strokes, or any family history of young stroke. Examination revealed normal vitals and his neurologic examination revealed normal cranial nerve examination with sensory aphasia and residual weakness in wrist and elbow extensors on the right side. His cerebellar and sensory examination were unremarkable.
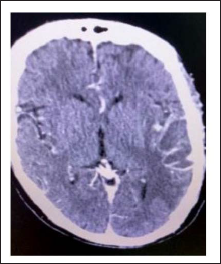
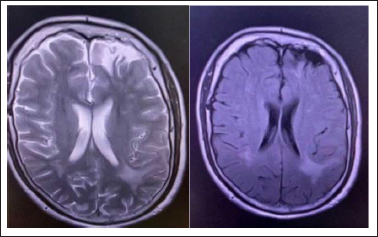
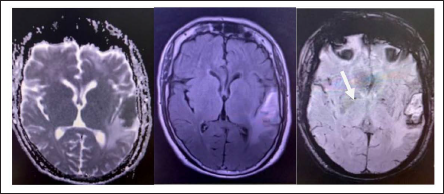
His initial Magnetic Resonance imaging (MRI) done from outside after his right-sided hemiparesis had revealed gliosis with encephalomalacia in the left frontal region. A new Computed Tomography (CT) of brain (3 months later) at the time of presentation to us revealed the hypodensity in the left temporal region with perilesional edema and contrast film showed rim enhancement. CT head angiogram and venogram were unyielding. Hence, a possibility of cerebral abscess was kept and MRI with contrast revealed diffusion restriction in the same region with blooming foci in the center. On comparing both the imaging (Figures 1, 2a,b, and 3a,b), it was noted that though diffusion restriction does occur in pyogenic abscess but blooming is not a feature of pyogenic abscess and clinically also patient did not have any features of infection or the laboratory reports supported it. His images were reviewed with senior radiologists and it was found that thrombosis was not clearly visualized but there was subtle narrowing of left sigmoid and sigmoid sinuses, as compared to the right sinuses. Furthermore, reviewing clinical status did not show signs of chronic meningeal irritation and was clinically improving without any antibiotics and hence, the possibility of chronic CVT was considered and moreover, there was no bony destruction around the lesion to suggest any fungal etiology. Moreover, subacute to chronic hemorrhage appears hypodense on CT and do show rim-like contrast enhancement. Hence, after summing up clinicoradiologic findings, finally it was concluded as a case of subacute to chronic hematoma due to CVT with partial self-recanalization of venous sinuses. We reviewed the literature for missed CVT and misdiagnosis of CVT, we found that in a large cohort, CVT was initially misdiagnosed in 1 out of 30 patients. 6 In our case, the possibility of CVT was entirely missed at the local hospital. He presented to us with subacute progressive course almost 3 months later. Headache and focal deficit at evolution and imaging findings of rim-enhancing localized lesion all drifted us away from CVT as initial possibility to more likelihood of SOL or abscess. Certain clues like blooming on imaging raised the suspicion of CVT and narrowing of sinuses on the affected side were indirect hints for subacute untreated CVT. Such patients are often misdiagnosed as SOL and may undergo unnecessary operative intervention and biopsy comes inconclusive.
Contrast-enhanced CT Image Shows Iso-to-hypodense Lesion with rim Enhancement with Surrounding Hypodensity in the Left Temporal Region.
T2-weighted Image (a) Shows Focal Hyperintense Lesion with Corresponding FLAIR-hypointensity (b) in the Left Frontal Region, Suggestive of Gliosis.
T2-weighted Image (a) Shows Focal Hypointensity in the Left Temporal Region with Perifocal Edema Visualized as Surrounding T2 Hyperintensity. Alongside, FLAIR-image (b) also Shows Variably Hyperintense Lesion with Perifocal Edema. Corresponding SWI Image (c) shows Blooming in the Same Area (arrow).
In addition, although headache was initially present, in presence of his sensory aphasia, its nature, intensity, and other characteristics could not be reliably assessed as it was difficult to communicate with him in the presence of Wernicke’s aphasia. In addition, the presence of rim-like contrast enhancement of hypodense lesion added to further confusion regarding its etiology. One should be vigilant to look for pointers indicating to CVT in subacute to chronic phase, and in this case, blooming, a marker of hemorrhage combined with narrowed CV sinuses were the clues for CVT.
