
Abstract
Introduction
Migraine has a considerable social, economic, physical and emotional burden but remains underdiagnosed and undertreated. A specific migraine screening tool could help remove barriers to health care and be an attractive instrument for epidemiological studies. The objective of this work was to assess the validity of an extended French version of ID Migraine™ as a migraine-screening tool.
Methods
Sixty-seven subjects from the NESCaV study (2010–2012) completed the migraine screen and were diagnosed by a neurologist specializing in headache medicine using the International Classification of Headache Disorders, 2nd edition criteria (gold standard). Agreement between the two diagnoses was evaluated by Cohen kappa coefficient (κ). Sensitivity, specificity and predictive values of the migraine screen were calculated.
Results
Migraine was diagnosed in 21 (31.3%) of the 67 subjects according to the screening tool and in 24 (35.8%) by the neurologist (κ = 0.90). The prevalence of migraine was unrelated to age, gender, education and perception of financial resources. Sensitivity and specificity of the screen were 87.5% and 100%, respectively. The screen prevalence of migraine with aura was 10.4% (sensitivity and specificity: 83.3% and 96.7%, respectively).
Conclusion
The extended French version of ID Migraine™ (ef-ID Migraine) is a validated tool to screen migraine in French-speaking countries.
Introduction
Migraine is a highly prevalent and disabling neurological condition interfering in everyday life with employment, household work, and social activities. About 15% of European adults (8% of men and 17% of women) suffer from migraine. The cost of migraine in Europe is estimated at €27 billion/year including direct and indirect costs due to the high prevalence of the disorder (1). About a quarter of adult migraine sufferers experience migraine with aura (MA). MA is characterized by transient neurological symptoms, classically scintillating scotoma, occurring before or at the beginning of the headache (2). The 12-month prevalence of MA across studies is 4.4% (range: 1.2%–5.8%) (3). Migraines with and without aura remain under-diagnosed and undertreated throughout the world (4,5). A valid screening tool implemented through a brief self-administered questionnaire could help remove barriers to health care and hence improve treatment (5). Moreover, a self-administered questionnaire is an attractive instrument for epidemiological studies, being inexpensive and relatively easy to use (6). The diagnosis of migraine is based on a combination of symptoms (headache characteristics and associated symptoms like photophobia or nausea) that are defined by the International Classification of Headache Disorders, 2nd edition (ICHD-II) (7) and easily captured by questionnaires (8). The ID Migraine™ self-administered screening instrument, which consists of only three items, is a validated and reliable tool, recommended as a simple method for diagnosing migraine in primary care settings (9). No such validated tool exists in French.
The objective of this study was to develop, in French, a short and practical migraine screening tool based on the ID Migraine™ screen. If validated, such a screening tool will be useful to estimate the prevalence of migraine in French-speaking populations and to identify MA.
Methods
Study population
The Nutrition, Environment and Cardiovascular Health (NESCaV) survey was a cross-sectional population-based survey of cardiovascular risk factors conducted between May 2010 and March 2012 in the province of Liège (Wallonia, Belgium) on a sample of 1017 presumably healthy subjects. The sample was stratified by gender, age (classified in five-year categories) and district of residence (Liège, Huy, Waremme, and Verviers). Pregnant women, people living in institutions, and individuals outside the age range of 20–69 years were excluded (10). The protocol of the NESCaV study was approved by the ethics committee of the Faculty of Medicine of Liège University (B70720097541). Most participants (n = 751) of the NESCaV survey filled in the new migraine-screening tool but only 67 (8.9%) of them were diagnosed with migraine (with or without aura) by the neurologist (J.S.) depending on his availability in the hospital. These 67 subjects constituted the study material. The clinical diagnosis of migraine was made according to the criteria of ICHD-II (7) and was considered as the gold standard hereafter. The use of the ID Migraine™ screen was authorized by its author, R. Lipton.
Design of the questionnaire
The French version of the new screening tool was based on the ID Migraine™ screen developed and validated in the United States (US) by Lipton et al. in 2003 (9). In primary care settings, the ID Migraine™ had a diagnostic sensitivity and specificity of 81% and 75%, respectively. Its positive predictive value (PPV) amounts to 93% for the clinical diagnosis of ICHD-I migraine (9). The three items of the screen record the presence or absence within the last three months of a disabling headache (inability to work, study, or do what you need to do for at least one day) accompanied by photophobia and nausea (9,11).
