
Abstract
Background
Several studies have been conducted on the inflammatory aspects of migraine. Pentraxins are a novel and important part of innate immunity as a superfamily of acute phase proteins. In our study, we aimed to demonstrate the relationship between migraine and the serum levels of pentraxin-3 (PTX-3), C-reactive protein (CRP), fibrinogen and D-dimer.
Methods
We recruited 30 migraine patients (in both the attack and interictal period) and 30 healthy controls. Serum samples were obtained from all participants, and a brain MRI performed in the last six months was assessed regarding the presence of deep white matter lesions. Comparisons between the attack, interictal and control groups regarding the serum levels of PTX-3, CRP, fibrinogen and D-dimer were performed. The association between serum PTX-3 levels and migraine characteristics (disease duration, headache frequency, MRI findings, aura, family history, attack duration, and MIDAS score) was also assessed.
Results
We found higher serum levels of fibrinogen and PTX-3 in migraine attack patients compared with the interictal and control groups (p = 0.03 and p < 0.001, respectively). Subgroup analysis also showed that patients with a disease duration of more than five years and with an attack duration of more than 12 hours have lower serum levels of PTX-3 than patients who have a relatively new diagnosis and have relatively short-lasting migraine attacks (p = 0.042 and p = 0.038, respectively).
Conclusions
PTX-3 and fibrinogen exhibit different serum levels in patients undergoing a migraine attack compared with the interictal group and the controls. Participants with longer attacks and disease durations have lower serum levels of PTX-3, suggesting that inflammatory processes change along with disease progression.
Introduction
Several studies have linked migraine to other comorbidities in recent years (1). Patients with migraine, especially migraine with aura, have been reported to have an increased risk of ischemic stroke (2–5). Migraine is also associated with an increased incidence of silent lesions such as deep and periventricular white matter lesions (WMLs) (6). The increased risk of ischemic stroke in migraine patients is further supported by studies that demonstrate that prothrombotic conditions are more common in patients with migraine compared to patients without (7,8). Various cytokines also seem to play an important role in the pathophysiology of migraine, whereas pro-inflammatory cytokines have been shown to be associated with pain (9,10). As shown in animal studies, neurogenic inflammation around the dural trigeminal afferents plays an important role in the generation of migraine attacks, whereas plasma protein extravasation and vasodilation play potent roles in neurogenic inflammation as well as in the generation of migraine headache pain. It has been suggested that the activation of trigeminal sensory fibers leads to neurogenic inflammation within the meningeal vasculature mediated by neuropeptide release from trigeminal sensory fibers and is characterized by plasma protein extravasation, vasodilation, and mast cell degranulation in the pathogenesis of migraine. However, studies on post-capillary blockade of extravasation showed that receptor-mediated inhibition of extravasation failed to treat acute migraine (11).
Several studies have been conducted on the inflammatory aspects of migraine, and thus, associations between various inflammatory biomarkers and migraine have been noted in several papers. The level of C-reactive protein (CRP), which has been associated with coronary heart disease and stroke in previous studies (12), was found to be abnormal among migraine patients (13). D-dimer and fibrinogen play potent roles in the systemic inflammatory response and prothrombotic conditions (14,15), and these biomarkers were also linked with the pathophysiology of migraine (7,16).
PTX-3 is one of the pentraxins with a C-terminal and long N-terminal domain. It differs from classical short pentraxins (i.e. CRP) in that is has an unrelated long N-terminal domain. Various cell types, such as macrophages, endothelial cells and vascular smooth cells, produce PTX-3. PTX-3 release appears to be specific to vascular damage (17). The association between PTX-3 and various neurological disorders have been investigated. In stroke patients, higher levels of PTX-3 have been associated with increased mortality (17). In a different study, the PTX-3 levels were higher in Parkinson’s disease compared to the control group (18). In our study, we aim to demonstrate the relationship between migraine and the serum levels of PTX-3 and other inflammatory biomarkers (CRP, fibrinogen and D-dimer). We also investigate serum PTX-3 levels and their association with migraine characteristics.
