
Abstract
The present study analyzed the (ICHD I-1988) and (ICHD II-2004) diagnostic criteria in children and adolescents. Our population consisted of 496 patients of the Headache Outpatient Ward for Children and Adolescents retrospectively studied from 1992 to 2002. Individuals were classified according to three diagnostic groups: Intuitive Clinical Diagnosis (Gold Standard), ICHD I-1988 and ICHD II-2004. They were statistically compared using the variables: Sensitivity (S), Specificity (Sp), Positive Predictive Value (PPV), Negative Predictive Value (NPV). When ICHD I-1988 was used, the sensitivity of migraine without and with aura was 21% and 27%, respectively, whereas in ICHD II-2004 it changed to 53% and 71% without affecting specificity. As a conclusion, the current classification criteria (ICHD II-2004) showed greater sensitivity and high specificity for migraine than ICHD I-1988, although it improved migraine diagnosis in children and adolescents, the sensitivity remains poor.
Introduction
In children and adolescents, headache is a highly prevalent symptom. Bille (1), in 1962, in his classical study, observed at least one episode of headache in 40% of 7-year-old children and 75% of 15-year-old adolescents. Several other populational studies have been carried out and showed a prevalence of migraine ranging from 2.7% to 22%(2–10).
In Brazil, to the best of our knowledge, there are no national prevalence studies available. In Porto Alegre (RS), Barea et al. (11), in 1996, evaluated 538 students with ages ranging from 10 to 18 years, using the criteria of the International Headache Society (IHS), International Classification of Headache Disorders (ICHD I-1988) (12, 13), and found prevalence rates of headache of 82.9%. The diagnosis of tension-type headache was given to 72.8% and of migraine to 9.9% of the students with headache. Primary headaches prevailed, that is, those where headache was the major symptom in the disease or syndrome.
In children/adolescents, tension-type headache and migraine are prototypes of primary headaches (11, 14–16). In populational studies tension-type headache prevails (7, 9, 11, 17) and migraine prevails in tertiary service studies (18–21). Migraine manifestations may take place from the first six months of life (18, 22–24).
The diagnosis of headaches is mostly clinical, by accurate anamnesis, and it is very difficult in children, especially young children (25–27).
Different diagnostic criteria have been used throughout the history of classifications (1, 2, 7, 27–38). The ICHD I-1988, based on operational criteria, allowed several studies and researches to be carried out, and several authors proved that these criteria have high specificity, but low sensitivity (17, 19, 32–39).
Among the different suggestions and proposals to change ICHD I-1988 criteria for migraine without aura in children, the most cited was the decrease of the minimum duration of crises to one hour, which would increase sensitivity without interfering with the specificity (17, 19, 32–41).
In 1999, with the IHS Committee, meetings were held to create the new edition of the classification and diagnostic criteria for headaches. No studies using the ICHD II-2004 classification have been found in literature. Therefore, scientific studies using these new criteria are required to evaluate its specificity and sensitivity. The objective of this study therefore was to critically evaluate the ICHD I-1988 and ICHD II-2004 diagnostic criteria of migraine for children and adolescents.
Materials and method
Five hundred and eight charts of patients seen and followed-up at the Headache Outpatient Ward for Children and Adolescents, GHMS-UNESP-Botucatu, were retrospectively evaluated from 1992 to 2002, after a minimum clinical follow-up of one year.
When the charts were reviewed, 12 patients were excluded due to inadequate filling of the standardized protocol for the new cases and for the follow-up visits, a headache diary was also routinely used to follow-up these cases. The final casuist was 496 individuals aged up to 15 years. Periodical childhood syndrome cases were not included (item 1.5 –ICHD I-1988 and 1.3-ICHD II-2004).