Case 2: A 42-year-old gentleman presented with a new acute onset global headache associated with vomiting 1.5 years back followed by altered sensorium of 3 days. He was diagnosed with cerebral vein thrombosis involving superior sagittal sinus (SSS) and left-side transverse sinus thrombosis without parenchymal region. Patient was not compliant to the anticoagulants, sometimes took suboptimal doses of warfarin randomly neither there were INR monitoring records. Though headache was relieved to the extent that only mild headache remained, site changing, and with apparently asymptomatic period of for almost 8 months then he developed transient visual obscuration and gradual painless, progressive bilateral decrease in vision to one meter finger counting over a month. The patient had no history of color desaturation or contrast sensitivity. He could not specify particular visual field involvement. For these symptoms, patient received pulse steroids followed by oral steroids in tapering dosage from outside, a regime for optic neuritis but no improvement in vision was observed and he was presented to our hospital. No other neuroaxis domain involved such as paresis and sensory loss. There was no history suggestive of connective tissue disease. Detailed ophthalmology examination revealed normal pupils with bilateral secondary optic disc atrophy. However, rest of his examination was normal. A diagnosis of intracranial hypertension secondary to chronic complication of untreated CVT was kept and dural arterio-venous fistula (AVF) possibility was also explored. CSF for intracranial pressure monitoring was deferred in view of altered coagulogram. His serum ANA, APLA profile, and angiotensin-converting enzyme (ACE) levels were normal. Aquaporin four-antibody and anti-MOG antibody levels were normal. Serum homocysteine was mildly raised with vitamin B12 deficiency. Patient was subjected for MRI brain with orbit with spine screening with contrast, which revealed features of raised intracranial hypertension in the form of partially empty sella and mildly prominent bilateral perioptic sheath causing scleral indentation. The superior sagittal and bilateral transverse sinuses showed small filling defects suggesting partial recanalization Special sequences of MRI, ASL and TRICKS sequence, which revealed hyperperfusion at the confluence of SSS and right-side transverse sinus showing enhancement in early arterial phase, which was likely suggestive of dural arteriovenous fistula (images not available). Patient was referred for DSA for confirmation and further nidus obliteration by embolization. However, DSA report was still awaited.
This case of chronic untreated CVT presented with secondary intracranial hypertension with sequelae of secondary optic atrophy and possibly dural AV fistula but the follow-up imaging quality was not good to evaluate dural AV fistula. This patient had diagnosis of CVT but was non-compliant to the treatment of CVT as was not knowing the gravity of ongoing chronic head pain and irreversible consequences of untreated CVT so much so that he landed up with severe visual impairment. AV fistula development is quite interesting and rare complication of CVST. 7 The associations between Cerebral vein thrombosis and dural arteriovenous fistulas are well known although primary or secondary cascades of events cannot be ascertained sometimes. Tripathi and associates 8 classified DAVFs into two categories, namely cavernous sinus dural fistulas (CSDAVFs) and non-cavernous sinus dural fistulas (NCS-DAVFs). Sigmoid and transverse sinuses are involved in 30% of symptomatic intracranial DAVFs approximately. 9 Tsai et al. stated cavernous sinus (21, 30%) being the most common site for development of Dural fistulas, next site is base of skull (13, 19%), followed by transverse sinus (12, 17%), convexities of dura (8, 12%), sigmoid sinus (7, 10%), torcular herophili (5, 7%), and lastly SSS (3, 4%). One study concluded that none developed dural fistulas at 6 months after acute CVT in a study of 112 patients while they underwent follow-up cerebral MR angiography to detect development of any new dAVF formation. 10 One study showed that misdiagnosis of CVT increased the length of the stay and no other adverse outcome noted when compared with patients without a CVT misdiagnosis. 6 This case reflects that even though CVT was diagnosed at the initial period, there is a need for knowledge reception at the part of patient to know about their individual disease and ignorance ended up in irreversible consequence in the form of blindness and adding burden to the caregivers. There are two hypotheses proposed regarding causation of dural fistulas. 7 The first states that there exist arteriovenous shunts that act physiologically between networks of meningeal arteries and networks and dural venous channels. Obstruction in the outflow of sinuses leads to pressure increase within the sinuses, thus opening these channels lead to dural fistula formation between sinus and artery. The second hypothesis was proved in rat model proposed that venous hypertension induced by an obstruction to venous outflow causes venous hypertension that hampers perfusion of cerebral vessels causing ischemia creating angiogenesis. This abnormal angiogenesis leads to arteriovenous shunting in dural vessels. Intra-arterial DSA is a confirmatory technique when CT venography or MR venography is inconclusive and there exists high suspicion of a dural arteriovenous shunt. 