
Abstract
Background:
Cerebral venous sinus thrombosis (CVST) is an uncommon subtype of stroke, and the role of D-dimer and fibrinogen in early diagnosis of CVST has been studied with varying results. The present study aims to study the role of the combination of D-dimer and fibrinogen in early diagnosis of acute CVST.
Methods:
Forty consecutive confirmed acute CVST cases admitted at a tertiary care center were recruited for the study. D-dimer and fibrinogen were assessed by a rapid semiquantitative latex agglutination assay.
Results:
Out of the 40 CVST patients, 21 (52.50%) were females. The mean age of the patients was 37.58 years ± 19.17 years. Common clinical features were headache (N = 38 [95%]), papilloedema (N = 15 [37.5%]), and seizures (N = 12 [30%]). Although the sensitivity (75%) of the combination of D-dimer and fibrinogen assay was lower than that of D-dimer or fibrinogen alone, the specificity and positive predictive value (75% each) was higher.
Conclusion:
The combination of D-dimer and fibrinogen testing may aid in an early diagnosis of acute CVST and in better management.
Introduction
Cerebral venous sinus thrombosis (CVST) is a relatively uncommon subtype of stroke with an incidence rate of 1.32 to 1.57 per 100,000 person-years.1, 2 Symptoms vary from headache and seizure to focal neurological deficit. Although the disease can be managed, it can cause significant morbidity and mortality if diagnosed late. Magnetic resonance imaging (MRI) in combination with magnetic resonance venography (MRV) or computed tomography venography is the investigation of choice in the diagnosis of the disease depending upon the circumstances. 3 Although the diagnosis appears to be straightforward, studies have shown that CVST is misdiagnosed in as high as 73% of the cases and that there can be a delay in diagnosing the disease for over 10 days. 4 Getting an MRI done in emergency rooms is difficult, especially in resource-poor countries like India. Early diagnosis is imperative to prevent mortality, which ranges from 4.3% in acute disease to 3.4% in patients admitted within a month of symptom onset. 5 Therefore, the role of a plasma biomarker in the early diagnosis of the disease becomes invaluable, and it would lead to early and better management of the disease. The sensitivity of the raised D-dimer varies from 93.9% to 97.8%, and specificity from 84.9% to 89.7% in diagnosing CVST in different studies.6, 7 In a study by Pathak et al., the sensitivity and specificity of D-dimer assay in the diagnosis of CVST was 81.25% and 62.5%, respectively. 8 In one of the only studies published by Meng et al., the sensitivity and specificity of D-dimer in combination with fibrinogen were 67.6% and 98.9%, respectively, in the Chinese population. 9 The present study was designed to evaluate the diagnostic sensitivity and specificity of the D-dimer and fibrinogen in diagnosing acute CVST.
Methods
The study was approved from the Institute Ethics Committee. The study was done in Sir Sunderlal Hospital, Banaras Hindu University—a tertiary care center in northern India. This was a prospective case control study carried out from September 2017 to February 2020 in the Department of Neurology. Consecutive, confirmed acute CVST cases (onset within three days) 10 based on clinical features and imaging findings, with age more than 15 years, admitted in neurology wards were included.
Exclusion Criteria
Patients with hepatic and renal impairment, disseminated intravascular coagulopathy, deep vein thrombosis (DVT) or pulmonary embolism, history of malignancy or a known case of malignancy at the time of diagnosis, and presence of other systemic disease or condition affecting D-dimer and fibrinogen levels (pregnancy, puerperium, septicemia, or meningitis) or on anticoagulation for other etiology were excluded.
