
Abstract
Morbidity and mortality of acute poisoning is a major serious health issue in the world. Paraquat is seriously known to be responsible for acute poisoning. The study aims to present the various aspects, including the epidemiological profile, clinical presentation, analysis of poisoning, outcome and cause of death. This is hospital based, prospective study of all the confirmed cases of paraquat poisoning. The paraquat poisoning patients were presented to the Emergency Department, Mamata General Hospital, attached to Medical College, Khammam, a one year study period from January 2022 to December 2022 was studied. A total of 16 paraquat poisoning cases were admitted during the study period. Complete data were collected and analysed from patients,attendants and hospital records. A total of 102 poisoning cases were admitted, out of which paraquat poisoning cases, 16 men were most involved. In this study, it was shown that most cases were reported from urban, married people.
Paraquat is widely marketed and easily available. The lack of availability of a specific antidote increases the paraquat fatality. The most common cause of death is respiratory failure. Paraquat causes renal failure by causing hypovolemia, circulatory failure, septicemia, and direct toxicity leading to multiorgan failure. The present study determines the most vulnerable age group, 31–40 years, males, married people from rural populations belonging to low socioeconomic strata. Most of people are employed in the agriculture sector. Most of the victims committed suicide due to financial problems.
Introduction
Paraquat, a herbicide and weed killer of the bipyridyl group, is widely encountered. Paraquat (C6H7N2]CL2) chemical composition is 1,1’-Dimethyl-4,4’-bi-pyridinium. It is commercially available in India in liquid form as GRAMOXANE (10%–30% conc) and in granule form as WEEDOL. 1 This toxic substance quickly gets absorbed through skin and mucus membranes and imparts cytotoxicity through free radical injury. As the highest concentration is found in lung tissue, pulmonary toxicity followed by liver damage is the main terminal pathology. 2 As little as a teaspoon of a concentrated amount of paraquat can result in death. In an adult human, the estimated fatal dose is about 30 mg/kg or 3–6 grams of paraquat ion, which is equivalent to 10–20 ml of 20% solution of paraquat. 3
Aims & Objectives
The main aim of the present study is to describe the demographic profile, including seasonal variation, time, place of consumption, amount of poison consumed, manner of poisoning, clinical presentation, outcome, and cause of death.
Materials & Methods
This prospective study was conducted in an Emergency Department at Mamata General Hospital, the study period was one year from January 2022 to December 2022, in Khammam, Telangana. This prospective study was conducted in an Emergency Department at Mamata General Hospital, the study period was one year from January 2022 to December 2022, in Khammam,Telangana.
Study Design
During this hospital-based study, a total of 106 poisoning cases were admitted, out of which 16 were Paraquat poisoning cases.
Study Population
All confirmed 16 paraquat poisoning cases were included in the present study as the study participant/population.
Inclusion Criteria
In the present study, paraquat patients who were presented to the casualty were considered, diagnosed, and confirmed paraquat poisoning cases were included as study samples, for one year between January 2022 and December 2022.
Exclusion Criteria
Criteria for the selection of cases, involving trauma, drugs, other poisons, asphyxia, diseases, unknown poison, and decomposition cases were excluded. The exclusions mentioned above are external factors that do not justify paraquat poisoning.
Sample Size
A prospective study was conducted in an Emergency Department at Mamata General Hospital. The study period was one year, from January 2022 to December 2022, in Khammam, Telangana, and a total of 16 paraquat poisoning cases were admitted during the study period.
Statistical Data Analysis
Proforma prepared, prospective data were collected from the patient, patient’s relatives, and hospital records, who received treatment regarding the demographic characteristics, occupation, time, place and amount consumed, symptoms, target organ damage, manner poisoning, outcome, histopathological changes, and cause of death were systematically analysed and results were tabulated.
Observations/Results
One hundred and two poisoning cases were admitted to the emergency department during the study period, of which 16 cases were diagnosed as paraquat poisoning cases, accounting for 1.56%. When compared with previous studies, the incidence has increased, which shows that the misuse of the paraquat has increased a lot.