Methods
This study was approved by our institutional ethics committee, and written informed consent was obtained from all participants.
Participants
Between July 2014 and November 2014, migraine patients who presented to the outpatient clinic with a migraine attack were considered for enrollment in our study. In this patient population, 30 consecutive migraine patients were selected according to the inclusion and exclusion criteria (Figure 1).
Flowchart of patients who met inclusion/exclusion criteria.
The inclusion criteria for the patient group were as follows: volunteering for the study; age between 18 and 45 years; established migraine diagnosis according to the International Classification of Headache Disorders, second edition (ICHD-2); episodic migraine with an attack frequency of less than five attacks per month; brain magnetic resonance imaging (MRI) performed within the last six months; lack of any acute or chronic disease other than migraine confirmed by medical reports and initial examination; non-obese (body mass index (BMI) < 30); no medications including anti-aggregants, anticoagulants, oral corticosteroids, selective serotonin re-uptake inhibitors (SSRIs) and antipsychotics prior to the study; no medications such as ergotamine, triptans and nonsteroidal anti-inflammatory drugs (NSAIDs) one week prior to the initial blood sampling; and no drug or substance addiction/abuse.
The exclusion criteria for both groups were as follows: any imaging finding other than focal T2 hyperintesity detected on brain MRI (n = 1, lacunar infarct); any type of ongoing or recurrent headaches during the week after a migraine attack (n = 12, nine patients had recurrent headache, and three patients had a headache on the day of the blood sampling); attacks that did not respond to a single dose of antimigraine medication (n = 22); the presence of any other inflammatory condition within the week after the migraine attack (n = 1, menstruation); and lost to follow-up (n = 6).
All migraine patients underwent medical treatment for the migraine attack at the time of admission and were asked to revisit the clinic one week later. After seven days, blood samples were obtained from the same patients to constitute the “interictal” group. The control group consisted of 30 age- and gender-matched individuals with no known medical conditions. The attack treatment consisted of 50 mg of intravenous dexketoprofen trometamol (DT). The choice of DT for attack treatment at our institution and in this study setting was based on its pharmacokinetics: (i) rapid onset of action; (ii) virtually no accumulation in biological tissues; and (iii) rapid and virtually complete elimination (19,20).
Imaging procedure
All MR examinations were performed with a 1.5 T MRI scanner (Magnetom Avanto, Siemens Healthcare, Forcheim, Germany). T1-weighted, T2-weighted, and fluid-attenuation inversion recovery (FLAIR) images were acquired. On MRI, periventricular and white matter lesions (WMLs) were defined as bright foci on T2-weighted and FLAIR images. All readings were performed by a single radiologist who was blinded to the patient data. Evaluations were made on a patient basis and counts of lesions were recorded for all participants. Headache-related or non-related imaging findings other than WMLs were noted. Patients were divided into two groups: The first group consisted of patients with no detected WMLs, and the second group included migraineurs with at least one hyperintense focus on MRI.
Immunoassay analysis
Fasting venous blood samples from the interictal and control groups were collected to measure the serum PTX-3 levels. Blood sampling from patients with a migraine attack were performed within the first four hours of the attack period. Thirty minutes after drawing the blood samples, the tubes were centrifuged for 10 minutes at 3000 rpm. Samples were aliquoted and stored at –80℃. Serum PTX-3 levels were measured using a commercial sandwich enzyme-linked immunosorbent assay (ELISA) (Aviscera Bioscience, Santa Clara, CA, USA. Catalog no: SK00101-06). The PTX-3 concentrations in the samples were determined by comparing the optical density of each individual sample with the standard curve. The intra-assay coefficient of variation for the assay was 4%–6%.