A total of 40 CVST cases were recruited, and a similar number of age-matched acute migraine patients visiting the emergency room were also recruited as healthy control. CVST was excluded in the control group based on the typical clinical feature and the normal neurological and radiological feature. Detailed history and examinations of CVST patients were done by a neurologist and the findings were noted on a prespecified format. All the relevant investigations including complete hemogram, erythrocyte sedimentation rate, serum biochemistry, radiograph of chest, and electrocardiogram were done. Thrombophilic workups including protein C, protein S, antithrombin III, factor V Leiden and methylenetetrahydrofolate reductase (MTHFR) gene mutation, antiphospholipid antibody, lupus anticoagulant, antinuclear antibody, and anti-ds deoxyribonucleic acid (DNA) antibody were done. MRI brain with contrast venography (Sigma HDxT, GEMS, Milwaukee, USA) was done in all patients. Radiological parameters including site and type of parenchymal lesions were recorded. On venography type, location and extent of venous sinus involvement were noted. The D-dimer and fibrinogen levels were assessed by a rapid semi-quantitative latex agglutination assay (STAGO’s D-Dimer Test). The cut-off values were equal or greater than 0.5 µg/mL for D-dimer and equal or greater than 4 g/L for fibrinogen, in accordance with the normal criteria of our laboratory and the criteria of other previous published studies. A blood sample for testing was collected within 48 h of the diagnosis. 1.8 mL of venous blood was collected in a vial containing 0.2 mL of 3.8% solution of trisodium citrate. Patients diagnosed with CVST were treated with low molecular weight heparin 100 unit/kg subcutaneously twice daily for five days followed by warfarin (orally), keeping the international normalized ratio (INR) between 2 and 2.5 during the course of the study.
Statistical Analysis
Descriptive statistics were calculated for all data of samples assays. All the values in the text and tables were presented as mean ± standard deviation and are analyzed with independent sample t-test. The percentages of the cases with abnormally elevated D-dimer and/or fibrinogen in each group were analyzed with chi-square test. A variable with P-value less than .05 was considered to be statistically significant. The specificity and sensitivity of D-dimer and fibrinogen on CVST prediction were described using receiver operating characteristic curve. All calculations were performed with the SPSS 25 statistical package (SSPS Inc. Chicago, IL 60606-6412, USA).
Results
A total of 40 cases (CVST patients) and 40 controls (migraine patients) were included. Mean age of patients was 37.58 years ± 19.17 years. 21 (52.50%) were females. Headache was the most common symptom and was present in 38 (95%) patients, followed by nausea in 26 (65%), nausea and vomiting in 21 (52.50%), blurred vision in 15 (37.50%), and seizures in 12 (30%) patients. Generalized tonic clonic seizure was present in 9 out of 12 (75%) cases.
Demographic, Clinical, Laboratory, and Radiological Characteristics of Acute CVST Patients
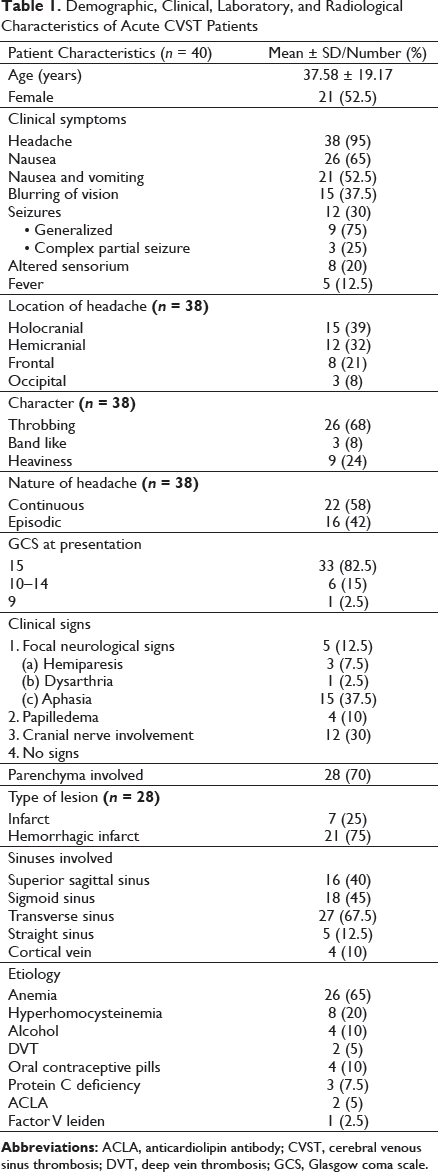
Baseline levels of D-dimer and fibrinogen in the CVST group were compared with the control groups. The average plasma D-dimer level in the CVST group (1.818 ± 0.941µg/mL) was significantly higher than in the control group (0.949 ± 0.941 µg/mL; P-value= < .001). The average plasma fibrinogen level in the CVST group (4.712 ± 1.594 g/L) was also significantly higher than in the control (3.861 ± 1.533 g/L) (P-value = .017).