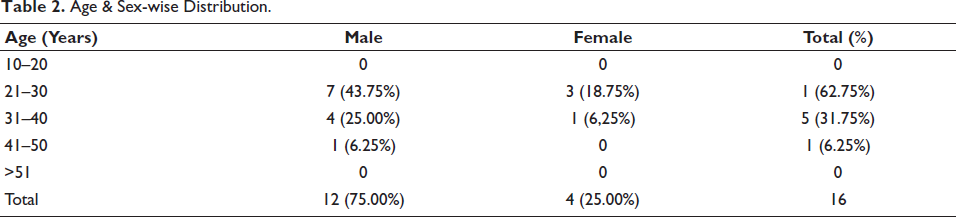
Most of the victims were young adults between 21 and 30 years of age, 10 (62.75%) in both genders, followed by 31–40 years, 5 (31.75%) as depicted in Table 1.
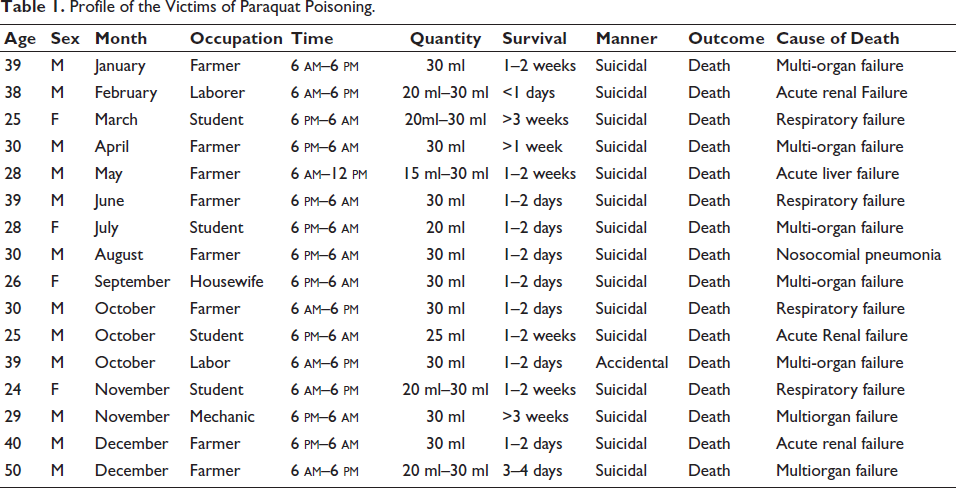
Profile of the Victims of Paraquat Poisoning.
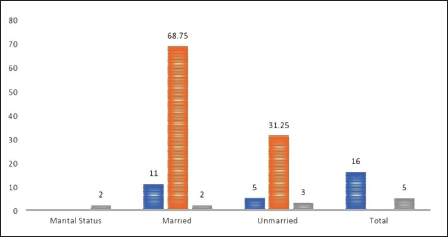
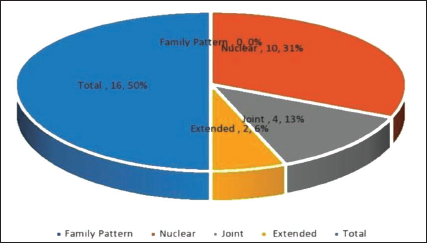
In our study, the male population 12 (75.00%) predominates the female population (25.00%) as depicted in Table 2. Most of the victims 11 (68.75%) were married people, whereas 5 (31.25%) were unmarried people, as depicted in Figure 1. In the present study,10 (62.50%) belonged to a nuclear family, 5 (31.25%) were from a joint family, and the rest 1 (6.25%) belonged to an extended family depicted in Figure 2.
Age & Sex-wise Distribution.