The modified “French version” of the ID Migraine™ screener (with English translation).
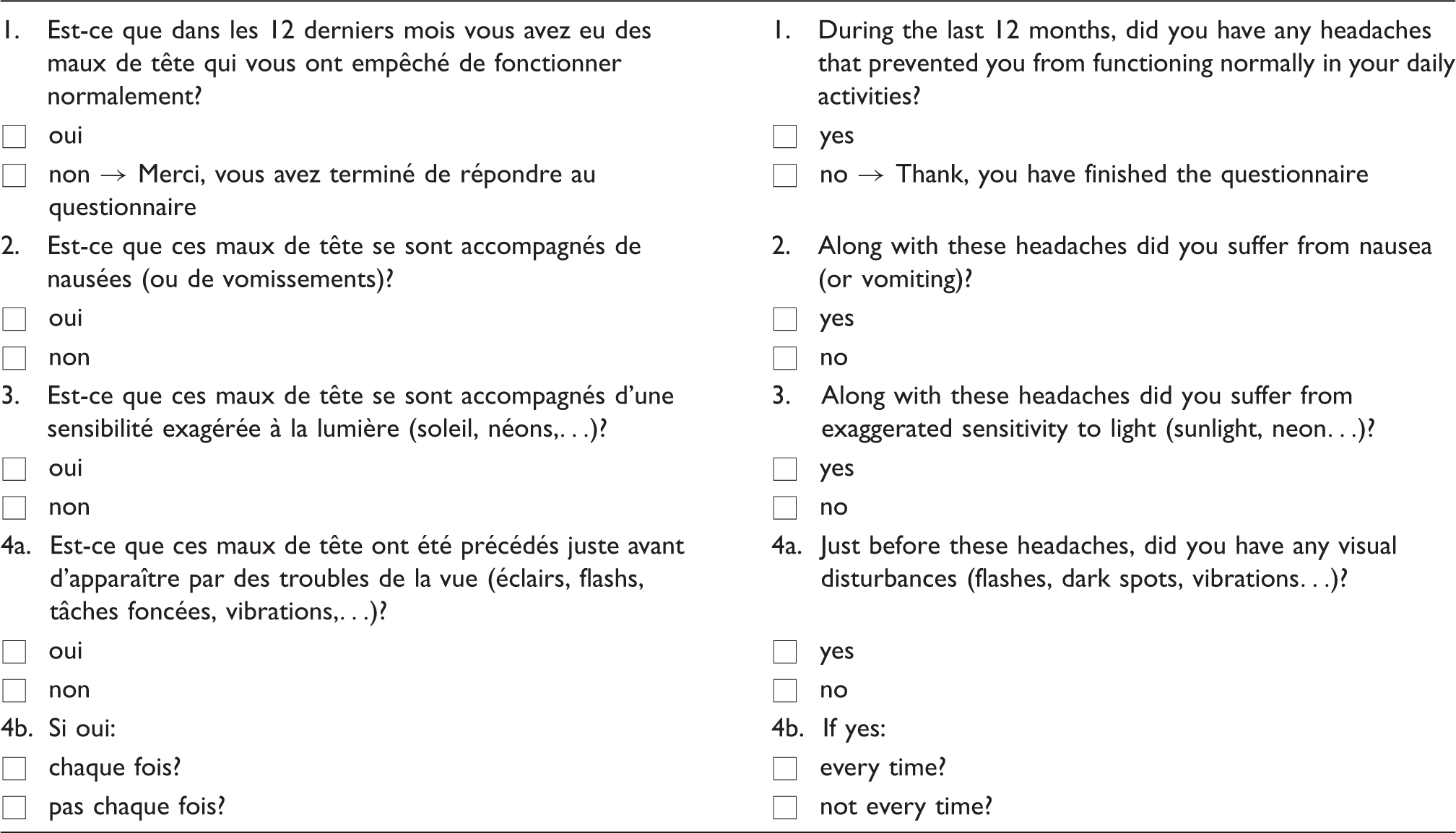
Subjects who answered “yes” to question 1 were classified as “headache sufferers.” Those who answered “no” constituted the control group. Further headache sufferers were classified as having migraine (migraineurs) if they answered “yes” for nausea/vomiting (question 2) and/or photophobia (question 3) and/or visual disturbances before headache (question 4). Migraineurs were classified as having MA if they responded positively to visual disturbances before headache.