8 CVT association with dural arteriovenous fistulae is still a complex entity and less understood. Dural fistula complicates CVT by allowing the opening of arteriovenous pathways during occlusion or recanalization and this causes persistent increased pressure over the walls. It is important to detect the fistula early (requiring intra-arterial DSA) to allow treatment with embolization. Conversely, CVT can occur during the development of an arteriovenous fistula. Whatever the relationship, clinicians need to be aware that these pathologies can co-exist and that they require specific treatments. One study was conducted in 18 patients (13 were females and 5 were males) with an average age of 39 years. CVT principally manifested as headaches, papilledema, psychiatric symptoms, varied degree of disturbed consciousness and symptomatic epilepsy, some with persistent neurodeficits. This particular study had eight misdiagnosed patients out of 18 patients with undefined etiology, less typical clinical profile, and less distinct direct neuroimaging evidence. 10
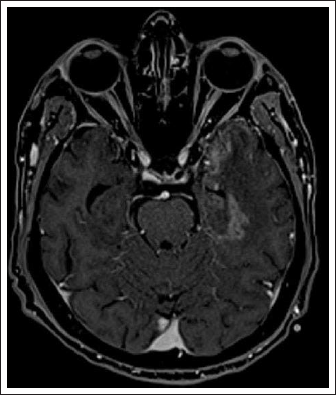
Case 3: A 50 year old woman presented with mild holo-cranial dull-aching headache of one and half month’s duration without nausea or vomiting or photophobia or phonophobia and decreases after taking analgesics, one week later left hemiparesis of sudden onset which gradually progressed to complete plegia over 7–8 h along with slurring of speech and facial deviation to right side. There were two episodes of left focal tonic-clonic movement with secondary generalization. Patient had history of COVID vaccination (Covishield) with the first dose taken 10 days prior to the illness. She did not have fever, rashes, vomiting, neither oral ulcerations, pain in joints, loose stools, or any other comorbidity. Neuroimaging was done at an outside facility and also at the study center and differentials of cerebritis/ICSOL/venous infarct were suggested. She was diagnosed with cerebral SOL and managed in periphery with anti-edema measures and antiepileptics and her weakness improved to modified ranking scale (mRS) 3. She improved moderately so did not seek further follow ups till she had recurrence of symptoms. She also gave history of menorrhagia since last 5 months. Examination revealed pallor and slight weakness in the left upper limb, but rest all the examination was within normal limits. Her routine lab investigations showed iron deficiency anemia. CT contrast (angiogram and venogram) showed venous infarct in right parietal region and attenuation of upper part of left internal jugular vein with partial filling defect (thrombus) in bilateral posterior condylar veins and also thrombo-check profile including Protein C and S was normal. USG abdomen shows adenomyotic changes with focal adenomyoma. Patient was started on anticoagulation along with iron supplementation and antiepileptics and gynecological consultation was taken for adenomyosis. Patient responded well to treatment and discharged with stable vitals. In this case, patient’s clinical profile was of subacute progressive focal deficit with seizures suggesting a cortical lesion etiology being non-infective and her images also supported SOL-like picture (Figure 4) and no direct evidence to suggest cerebral thrombosis. Only when her imaging was reviewed keenly with senior radiologist showed attenuation of cerebral vein that led to the suspicion of subacute cerebral vein thrombosis and CT venogram revealed left internal jugular vein was markedly attenuated in caliber showing linear hypodensity within the lumen in the upper part suggestive of thrombus suggesting lumen occlusion, similar intraluminal filling defect is also noticed in bilateral posterior condylar veins and condylar venous plexus with left transverse sinus appears hypoplastic. These features supported to make a diagnosis separate from her very evident SOL-like presentation for which she was already managed and got partially relieved, and her progression in symptoms led her to seek higher consultation at a tertiary hospital. Her clinical profile added with anemia resulting from menorrhagia for 6 months. When summed up the whole clinicoradiologic features, anemia associated with CVT was concluded and she was started on anticoagulation with monitoring of INR and titrated according to menorrhagia symptoms and regular gynecological consulataion was requested. Treating CVT in menorrhagia is challenging so she is under close follow up with hemogram, bleeding during cycles and with INR and dosage of anticoagulants are modified during cycles. This case of CVT occurred after 10 days of covidshield vaccination and CVT could be a result of the vaccine. Various cases of CVT following adenovirus-vector covidshield immunization have been reported,11–13 which is endangering the vaccine implementation. Several hypothetical models have tried to explain such vaccine-induced thrombosis. 14 The most acceptable one is breach of immune tolerance that trigger many autoantibodies against platelet factor-4 (PF4). Several events following intramuscular covidshield inoculation occur at molecular level including microvascular hemorrhages and platelets activation triggering release of PF4 weakening immune tolerance resulting in autoimmune cascade release of anti-PF4. Contamination of vaccine proteins, mimicry of molecular structure and of protein related to viral vector or against SARS-CoV-2 spike proteins are certain proposed causations for activation of thrombosis. 14
Legend -Contrast Axial image of berain showing left temporal heterogenous enhancing lesion suggestive of SOL.