Individuals were classified according to gender, age, type and duration of pain and type of headache in three diagnostic groups, according to:
Standard diagnosis criteria (SD)/Gold Standard: obtained through the ‘intuitive clinical diagnosis’, considering the physicians previous knowledge based on all the former classification of headache and studies about this subject, analysis of standardized protocols and headache diaries with parents’ and caretakers’ information on the headache events and the patients’ and family′ s previous history. The clinical features of pain were also considered, they are: location (uni or bilateral), quality, and intensity. The headache attacks duration included periods shorter than one hour to 72 h as well as the sleeping period in patients who fell asleep during an attack. The classical accompanying symptoms, like nausea and/or vomiting, photophobia, or phonophobia or osmophobia were taken into account when diagnosing the headache (1, 2, 27–38, 40, 41);
ICHD I-1988 diagnosis criteria (13);
ICHD II-2004 diagnosis criteria (42).
The ICHD I and II were fully respected concerning all operational criteria, notes and comments involving children and adolescents including in the lasting of pain the period when they fell asleep with headache and woke up without it.
The three groups (SD, ICHD I-1988, ICHD II-2004) were statistically compared, using Sensitivity (S), Specificity (Sp), Positive Predictive Values (PPV) and Negative Predictive Values (NPV), as defined by CLAP (43) and according to Rouquayrol (44).
Ethical procedure
This study may be considered without risk since it used retrospective technique (charts review) and method and it did not use any intentional intervention or modification in physiological, psychological and social variables of the individual. It was approved by the medical ethics committee, GHMS – Botucatu – UNESP.
Results
In this study, 261 (52.62%) were male and 235 (47.38%) were female, aged 2–15 years, mean age ± standard deviation 9.32 ± 6.63 (Fig. 1). Patients were divided according to duration of pain: 27% regardless of time (less than 30 min), 19% from 30 min to 1 h, 32% 1–2 h and 20% 2–72 h as shown in Fig. 2.

Distribution according to age.