Among the CVST patients, 80% (32/40) had D-dimer elevation, 65% (26/40) had fibrinogen elevation, and 65% (26/40) had both D-dimer and fibrinogen elevation. In addition, 15% (6/40) had D-dimer elevation but normal fibrinogen; however, none had normal D-dimer with elevated fibrinogen levels. Eight (20%) CVST patients had normal D-dimer and fibrinogen levels. In the control cases, only 32.5% (13/40) had D-dimer elevation, 37.5% (15/40) had fibrinogen elevation, 32.5% (13/40) had both D-dimer and fibrinogen elevation, and 62.5% (25/40) had normal levels of D-dimer and fibrinogen.
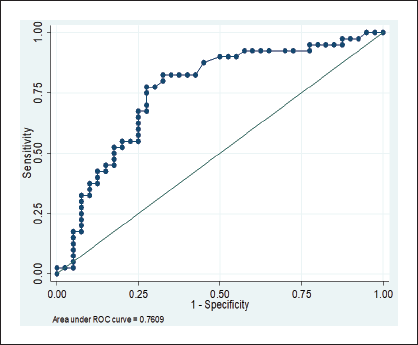
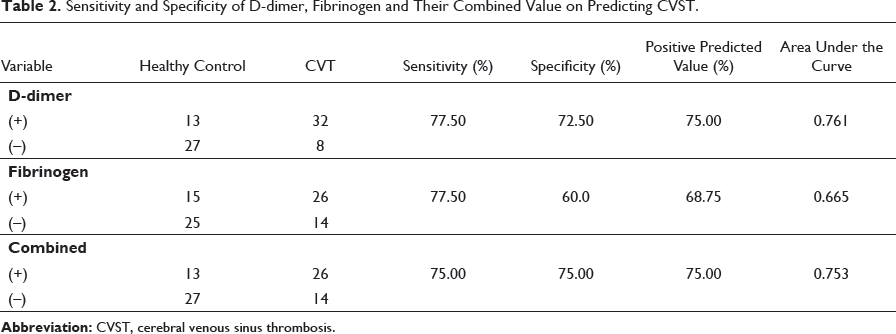
The sensitivity and specificity of D-dimer and fibrinogen levels alone and their combination in acute phase are displayed in Table 2. The cut off value for D-dimer assay was equal to or greater than 0.5 µg/mL and the area under the curve of D-dimer in acute phase was found to be 0.761 (Figure 1). The sensitivity was found to be 77.5%, specificity 72.5%, and positive predictive value 75%. The cut off value for fibrinogen was equal to or greater than 4 g/L and the area under the curve of fibrinogen in acute phase was found to be 0.665 (Figure 2). The sensitivity was found to be 77.5%, specificity 60%, and positive predictive value 68.75%. When both D-dimer and fibrinogen were combined, the sensitivity, specificity, and positive predictive value was 75% each. The area under the curve for the combined D-dimer and fibrinogen in acute phase was 0.753 (Figure 3).
ROC for Predicting Acute CVST by D-dimer.
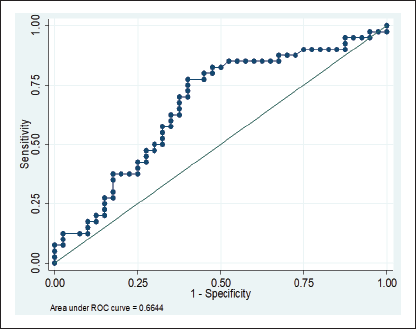
ROC for Predicting Acute CVST by Fibrinogen.
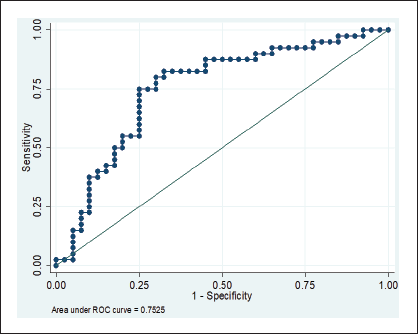
ROC for Predicting Acute CVST by Combination of D-dimer and Fibrinogen.
Sensitivity and Specificity of D-dimer, Fibrinogen and Their Combined Value on Predicting CVST.