CVST is an under-diagnosed condition. Patients present with different phenotypes that delays the correct diagnosis. Early stages of CVST may have only cortical vein thrombosis, sparing sinus. The latter is involved lately when the thrombotic process progresses. The varied presentation of CVST makes it a diagnostic challenge and so frequently missed. Seizures, motor, and sensory focal deficits with varying degree of impaired consciousness and raised intracranial features in the form of papilledema, occur almost three-fourth of cases. 15 CVST has generally good prognosis except in patients with advance age, sepsis, malignancies, deep cortical venous involvement, and poor Glasgow coma scale (GCS). Approximately 80% of patients have a good neurological outcome like in the present case and any delay in diagnosis adds to fatality.
Case 4: A 50-year-old female with no premorbidities was referred from the eye department with the history of acute onset sequential bilateral vision loss (left followed by right in a one-month-gap) over a period of 9 months. Also, she had hearing loss from left ear and headache on and off for 9 months; her previous MRI brain report showed features of BIH such as empty sella, prominent bilateral perioptic spaces with prominent CSF spaces around the Dorello’s canal, Meckel’s cave, and bilateral oculomotor nerves. Further, there is mild smooth narrowing of left transverse and sigmoid sinus on MRV and fundus showed bilateral optic atrophy. She had chronic suppurative otitis media (CSOM) in the right ear since childhood intermittently and it was operated 9 months back in a private hospital and biopsy revealed for right-sided cholesteatoma. On postoperative day 2, patient developed acute onset painless vision loss from the left eye followed by decreased hearing from the left ear 5 days later. Subsequently, in one month, the right eye also developed painless vision impairment to no light perception. Patient also had intermittent dull-aching holo-cranial non-migrainous type headache for the last 8–9 months which did not completely relieved with analgesics. Her initial eye exanimation confirmed that the patient had bilateral papilledema (outside report), and at 8 months, when she visited our department, fundus revealed bilateral secondary optic atrophy. MRI brain showed features of BIH for which she was referred to us for evaluation and to rule out secondary causes of raised ICH. The remaining neurological and general examination were normal. CSF pressure monitoring was done and it showed high CSF opening pressure (30 cm H20) with one cell and normal CSF protein and glucose levels that supported the ICH. All routine investigations along with viral markers such as HIV and VDRL were done. Pure tone audiometry (PTA) revealed bilateral mixed hearing loss at low frequencies. A fresh contrast CT was done and previous MRI films reviewed with radiology department showed partial resolving thrombosis of right sigmoid and transverse sinus and attenuation of the right proximal part of internal jugular vein. The attenuated sinuses were the subtle clue indicated a subacute thrombosis of sinuses (images not available). Anticoagulation was not indicated in this case as it was already 8–9 months of illness, but it was planned for later according to thrombo-check profile report. Neurosurgical opinion was taken for shunt surgery, and however, the attendants of patient denied the surgical procedure. Patient was discharged on acetazolamide and advised to follow-up with thrombo-check profile.
Implications
The above-described cases indicate the importance of being aware of the unrelieving headaches that seems to be benign but when not diagnosed early especially the treatable cause of venous thrombosis can lead to irreversible sequelae like blindness, persistent intra cranial hypertension, dural AVF, and so on.