Statistical analysis
Summary statistics of both groups were obtained based on the means or medians and 95% confidence interval (CI) for the means or medians. Data are presented as line graphics. The distribution of normality was assessed with the D’Agostino-Pearson test. Nominal categorical variables were assessed with the Fisher exact test. Repeated-measures analysis of variance (ANOVA) test and the Friedman test were used to compare the normal and non-normal distributed data within more than two groups. Pairwise comparisons were performed via the Scheffé test, and Bonferroni correction was applied after repeated-measures ANOVA. Continuous variables with a normal distribution within the subgroups were compared with the independent t test. A two-tailed p value < 0.05 was considered to be statistically significant. All statistical analyses were performed using MedCalc statistics software (MedCalc, version 12.2.1.0, Mariakerke, Belgium).
Results
Distribution of patients within subgroups.

MIDAS: Migraine Disability Assessment Score.
Data regarding serum CRP, fibrinogen, D-dimer and PTX-3 levels in all groups are presented in Figure 2. Statistically significant differences in the median concentration of fibrinogen levels were present between the attack and interictal groups, and between the attack and control groups (p = 0.03). Serum levels of PTX-3 were also found to be statistically significant between the attack and interictal groups and between the attack and control groups (p < 0.001).
Serum CRP, fibrinogen, D-dimer and PTX-3 levels of all groups by means (median for PTX-3) and 95% CI for means (median for PTX-3) are presented as line graphics. Means and median are shown as central triangles. Upper and lower levels of CIs are shown as terminal horizontal lines. For fibrinogen levels, multiple comparisons revealed significance between attack vs. interictal and attack vs. control with significance level of 0.05. For PTX-3 levels, pairwise comparisons revealed significance between attack vs. interictal and attack vs. control with Bonferroni correction. There was no significance between the three groups regarding serum levels of D-dimer and CRP.
Subgroup analysis of serum Pentraxin-3 levels in patients obtained at the time of migraine attack.
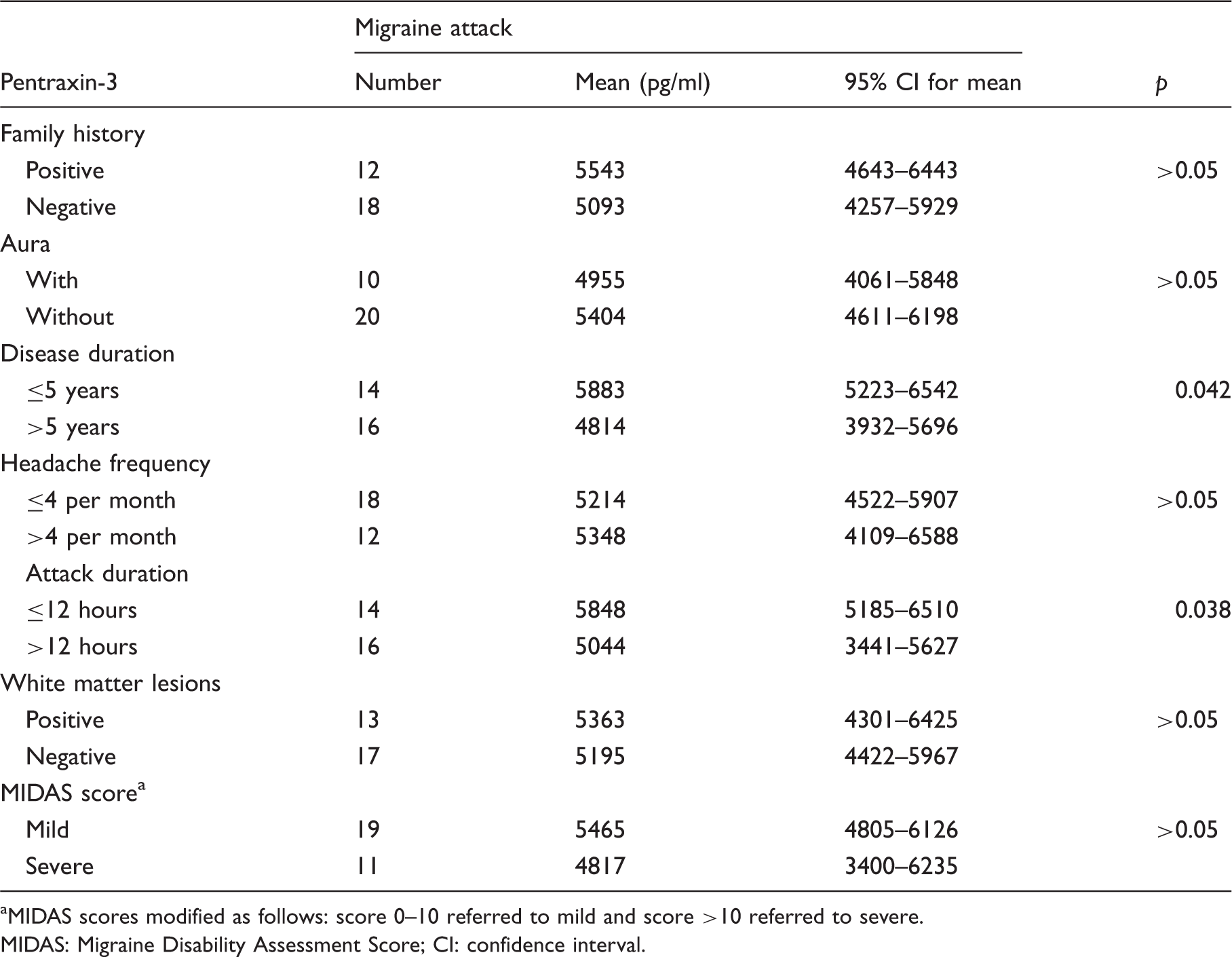
MIDAS scores modified as follows: score 0–10 referred to mild and score >10 referred to severe.
MIDAS: Migraine Disability Assessment Score; CI: confidence interval.
Discussion