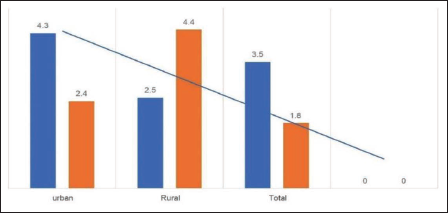
The present study showed that paraquat poisoning was more common in rural than urban populations. Out of the 16 cases studied, 12 (75.00%) were from rural backgrounds and 4 (25.00%) were from urban populations as shown in Figure 3.
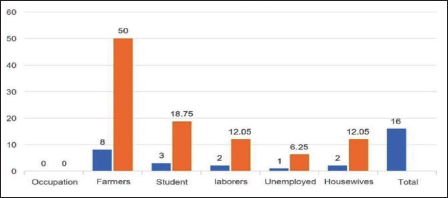
We observed that the poisoning and its fatality were found to be more common and prominent in the people employed in the occupation of agriculture 8 (50.00%) of them were farmers, 3 (18.75%) were students, next laborers were 2 (12.05%) cases and 2 (12.05%) were housewives. Only 1 (6.25%) case was unemployed, as depicted in Figure 4.
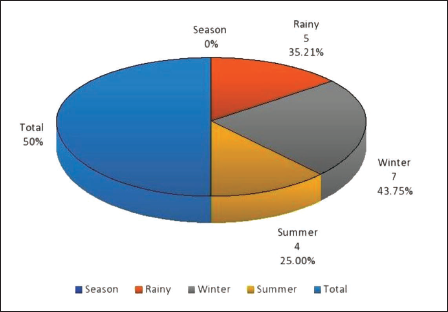
The present study showed that out of 16 cases, the highest number of cases were reported during the rainy season 7 (43.75%) followed by winter 5 (35.21%), and 4 (25.00%) cases were reported during summer as depicted in Figure 5. Month-wise, cases reported the highest number of cases during the last quarter of the year, which is October to December, with 7 (43.75%) cases. Each month, only one case was reported from January to September, as in Table 1.
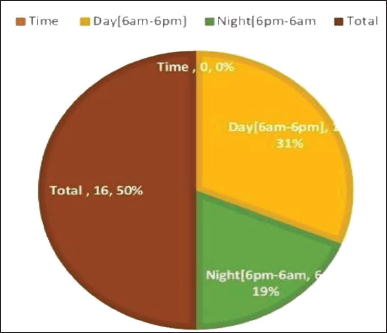
The present study noted that the highest number of 10 (62.50%) cases were consumed poison during the morning hours between 6 am and 6 pm, while compared to nighttime (6 pm–6 am), 6 (37.50%) showed in Figure 6
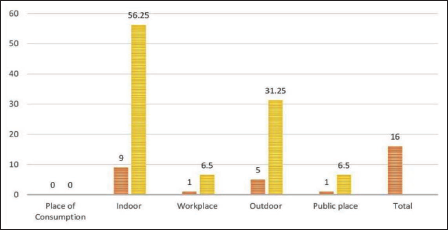
The present study found that the most common place of poison consumed at their residency was indoors, 9 (56.25%) than outdoors 5 (31.25%) as depicted in Figure 7.
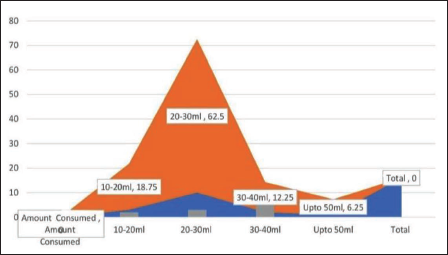
In this study, observed that the exact dose of paraquat amount ingested was noted in detail in all 16 patients, the same amount consumed is based on the history given by patient/attendants, and the amount consumed was approximately 20–30 ml in 10 (62.50%) cases,10–20 ml in 3 (18.75%) cases, 40–50 ml in 2 (12.50%) cases, and more than 50 ml in 1 (6.25%) case were respectively as depicted in Figure 8. The Paraquat concentration is present in the consumed liquids, ranging from 5% to 30%.