By carefully looking for the chronic signatures of untreated CVT in coordination with neuroradiologist one can easily prevent misdiagnosis, thus decreasing the probability of missed CVT and wrong or delayed treatment.
Discussion
All subjects had misdaignosed due to lack of knowledge and less index of suspicion that it could be CVT because of nonspecific headache and progressive symptoms suggestive of SOL which disguised the correct diagnosis. They were presented to a tertiary hospital until they developed devastating consequences in the form of blindness. Imaging also was misreported as abscess, SOL, or cerebritis, and hence, CVT was not suspected and treatment with anticoagulants were not received. One had temporal lobe mass with rim enhancement and it was easily missed as abscess; however, keen review of the negated the infection as a cause and imaging review with a senior radiology experts gave clues like blooming, indicating remote hemorrhage in that area though with some diffusion restriction areas. Two had imaging features of increased intracranial pressure in the form of scleral flattening, tortuous optic nerves, and meningoceles that correlated the clinical features of Idiopathic intracranial hypertension (IIH) and one was misdiagnosed as an intracranial space-occupying lesion and neurosurgical, ophthalmology consultations for SOL suspicion and painless visual impairment. Delayed presentation led to devastating consequences like secondary atrophy secondary to persistent raised intracranial pressure, dural AVF and meningocele development. Lumbar puncture in two patients showed increased intracranial CSF pressures and cytobiochemical analysis was normal suggestive of BIH. The utility of lumbar puncture is to rule out infective causes and to assess the opening pressure confirming intracranial hypertension.
CVT features are always variable, as two patients do not have the same clinical profile. Headache occurs 75%–90% of CVT cases, and it is being most common and sole manifestation of around 25% of patients. 16 Headache can present diffusely or can be localized or with migrainous features at times.17–20 Headache sites has no correlation with the site of cerebral venous thrombosis, except that approximately 61% of patients with sigmoid sinus thrombus alone but pains in the occipital and neck regions indicates more of transverse or sigmoid involvement. 20 Headaches of CVT varies in intensity from dull aching to thunderclap presentation. Misdiagnosis of CVT goes high when headache is presented as sole manifestation.
With no other neurological symptoms or signs isolated intracranial hypertension occurs typically from long standing sagittal sinus thrombosis usually leads to headache, visual impairment secondary to long standing papilledema. Isolated intracranial hypertension (ICH) at first presentation indicates good outcome in three studies. One study showed 37% patients of CVT presented with isolated ICH. More than one sinus was involved in about 35 patients (59%). 21 CVT-related headache has very bizarre features, some as first presentation with thunderclap headache and others progress over hours or days; thunderclap headache is associated with subarachnoid bleeding. We suggest neuroimaging as an important tool to be performed if headache with red flags’ features as new-onset and persistent; worsening with the Valsalva maneuver; less response to regular analgesia, any pattern change from routine mundane headache. CVT often present as hemorrhagic-ischemic stroke that lacks territorial restrictions and has atypical presentations not pertaining to any subtype of headache. Varying degrees of lesion severity and different progression pace render a definite diagnosis of CVT almost impossible. However, the reason for this remains unknown in 20% of CVT cases, which increases misdiagnosis and delayed diagnosis of CVT. 22 One study showed four cases with wrong diagnosis out of eight cases and CVT was missed in them. CVT may also present with focal seizures, language disturbances, and limb weakness. Radiology helps in subacute and chronic cases of missed CVT both for diagnosis and treatment decision. Empty triangle and cord signs are some important signs that give clues for early diagnosis of CVT and has high specificity, but low positivity rate. One study showed atypical empty triangle sign in 1/18 patients. Focal edema or infarction/hemorrhage at less usual sites, not respecting territories are indirect signs in cerebral tomogram scan (CT) head. MRI brain combined with MRV still remains the gold standard investigating tool and is a preferred atraumatic and precise method for confirming CVT. 23 We can detect almost >90% of the patients with venous occlusion and subtle hints led to the correct diagnosis of CVT at delayed presentation time. If the imaging results showed atypical site of cerebral infarction or bleed, or some type of space lesions, especially in subacute and chronic phase and no direct evidence of cerebral vein or sinuses involvement, then misdiagnosis in the imaging is more likely possible. In such cases, we need to look carefully the indirect evidence, that is, in the form of blooming in SWI images of MRI scans, attenuation of the sinuses of that side, and the presence of partial thrombus with contrast, which can be otherwise missed as normal flow voids. For this radiology, consultation becomes important to conclude diagnosis. Also, biomarkers like D dimer, and fibrinogen levels are helpful in acute CVT cases and not in subacute and chronic CVT cases.