Distribution according to duration of pain. ▪ < 30 min; ░ 30 min−1 h; 1–2 h; □ 2–72 h
The following findings were observed: 93.4% primary headaches, 4.6% secondary headaches and 2% nonclassifiable headaches.
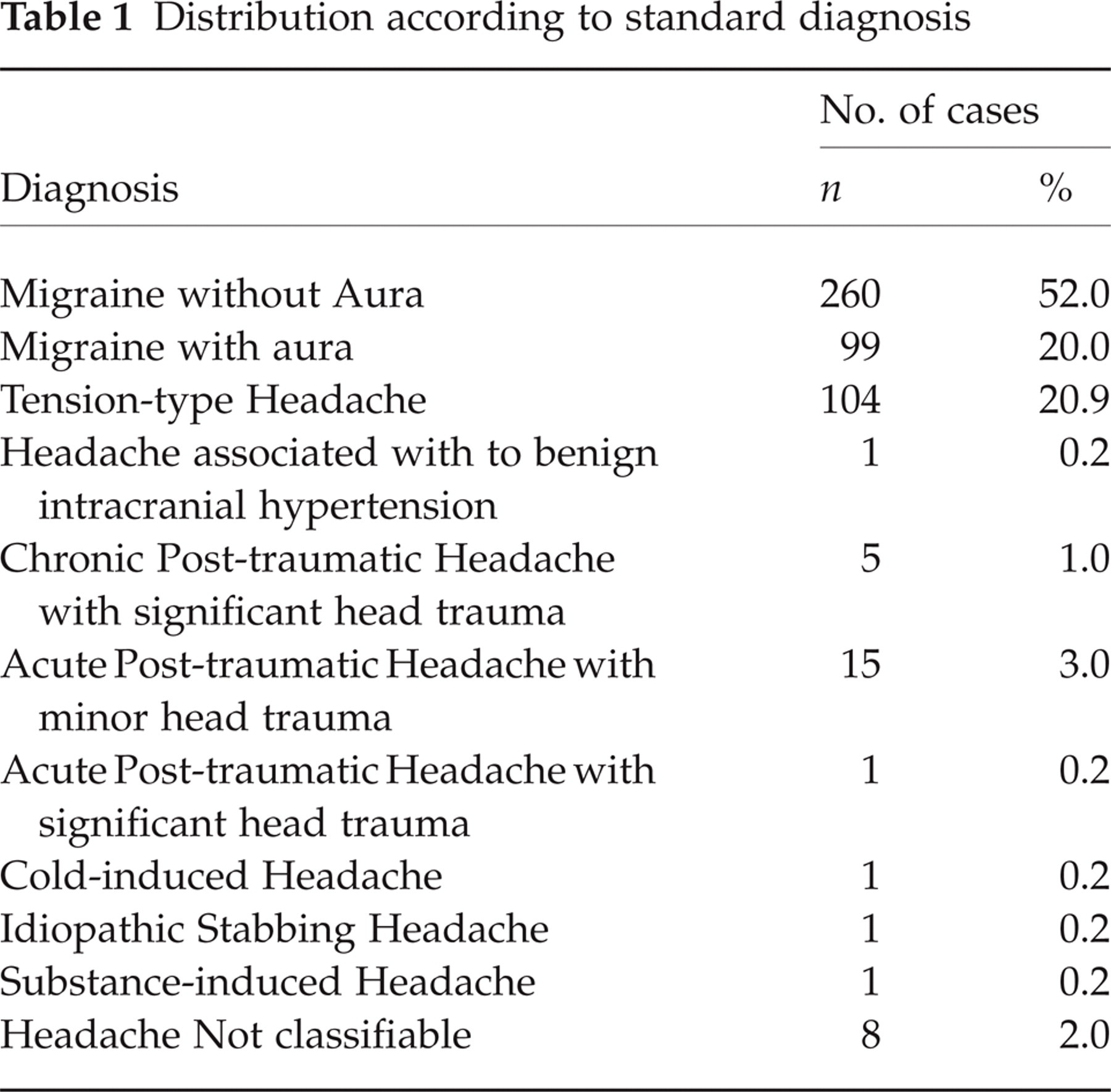
The results presented the following patient distribution related to primary headaches according to SD: migraine without aura 52%, migraine with aura 20%, tension-type headache 20.9% (Table 1). Although the findings concerning primary stabbing, cold induced, secondary and unspecified headaches were less prevalent, they are shown in Table 1, and the results were identical, when ICHD I-1988 and II-2004 were used. It is interesting to observe that 8 cases of headache not classifiable involved individuals who showed, at some time of their clinical history, a diagnosis of neurocysticercosis, but at the time of clinical evaluation, their headache was not due to this infection.
Distribution according to standard diagnosis
According to ICHD I-1988 (Table 2) there was reduction in migraine without aura to 11% and with aura to 5.2%. There was significant migration of patients previously diagnosed as migraine with and without aura by SD to migrainous disorder that does not meet criteria. Similar fact occurred with tension-type headache.
Distribution according to ICHD I-1988 Diagnosis

As for ICHD II-2004, 28% of patients were diagnosed as migraine without aura and 14.5% as migraine with aura (Table 3). Tension-type headache presented similar result to ICHD I-1988. The results for migraine in ICHD II-2004 comparatively to ICHDI-1988 tend to approach to the ones obtained by SD, since lower migration from migraine with and without aura to probable migraine was observed.
Distribution According to ICHD II-2004 Diagnosis

The ICHD I-1988 showed 21% and 27% Sensitivity for migraine without aura and with aura, respectively, and 100% Specificity for both. Whereas the ICHD II-2004 showed 53% Sensitivity and 100% Specificity for migraine without aura, and 71% Sensitivity and 99% Specificity for migraine with aura. The ICHD II-2004 diagnosis showed high specificity and greater sensitivity for migraine, when compared to the ICHD I-1988 diagnosis (Table 4).