We found higher serum levels of fibrinogen and PTX-3 in migraine attack patients compared with interictal and control groups. Subgroup analysis also showed that patients with a disease duration of more than five years and with an attack duration of more than 12 hours exhibit lower serum levels of PTX-3 compared to patients who have relatively new diagnoses and relatively short-lasting migraine attacks. Furthermore, the disease duration is associated with attack duration as patients with disease more than five years tend to have migraine attacks that last more than 12 hours. Assuming that chronicity of the disease based on the disease duration and attack duration is associated with a decreased inflammatory response, inflammation might play an initial role in the pathophysiology of the migraine.
Inflammation and migraine association is noted in many other scientific papers, and serum levels of fibrinogen, CRP and D-dimer have been linked to migraine in these studies (7,13,16,21–27).
Fibrinogen is a glycoprotein that acts in the final cascade of blood coagulation and regulation of leukocyte function in inflammation. Fibrinogen is a key factor in the coagulation cascade and exhibits proinflammatory properties as an acute phase reactant (21). Studies conducted on migraine patients investigating the association of fibrinogen reveal discrepant results. In one study, lower plasma levels of fibrinogen were reported in migraine patients (22), whereas two others have reported an increase in fibrinogen in migraine patients compared to controls (7,16). Furthermore, a general population-based study revealed that the elevated fibrinogen levels were most closely associated with migraine attack in women with a high frequency of attacks (23). Our study results are consistent with the results in that study. We found higher levels of fibrinogen in attack patients, although there were no significant differences between the interictal and control groups.
D-dimers are formed by plasmin-mediated degradation of fibrin. In addition, increased levels of fibrin degradation products, such as D-dimer, are commonly used in clinical practice as markers of inflammation, increased coagulation activity, and risk predictors for thrombotic conditions (24,25). Yucel et al. found significantly higher levels of D-dimer in migraine patients compared with healthy controls. In their study, they also found that plasma D-dimer levels differed between the migraine attack group and the interictal group (7). In contrast, we found no significant differences in serum D-dimer levels between the attack and interictal groups or between the interictal and control groups.