In our described patients, CVT mimicked as temporal abscess/SOL (case 1). Imaging showed the absence of flow void signals in venous channels along with and signal intensity change, suggesting thrombosis. MRV is helpful in showing various defects of flow in the form absent flow, unsharpened edges, constriction of vessels and filling incompleteness of the blood flow signals in the sinuses along with best status of the collaterals. MRI brain + MRV is a non-invasive blood vessel examination method, and it is also a gold measure for CVT diagnosis. However, MRI brain + MRV has a limitation, as it gives false positivity due to variations in anatomy and development defects of the sinuses. DSA is a useful tool to combat these limitations and is widely performed in advanced institutes. It precisely locates the thrombosed site along with dynamics of the abnormal venous back flow associated with compensatory channels formed over the disease process circulation. Since DSA require experts and it is an invasive procedure, it is done for cases with diagnostic dilemmas and high index of suspicion.
Lumbar puncture test in delayed diagnosis of CVT has a role in reflecting features of increased intracranial CSF pressure and excluding infective etiology as a cause for CVT, such as infections and malignancy. Treatment of CVT with anticoagulants when diagnosed late depends on the time of presentation, recanalization status of the sinuses, and thrombotic profile, which indicate hereditary propensity. If it is presented before 3 months, anticoagulants can be continued up to 6 months to 1 year depending on the etiology. Prolonged anticoagulants are indicated for patients having abnormal thrombophilia profile. Anticoagulant therapy like Heparin is administered either by subcutaneous or intravenous route and the activated partial thromboplastin time (aPTT) is to be doubled while the normal values overlapping with warfarin orally and INR is regularly monitored and adjusted between 2.0 and 3.0. 24 Other medical treatments include active treatment of seizure activity. In this series, one patient (case) presented 9 months with secondary optic atrophy with CSOM. Anticoagulants were deferred and optic nerve fenestration for intracranial hypertension advised after CSF pressure monitoring along with visual perimetry at follow up. Another patient who had intracranial presentation with 8 month duration, patient with secondary visual atrophy was deferred for anticoagulants treatment and visual field charting at follow up advised for correction of dural AVF once confirmed by DSA. For the rest of the two patients, anticoagulants were continued for three more months and thrombo-check profile will decide the further duration of anticoagulation.
Conclusion
Our patients had irreversible sequalae of undiagnosed, untreated CVT as optic atrophy, intracranial hypertension and suspected dural AVF so, recognition of CVT has crucial prognostic and therapeutic implications, MRI, with magnetic resonance venography, when necessary, should be performed in patients with isolated intracranial hypertension. This series give us insight regarding the natural history of untreated CVT and showed that partial self-recanalization does occur, but it does not prevent the development of irreversible complications of CVT. Also, how subtle radiologic features are to be seen with bird’s eye view to finally conclude it to be CVT. More so, isolated raised intracranial pressure from CVT should be classified neither as “IIH” nor “pseudotumor cerebri”.
Footnotes
Abbreviations
CVT, cerebral venous channel thrombosis; DSA, digital subtraction angiography; AVF, arterio-venous fistula; MRI, magnetic Resonance study; SOL, space occupying lesion; BIH, Benign Intracranial Hypertension; SSS, superior sagittal sinus; ACE, angiotensin-converting enzyme; GCS, Glasgow coma scale; CSOM, chronic suppurative otitis media.
Acknowledgement
I am thankful to the radiology department for detailing the key points of diagnosing chronic CVT.
Authors’ Contribution
Dr Priyanka V Kashyap helped in writing the main manuscript and data collection; Dr Manshi Kashyap in formatting the manuscript and literature search; Dr Akanxa Yadav in editing, image compilation, and supervision; and Dr Arpit Dhiran in corrections, literature search, and planning.
Statement of Ethics
Written informed consent was obtained from the patient.
Declaration of Conflict of Interest
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.