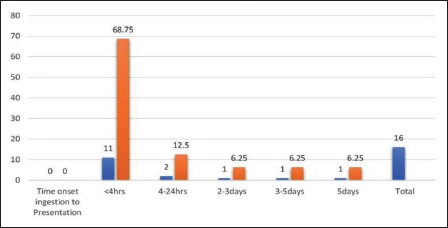
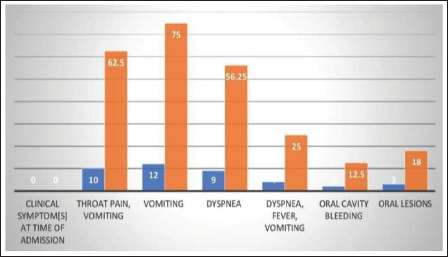
The present study showed that in most cases, in 11 (68.75%) cases where the time of onset of ingestion to the presentation of poison is less than four hours, while 4–24 hours after ingestion in 2 (12.50%) cases, as shown in Figure 9. In this present study, the commonest presented symptom after ingestion of paraquat included vomiting in 9 (75.00%) cases, followed by difficulty in breathing in 4 (25:00%) cases. One patient (6.25%) was febrile at admission, as depicted in Figure 10.
Our study on clinical examination showed oral cavity erosions in one patient (6.25%) and icterus in one patient (6.25%). The results of clinical presentations and the key laboratory investigations are the pattern of organ involvement and mortality assessment in paraquat poisoning.
In this study, in almost all patients, the manner of paraquat poisoning is in a suicidal manner in 15 (93.75%) cases and accidental in 1 (6.25%) case.
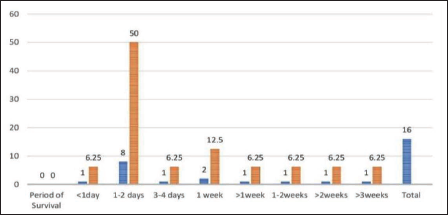
In the present study, the overall survival period of post-paraquat consumption ranged from 10 hours to 25 days, as shown in Figure 11. In the present study, of the total fatalities, eight patients (50.00%) survived in 24–48 hours, and at least two patients (12.50%) survived one week. The outcome of the cases, in the present study, we observed that almost all 15 patients died.
On analysing the cases for organs involved, the stomach was affected in 15 (9375%) cases, the lungs were affected in 15 (93.75%) cases, the liver in 14 (87.50%) cases, and the kidneys in 10 (62.50%) cases.
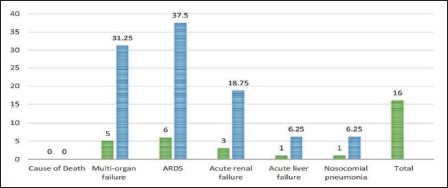
The underlying cause of death was a multi-organ failure in 6 (37.50%) patients, followed by acute respiratory distress syndrome in 5 (31.25%) patients and acute renal failure in 3 (18.74%) patients. In the remaining two patients, one is acute liver failure and another one is nosocomial pneumonia, as depicted in Figure 12.
On autopsy, the brain was congested and edematous, and visceral organs showed marked congestion in all cases. Lungs were congested with marked pulmonary edema in 10 cases. Erosion due to the corrosive action was present in the oral mucosa, tongue, esophagus, and stomach. Mainly all three vital organs were affected (lungs, liver, and kidneys). Histopathological analysis revealed changes like ulceration of the gastric mucosa, pulmonary edema in the lungs, centrilobular necrosis in the liver, and acute tubular necrosis in the kidneys.
Discussion
In the present study, a total of 16 paraquat cases were admitted during the study period, which confirmed paraquat poisoning was included in the present study. The incidence of paraquat poisoning is 16 (15.68%). Similar observations were noted by other studies.3–5 The incidence of paraquat poisoning revealed that there has been a threefold increase, compared to past studies. This increase has to be considered as the poison is easily available over the counter, with unrestricted access, and the fatality of the poison is much higher.