Statistical test result
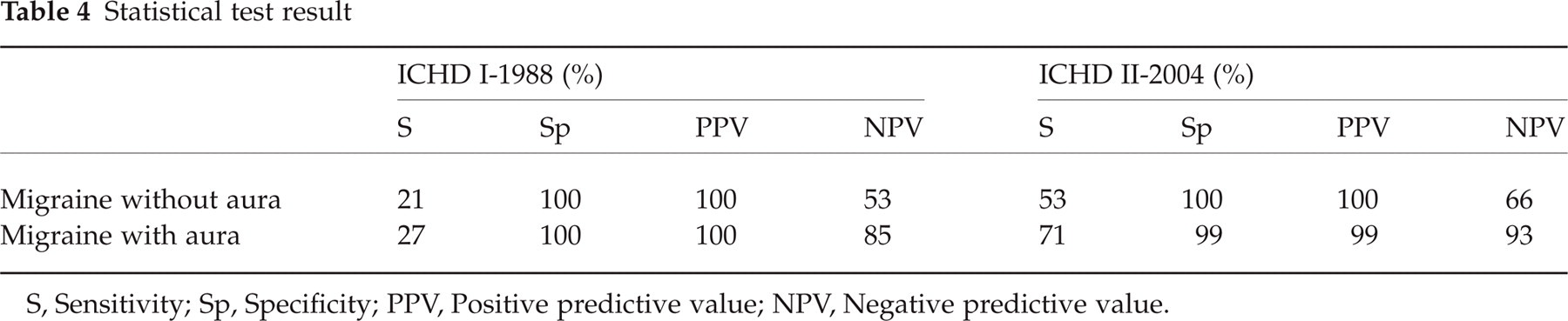
S, Sensitivity; Sp, Specificity; PPV, Positive predictive value; NPV, Negative predictive value.
When the group of patients diagnosed with migrainous disorder was associated with migraine with and without aura (ICHD I-1988), and the group diagnosed with probable migraine was also associated with migraine with and without aura (ICHD II-2004), the comparison of these big groups with our SD of ‘intuitive migraine’ (with and without aura) showed, respectively, 98% and 97% Sensitivity and 100% and 99% Specificity.
Discussion
Historically, the classification of headache of the Ad Hoc Committee (45) in 1962, did not include children and adolescents. The ICHD I-1988 classification included this age group, mentioning it in comments, but only regarding the minimum duration of migraine episodes without aura which lasting of crises changed from 4 h (adults) to 2 h (children and adolescents under 15 years old) (12, 13).
Several studies, even before the publication of the ICHD I-1988 criteria, observed that the duration of crises in children was shorter, and that it increased in adolescents (1, 4, 32). This was also confirmed during the validation of these criteria by several authors (14, 17, 19–21, 32–39).
Some authors have shown that IHS criteria are highly specific, but not very sensible (19–22, 32–39). Therefore, some authors consider that the intuitive clinical diagnosis, given by a specialist, should be the standard diagnosis (Gold Standard) (15, 17, 20, 29, 32). This suggestion is prone to criticism, since there is no be homogeneous standard diagnostic criteria, even thought it is valid and used in several studies. Other authors prefer the use of ICHD I-1988 criteria with a few specific modifications (33, 36, 40).
Because our standard diagnosis has considered duration of headache attacks shorter than one hour, there was a total percentage of patients with migraine attacks lasting less than 1 h much higher than in any other study (1, 4, 15, 17, 19–21, 32–39). The sleeping period was taken into account when the subjects fell asleep during an attack and woke up healed. This information was obtained from the patients’ charts and was given by parents or caretakers who described in several case, that the subject was recovered after taking a nap ranging 15–30 min.
When a patient meets all except one criteria, migraine is classified as migrainous disorder in ICHD I-1988 and probable migraine in ICHD II-2004. This study has found 57% of the cases (46) diagnosed as migrainous disorder and 30% (47) as probable migraine.
Most of the cases classified as migrainous disorder were reevaluated as having migraines, probably because the duration criterion in the standard diagnosis is highly flexible (duration of less than 30 min) or because the location (unilateral or bilateral). It was considered that children, especially the younger ones, take longer to inform their mothers about the pain, and when they are aware of the headache, the pain has probably been present for some time, ‘shortening’ the overall duration.