Statistics
Results for demographic characteristics were expressed as counts and percentages for categorical variables. The Chi-square goodness-of-fit test was used to compare the characteristics of the study subsample and the NESCaV population. To compare the responses of the 67 study subjects with those of the NESCaV participants who filled in the new migraine screening questionnaire but were not seen by the neurologist, the classical Chi-square test was applied. The prevalence of migraine was estimated with 95% confidence interval (95% CI) and its relation with age, gender, educational level and perception of financial resources was tested by logistic regression analysis. Sensitivity, specificity, PPV and negative predictive values (NPV) of the screening tool were calculated with 95% CI, according to the diagnosis based on ICHD-II criteria. Cohen kappa coefficient with 95% CI was used to assess the degree of concordance between the screen and the gold standard. The significance level was set at p < 0.05. All calculations were performed with the SAS statistical package (version 9.3 for Windows).
Results
Subjects
Demographic characteristics of the study sample and of the Nutrition, Environment and Cardiovascular Health (NESCaV) survey study population.

New migraine screening questionnaire
Distribution of answers to the new migraine screening questionnaire for study subjects and Nutrition, Environment and Cardiovascular Health (NESCaV) survey participants who filled in the questionnaire but were not diagnosed by the neurologist.

Validity of the screening tool
The neurologist diagnosed migraine in 24 of the 67 subjects, yielding a prevalence of 35.8% (95% CI: 24.3–47.3). Prevalence did not differ between women and men (38.5% vs. 32.1%, p = 0.80) and was not related to age (p = 0.17). Among the 24 migraine sufferers, six (four women and two men) had MA, leading to a prevalence of 9.0% (95% CI: 2.1–15.8).
When considering the new screening tool, 21 subjects were classified as having migraine, giving a prevalence of 31.3% (95%CI: 20.2–42.5). Cohen kappa coefficient was equal to 0.90 (95% CI: 0.79–1.0), indicating an excellent agreement between the new screening tool and the gold standard. The prevalence did not differ between women and men (38.5% vs. 21.4%, p = 0.22) and was unrelated to age (p = 0.18). Seven subjects (three men and four women) were identified as MA, yielding an overall prevalence of 10.4% (95% CI: 3.1–17.8). Cohen kappa coefficient was equal to 0.74 (95% CI: 0.47–1.0).
No association was found between migraine prevalence, whether diagnosed by the neurologist or the screening tool, and level of education or perception of financial resources.
Validity of the new migraine screening tool.

CI: confidence interval; PPV: positive predictive value; NPV: negative predictive value; MA: migraine with aura.
For MA, sensitivity was 83.3% and specificity 96.7% with a PPV and an NPV of 71.4% and 98.3%, respectively.
Discussion
The present study was designed to validate an extended French version of the ID Migraine™ (or “ef-ID Migraine”) screen self-administered questionnaire. The new migraine-screening tool was also intended to be used by general practitioners in the primary care setting and in epidemiological studies by researchers. General practitioners and researchers may indeed not be familiar with the detailed criteria of ICHD-II which could advantageously be replaced by this novel quick, easy to use and inexpensive screening instrument.
The ef-ID Migraine is a valid screening tool for migraine with a high degree of agreement between self-reported migraine and migraine diagnosed by a neurologist. Since we found a high degree of agreement (14) between reported and clinically diagnosed migraine, ef-ID Migraine can be used to estimate the prevalence of migraine. It is a screening tool, not a diagnostic instrument, because of the rather high false-negative rate of 12.5%. Because the first question helps identify subjects with disabling headaches in the last year, the tool selects subjects with active migraine, which somewhat reduces its sensitivity but increases specificity. Concordantly false positives were absent in our survey for migraine without aura. The first three items of ef-ID Migraine about headache disability, nausea and photophobia are similar to those of the English ID Migraine™. General practitioners and researchers could use them as a fast and effective instrument for screening migraine.