Most of the victims of paraquat poisoning were young adults between 21 and 30 years of age, 10 (62.75%) in both genders, followed by 31–40 years 5 (31.75%), and 1 (6.25%) case reported in the age between 41 and 50 years. No cases were reported between 10 and 20 years or more than 50 years. These are consistent with the author’s studies.4–6 Young men married who encounter hardship in their lives, and if they fail to achieve the required goals, consume poison and end their lives. Similar results were seen in other studies too.
In the present study, the paraquat poisoning cases where males predominate 12 (75.00%) than females 4 (25.00%). These are consistent with other studies.4–6 The male-to-female ratio was found to be 3:1.
The present study showed that most of the victims are from the rural population 12 (7500%) than the urban population 4 (25.00%), supported by authors’ studies.5, 6
In the present study, most patients are married people 12 (75.00%) compared to unmarried people 4 (25.00%), who encounter hardship in their lives. These findings were similar to those of other studies.6, 7
A maximum number of paraquat victims 10 (62.50%) belonged to the nuclear family when compared to the joint family 5 (31.25%). Similar findings are observed by Indian authors.6–8
In the present study, most of the victims 8 (50.00%) were farmers and the remaining were students 3 (18.00%), 2 (12.05%) housewives, and laborers 2 (12.05%). These findings are consistent with other author studies.7–9 This percentage is higher than in other parts of the country, such as Meerat and Punjab.
The present study showed that out of 16 cases, the maximum number of cases reported during winter was 7 (43.75%) followed by the rainy season 5 (35.21%) and 4 (25.00%) cases reported during summer. These observations are like the other studies.8, 9 Month-wise, cases reported most cases were during the last quarter of the year, that is, October to December months, 7 (43.75%) cases, and each month one case only reported from January to September months. Similar observations are made in studies carried out by authors.8–10
The highest number of patients who consumed paraquat in the daytime was 10 (62.50%) while the nighttime 6 (37.50%). These findings were like the other studies.9–11 Most of the victims consumed paraquat at their residence 9 (56.25%) as compared to outdoor 5 (31.25%). These are consistent with the authors.9–11
The exact dose of paraquat ingested in the present study was noted in detail. Based on the history given by patients/attendants, the amount consumed was approximately 20–30 ml in 10 (62.50%) cases, 10–20 ml in 3 (18.75%) cases, 40–50 ml in 2 (12.50%) cases, and more than 50 ml in 1 (6.25%) case, respectively. This was similar to the study of the authors.10–12
In our study, we observed that the amount of ingested paraquat was stated by patients/relatives as a mouthful, cap of a container, and all or part of a mug or cup. We consider the volume of a mouthful amount equal to 30, a normal mug, and a cup equal to 150–250 ml, respectively. These findings are like other studies.11–13 The volume of a sample of 1 l paraquat container cap was measured as 25 ml. In the existence of a remainder of ingested poison, we estimated the ingested volume by directly measuring the residual volume and asking for recent or previous use of poison. The concentration of paraquat present in the consumed liquids ranged from 5% to 30%. We observed that the majority of paraquat victims consumed a fatal dose between 20 and 30 ml of paraquat. The prognosis of the patient hugely depends on the amount of paraquat poison consumption. Although the WHO has estimated the lethal dose of paraquat for humans to be 30–50 mg/kg, even lower doses may be fatal among children.
The present study noted that the common presenting symptoms after ingestion of paraquat poison included vomiting in 9 (75.00%) patients, followed by difficulty in breathing in 4 (25.00%) patients. One patient (6.25%) was presented with febrile at the time of admission. On clinical examination, the present study showed oral cavity lesions in 1 (6.25%) patient and icterus in 1 (6.25%) patient. Paraquat, when consumed, causes ulceration and erosion of the oral mucosa, tongue, esophagus, and stomach. These are consistent with many Indian authors.12–14
Our study observed that ingestion of paraquat was for deliberate self-harm or suicide in 15 (93.75%), and accidental in 1 (6.25%). The present study observed that almost all patients ingested paraquat orally, and other routes of paraquat poisoning were not shown. These are similarly supported by studies carried out by authors.12–15
We observed that the overall survival period of post-paraquat consumption ranged between 10 hours and 25 days. Of the total fatalities, eight patients (50.00%) survived in 24–48 hours, at least two patients (12.50%) one week. Similar findings are made by other studies.16, 17 For the surviving patients, the average amount of ingested paraquat is 25 ml. Prolonged exposure can cause gastric/esophageal perforations and pancreatitis. Paraquat is exceedingly toxic to humans, and as little as one teaspoonful of the active ingredient may be fatal, with death known to occur as late as 30 days after ingestion.