CRP has been reported to be abnormal among migraineurs in many studies. However, these studies yield inconsistent results. In some studies CRP is found to be elevated in migraine patients without aura (13,26). Furthermore, some other studies found no difference between patients and control groups. However, these results were obtained from patients in the non-attack state and comparisons were made with healthy controls (27). In our study, we assessed serum levels of CRP in patients within the attack and interictal period, and our results yielded no significant differences.
As a novel and important part of innate immunity, pentraxins are a superfamily of acute phase proteins and basically serve as one of the pattern recognition receptors (28). The association between PTX-3 levels and several other diseases has been presented in the literature (29), whereas there are no data available on the connection between PTX-3 and migraine.
Considering the fact that the levels of several inflammatory biomarkers increase at the beginning of a migraine attack as we also found in our study, inflammatory mechanisms may play a dominant role at the beginning of the migraine attack but may lose their initial effect as the attack state progresses. Neurological mechanisms may be involved in the neuroinflammation process after this point. The neuroinflammatory basis of the migraine attack has been suggested in many research papers. In animal models, it is suggested that inflammatory substances may contribute to the activation and sensitization of the ophthalmic division of the trigeminal nerve (TGV). The continuous and abnormal stimulation of the TGV system could promote central sensitization: The sustained firing of sensitized meningeal nociceptors leads to the sensitization and activation of second-order central TGV neurons (30,31). In animal studies, the activation of TGV afferents by inflammatory substances initiates the migraine pain and central sensitization. Self-sustained central desensitization is thought to play a potent role in maintaining and prolonging migraine pain (30). This might be a clue for migraine treatment; anti-inflammatory agents might be more effective for relatively short-lasting attacks (<12 hours), whereas neuronal modulators might be preferred for long-lasting attacks (>12 hours). Similarly, patients with disease for more than five years might gain less benefit from anti-inflammatory medication.
White matter hyperintensities are believed to be associated with atherosclerosis, increased risk of ischemic stroke, and cognitive disorders (32). The association between migraine and MRI-measured white matter hyperintensities emphasizes the point that recurring migraine headaches may be associated with migraine-associated cerebral ischemia. In a general, population-based study, authors found that migraine patients had a higher prevalence of deep white matter hyperintensities on MRI, especially in the posterior circulation territories (11). In our study, we found no difference in the PTX-3 levels in migraine patients with and without deep WMLs. We also found no relationship between WMLs and other disease characteristics. However, we should mention that larger series are needed to evaluate this association.
Our study also has some limitations. Our study group is relatively small, and it should be supported by studies with larger groups of individuals. We classified the participants into three main groups: migraine attack, interictal and controls. Furthermore, we divided the migraine attack group into subgroups. However, the grade or classification of patients in the subgroups was modified in some respects. In the MIDAS subgroup, for instance, we defined two grades (mild, severe) rather than four actual grades (minimal, mild, moderate, severe) to increase the power of the statistical analysis. Such modification is also valid for disease duration and headache frequency. Again, we should mention that larger groups of patients are needed for additional subgroup analyses.
Conclusions
Fibrinogen and PTX-3, as markers of vascular inflammation, have different serum levels in patients with migraine attack vs. interictal and controls. Serum PTX-3 levels also show changes in different disease characteristics. Individuals with different lengths of attacks and disease durations have different serum levels of PTX-3, which suggests that inflammatory processes are altered along with disease progression.
Footnotes
Article highlights
Serum fibrinogen and pentraxin-3 (PTX-3) levels rise during a migraine attack.
Patients with disease duration of more than five years have lower serum levels of PTX-3 than patients who have relatively new diagnosis.
Patients with attack duration of more than 12 hours have lower serum levels of PTX-3 than patients who have relatively short-lasting migraine attacks.
Inflammation might play an initial role in the pathophysiology of migraine.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.