Compared to the original ID Migraine™ validation study (9) and other studies of validation of this questionnaire in other languages, e.g. Italian, Portuguese and Turkish (15–17), the performance of ef-ID Migraine in our study was similar with comparable sensitivity but higher specificity. The observed differences in performance between studies can result from the study design. The validation study of the original ID Migraine™ used the first edition of the International Classification of Headache Disorders (ICHD-I) as the gold standard (9). In our study, we used ICHD-II as the gold standard, but this should not markedly impact the results, as the diagnostic criteria for migraine are identical between the two editions. Moreover, these validation studies were conducted with patients referred to specialized headache centers (9,15,16), while in our study we used a sample of supposedly healthy subjects from the general population. Testing a clinical sample of headache patients could bias the results toward a better performance of the migraine-screening tool.
Recently, a new migraine-screening questionnaire intended to be used in clinical practice and research in the general population, the Migraine Screen Questionnaire (MS-Q), has shown excellent efficacy, with sensitivity, specificity, PPV and NPV all greater than 80.0%. The tool consists of five items: frequency and intensity of headache, duration (between four hours and three days), nausea, sensitivity to light/noise, and disability. Unfortunately, the development and validation of the instrument was not conducted on a general population sample and it might therefore not be easily generalized (18).
Many other questionnaires for screening migraine exist. However, it is important to keep in mind that an instrument must be chosen with caution depending on the desired performance and objectives of the screening (19). Indeed, depending of the setting (specialty referral settings, general population or primary care), the requested screening instrument for migraine may probably need to be adapted. Several studies did not have optimal expert confirmation of the migraine diagnosis. Others developed instruments that either had unfavorable performance characteristics or were too time consuming for routine use (9,19).
In a recent meta-analysis, MA was found to be an independent relative risk factor for ischemic stroke, particularly in women (12). To assess the risk of stroke, physicians must therefore take MA into account in patient history. The ef-ID Migraine was developed to detect MA and could therefore help primary care physicians to integrate this risk factor into stroke risk management. In our study, the screening of MA had a good sensitivity and specificity. This was clearly higher than the 43% sensitivity and 74% specificity reported by Lipton et al. (9). The different wording of the question intended to identify visual auras and the small number of cases of MA in the current study could explain the difference in performance between the two screening questions.
The study presents some strengths and limitations. First, it used a representative stratified sample from the NESCaV study population (N = 1017). Secondly, validation was conducted on a presumably healthy population, which limits a possible selection bias. Indeed, when validations are conducted in specialty referral settings, patients are more likely to be aware of their disease and concordance likely to be higher.
The first question of the ef-ID Migraine screening tool can be associated with a recall bias. Since the period of assessment concerns the last 12 months, some subjects might have forgotten a remote episode of migraine. The relatively small number of subjects (n = 67) represents another limitation of our validation study; however, the responses to the questions of the ef-ID Migraine did not really differ between the study subjects (n = 67) and the other participants who completed it (n = 684). Moreover, the ef-ID Migraine did not behave differently according to age, gender, educational level and perception of financial resources.
Conclusions
In conclusion, the extended French version of ID Migraine™ can be seen as a valid and easy-to-use migraine-screening tool. It is particularly appropriate for epidemiological studies of migraine prevalence in French-speaking countries. Further studies are needed for its validation in primary care settings and for the validation of the MA screening question.
Clinical implications
The extended French version of the ID Migraine screen (ef-ID Migraine) can be reliably used to screen migraine in French-speaking countries. The ef-ID Migraine includes a question for screening migraine with aura, which is of clinical importance because of the strong relation between MA and cardiovascular diseases.
Footnotes
Funding
The current study was an ancillary study of the NESCaV survey project, supported by INTERREG IV A program, “Greater Region,” 2007–2013. It was co-funded by the European Regional Development Fund (ERDF) (NESCAV N° 39/GR/3/3/056), the Walloon Region and the University of Liège in Belgium.
Conflict of interest
None declared.
Acknowledgment
The authors are grateful to Dr Richard Lipton for allowing the use of ID Migraine™ in this study.