Discussion
The highlight of present study was that of the 40 CVST patients, 80% had D-dimer elevation, 65% had fibrinogen elevation, and 65% had both D-dimer and fibrinogen elevation. Our study, re-evaluating the role of D-dimer and fibrinogen in diagnosing the acute CVST along with the sensitivity and specificity when both the molecules were combined together, revealed a relatively lower sensitivity (75%) but higher specificity (75%) and positive predictive value (75%) in comparison to D-dimer and fibrinogen when used alone. The sensitivity and specificity of the diagnostic value of D-dimer was similar to the author’s previous published work and was also consistent with the study published by Venkatesh et al., in South Indian Cohort of CVST patients.8, 11 In a similar study by Meng et al., the sensitivity and specificity of D-dimer was 94.1% and 97.5%, respectively, which was relatively very high, and the difference could be because of the different population and difference in the time of diagnosis and inclusion in the study. 9 In a similar study done by Kionski et al., in CVST patients, sensitivity and specificity of D-dimers was 97.1% and 91.2%, respectively. 12 Metanalysis done by Alons et al. and Dentali et al. concluded that sensitivity of the raised D-dimer varies from 93.9% to 97.8% and the specificity from 84.9% to 89.7% in diagnosing CVST.6, 7 Although D-dimers have a high negative predictive value in CVST patients with isolated headache, a negative D-dimer test cannot rule out CVT, as false negative results can be seen in isolated headache, longer duration of symptoms, and limited sinus involvement.6, 7 In our study, the diagnostic sensitivity and the specificity of fibrinogen alone were 60% and 68.75%, respectively. The only similar study published by Meng et al., had sensitivity of 73.5% and 83.9%, respectively. 9 The diagnostic sensitivity and specificity of D-dimer and fibrinogen in combination was 75% each. Meng et al., also found that the sensitivity and specificity of combination of D-dimer and fibrinogen in the acute stage were 67.6% and 98.9%, respectively. 9 The reasons for the different sensitivity in the present study could be because of the variability in time of the diagnosis of patients of the two-study population and/or because of the genetic difference along with the different etiology of the CVST of the two study groups. Despite the low sensitivity in comparison to either test alone, the positive predictive value was 75%, which adds to the importance of combined tests of the two molecules. However, it needs to be emphasized that these biomarkers act as a complementary tool to the intracranial imaging in clinching the diagnosis of this rare entity as these can also be elevated in other clinical conditions. 13 In a recent study by Heldner et al., a score combining clinical symptoms and D-dimer levels to predict diagnosis of CVST was used and, with the suggested cut off, the reported performance was sensitivity 83%, specificity 86.8%, negative predictive value 93.5%, and accuracy 84.4%. 14 Many features of this study differed from the previous studies. First, this was the largest published cohort studying the combined values of D-dimer and fibrinogen in acute CVST (40 cases) along with the clinical and radiological features, which was an extension of our previous study. 8 Second, the study highlights the decent positive (75%) predictive value of the combined D-dimer and fibrinogen test, hence emphasizing the importance of the combining the two molecules for diagnosing acute CVST patients.
A major limitation of the study was the small sample size, which might have led to variations from the published literature in the value of measured statistical variables. Hence, in future, prospective studies in a larger population are needed to confirm our findings.
Conclusion
Our study suggests that combination of D-dimer and fibrinogen testing may help in guiding the diagnosis of acute CVST and in better management. D-dimer in combination with fibrinogen may increase the positive predictive value of acute CVST. However, patients suspected with normal plasma D-dimer or fibrinogen should not be excluded from the diagnosis of CVST. A large multicenter trial with higher statistical power is needed to confirm our findings.
Footnotes
Acknowledgments
We acknowledge all our patients for giving their consent and participating in the study. The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available because of privacy or ethical restrictions.
Authors’ Contribution
AP: Concept and design of study, writing the manuscript. VKS: Reviewing and analyzing the data, Manuscript editing. AK: Analyzing data and editing the manuscript. VNM: Reviewing and analyzing the data. RNC: Data collection, writing and reviewing the manuscript. DJ: Data collection and supervision, reviewing the manuscript.
Statement of Ethics
Ethical approval was taken from institute ethical committee. The present research complies with the guidelines for human studies and should include evidence that the research was conducted in accordance with the World Medical Association Declaration of Helsinki.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Abhishek Pathak and Varun Kumar Singh will have the first authorship because of equal contribution. Rest, there is no conflicts of interest between the authors to declare with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.