This may partially explain the relatively low results of ICHD I-1988 Sensitivity of the sample, in this study, for migraine without aura (S = 21%) when compared to other authors (32, 33), since their number is around 60% for ICHD I-1988 classification criteria, probably because they chose more strict duration criteria than the standard criteria used in this study. However, studies with Sensitivity as low as 27% were also observed, with results similar to the ones found in this study (39).
It's believed that the higher Sensitivity of ICHD II-2004 of the sample for migraine when compared to the ICHD I-1988 (S = 21%), was due to the duration and location criteria modification in the ICHD II-2004. Where, it was observed that the duration of headache attacks may last 1–72 h (reduction of 1 h comparing to ICHD I-1988) and the location might be unilateral or bilateral in children migraine (only unilateral in the ICHD I-1988) (42).
The result found when both groups (migraine with and without aura and migrainous disorder – ICHD I-1988, and migraine with and without aura and probable migraine – ICHD II-2004) were compared with intuitive migraine (SD), showed high specificity and higher sensitivity than the results previously described when the comparison did not include migrainous disorder or probable migraine. This finding was expected once the subjects diagnosed with migraine by standard diagnosis, were reclassified as migrainous disorder or probable migraine when submitted to ICHD I-1988 and ICHD II-2004, respectively.
As for the diagnosis of migraine with aura, ICHD I-1988 describes the general characteristics of headache, but does not list them in the diagnostic criteria (12, 13), allowing a free interpretation of the characteristics of headache observed in migraine with aura in general. The current classification ICHD II-2004 reviewed this point and described more extensively the migraines with aura. The item Typical Aura with Migrainous Headache was also defined, other algic characteristics were considered for migraine with aura so, two other subforms were also defined and differentiated: Typical Aura with Non Migrainous Headache and Typical Aura Without Headache. In addition to a better specification of Familial Hemiplegic Migraine and Sporadic Hemiplegic Migraine, the classification reports that in cases of aura with motor deficit, migraine should be listed under the item Hemiplegic Migraine as opposed to the ICHD I-1988 classification, which considered this type of aura as under Migraine with Typical Aura and did not include the item Sporadic Hemiplegic Migraine (42).
Every case of migraine with aura reported in this study presented migraine headache (typical aura with migrainous headache). No typical aura with non migrainous headache or without headache was observed.
The ‘intuitive clinical diagnosis’ might cause false positive diagnoses of migraine with aura, since migraine attacks might be accompanied by various neurological symptoms (premonitory symptoms) such as fatigue, difficulty in concentration, neck stiffness, blurred vision, yawning and pallor, which do not fulfil the criteria of migraine aura (42). The aura symptoms usually follow one another in succession beginning with the most common type of aura, that are visual symptoms with positive-scintillating figure or scotoma, and next, in frequency – sensory disturbances in the form of pins and needles moving slowly from the point of origin and affecting a greater or smaller part of one side of the body and face. Less frequent are speech disturbances and motor weakness.
Although the ‘intuitive clinical diagnosis’ were used in this work as standard diagnosis, there were no difficulties to identify migraine with aura in this study, using the headache diary to facilitate the separation between premonitory symptoms and aura (except for the description of the duration of aura, especially in younger children, when the duration is at times unclear), however, doubtless of its characterization (38, 39).
In conclusion, the results have clearly shown that the ICHD II-2004 diagnosis has high specificity and greater sensitivity for migraine, when compared to the ICHD I-1988 diagnosis. It was observed that in the 16 years elapsed between the ICHD I and ICHD II classifications, there was an addition for migraine in children, and a better definition of migraines with aura and the headaches that may follow it. In our opinion the current classification ICHD II-2004 promoted improvement and advance for children and adolescents migraine diagnosis, although it remains with poor sensitivity (53–77%).