The present study outcome of the victims showed that almost all 16 (100.00%) patients died. Paraquat toxicity at a cellular level is due to redox cycling and intracellular oxidative stress generation by the accumulation of superoxide anion, hydrogen peroxide, and hydroxy radicals. These are consistent with other studies.17–19 The corrosive action is not present in other pesticides, as a result, gastric lavage is not routinely performed in such cases. The prognosis of the patient hugely depends upon the amount of consumption.
On analysing the cases for organs involved, the stomach was affected in 15 (93.75%) cases, the lungs were affected in 15 (93.75%) cases, the liver in 14 (87.50%) cases, and kidneys in 10 (62.50%) cases. Similar observations are made by many studies.17–20 On ingestion, paraquat is rapidly but incompletely absorbed and is rapidly distributed to the lungs, liver, kidneys, and muscles. Due to corrosive action, erosion was present in the oral mucosa, tongue, esophagus, and stomach. It also causes acute tubular necrosis in the kidneys and thereby causes acute kidney injury. It affects the liver and causes centrilobular necrosis and ischemic changes. In the lungs, it causes pulmonary edema and later stages fibrosis.
The present study showed that most patients died from organ failure in 6 (37.50%) cases, followed by acute respiratory distress syndrome in 5 (31.25%) cases, acute renal failure in 3 (18.74%) cases and the remaining cases were acute liver failure in one case and nosocomial pneumonia one case. Ingestion at high doses is known to injure other organ systems like the kidneys, liver, and heart, with death in most cases resulting from respiratory or multi-organ failure. Which are supported by studies carried out by authors.18–21
On autopsy, the brain was congested and edematous, and visceral organs showed marked congestion in all cases. Lungs were congested with marked pulmonary edema in 10 (62.50%) cases. Due to corrosive action, erosion was present in the oral mucosa, tongue, esophagus, and stomach. Similar findings are made by the authors’ studies carried out in India.19–22 All fatal cases had many similarities including the history of consumption of large amounts, ventilator support from day one, and all three vital organs were affected (lungs, liver, and kidneys). Histopathological analysis revealed similar changes like ulceration of the gastric mucosa, pulmonary edema in the lungs, centrilobular necrosis in the liver, and acute tubular necrosis in the kidneys.
In all the cases, viscera were sent for analysis, and out of 16 reports obtained,16 were positive. These are consistent with other studies.20–23 Hemodialysis and hemoperfusion can be done, and Immunosuppressive drugs and opiates may also be given. Emetics, cathartics, and oxygen are contraindicated.
Conclusion
All the paraquat poisoning cases should be treated as medical emergencies. When compared to other pesticides, paraquat is the most dangerous of all, with a maximum fatal rate.
Treatment protocol for paraquat poisoning should be framed, and it is better to implement stringent rules in the sales than to struggle in the treatment part of it.
There must be further research to develop adequate tests to determine the presence of paraquat toxicity in live or deceased patients, as the postmortem features are grossly vague and resemble multi-organ failure. Paraquat toxicity should be considered in case of an unexplained combination of respiratory, and gastrointestinal symptoms and acute renal damage, even in the absence of a proper history of paraquat consumption.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Informed consent statements have been taken from all the patients and were submitted to Institutional Ethics Committee and got approval (Ref. No. IEC/IRB/MMC/25/22).
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Informed consent statements have been taken from all the patients.