
Abstract
Paraquat, an essential tool for farmers for more than 50 years, is also a leading cause of fatal poisoning in underdeveloped countries. Consuming this lethal herbicide can affect multiple organ systems the most common being the respiratory and renal system. However, in the recent times, we have seen a drastic rise in the number of cases associated with cardiovascular abnormalities and with acute myocardial infarction as a complication.
Lack of effective treatment and high potency of paraquat has made early diagnosis of prime importance. Here we present to you a case of paraquat poisoning and its correlation with myocardial injury.
Further through this report we intend to frame a hypothesis on the mechanism by which paraquat poisoning affects the cardiovascular system.
Thus, hospitalisation and close cardiac monitoring becomes essential in the treatment of paraquat poisoning.
Introduction
Acute myocardial infarction (MI) is a fatal disease that takes the lives of millions every year. Eliciting adequate history, performing necessary clinical examinations and interpreting laboratory results effectively remain crucial in diagnosing a MI. The exact aetiology of MI remains incompletely understood; however, research suggests that the condition has several predisposing factors including hypertension, hyperlipidaemia, cigarette smoking (modifiable) and family history, age and gender (non-modifiable). While a diverse group of aetiologies has been proposed, one such aetiology ‘paraquat poisoning’ remains understudied. We hereby report a case of an 18-year-old boy from Shivamogga, a city in Karnataka State, Southwest India, with acute MI secondary to paraquat poisoning. He had no history of high blood pressure, smoking or anything that could suggest a MI.
Paraquat poisoning is one of the fatal poisoning cases in many underdeveloped countries in Asia, Central America and the Pacific Islands. 1 Paraquat (N,N’-dimethyl-4,4’-bipyridium chloride) is a highly toxic chemical herbicide primary used as a weed killer. It generates reactive oxygen species which cause cellular damage via lipid peroxidation, activation of nuclear factor-kappa B (NF-κB), mitochondrial damage and apoptosis in many organs. 2 Paraquat poisoning is proved to result in pulmonary damage and hepatotoxicity. 3 However, its role in causing cardiotoxicity remains ambiguous.
Case Summary (De-identified Subject)
An 18-year-old male was brought to tertiary care teaching hospital, in South India. The patient was transferred here from nearby local area hospital for further management. He was admitted with alleged history of consumption of an unknown compound. Several measures were taken despite which he had a cardiac arrest with bradycardia and succumbed to death in the next morning. The information from the police file revealed that the deceased was kidnapped and fed poison (a black bottle) at the railway station.
On Autopsy Examination
The body of a young male brought to the mortuary was cold and stiff (rigor mortis was present) all over the body. Postmortem lividity present over the back was not fixed. Multiple external injuries like abrasions and contusions were present over the chest, abdomen and upper limbs. The skull, vertebrae and spinal cord remained intact. The brain was oedematous. The tracheal lumen contained purulent mucoid fluid and both the lungs were soft, congested and blood-stained frothy fluid oozed on the cut section. Multiple epicardial haemorrhages were present over the anterior and posterior surface of the left ventricle of the heart. Walls were intact and valves were competent. All the coronaries were patent on cut section. The aortic wall showed multiple atheromatous streaks. The stomach, parts of the intestinal mucosa and adrenals were haemorrhagic. The liver, spleen and kidneys were congested on cut section.
The colour tests and thin layer chromatographic methods of analysis responded for the presence of paraquat (herbicide) in the blood. The histopathological examination of left ventricle wall showed neutrophilic infiltrate with focal myocardial necrosis suggestive of acute MI. Hence, the final opinion as to the cause of death from perusal of histopathology report, autopsy findings and Regional Forensic Science Laboratory (RFSL) report is due to acute MI as a complication associated with consumption of paraquat (herbicide).
The consent was obtained from the relatives of the deceased person to publish the article which adds to the existing literature.
Discussion
Paraquat poisoning is a major medical problem in Asia and few parts of the world. The inherent toxicity and lack of effective treatment are responsible for high-case fatality of poisoning by this herbicide. 2 With no specific antidotes for paraquat poisoning and increased use of paraquat for suicidal or homicidal purpose, mortality for the same is increasing at an alarming rate. Although it is a commonly used herbicide, cases of consumption of this chemical and a subsequent MI are rare. Thus, we intend to study and discover the cause of this rare consequence. If paraquat is ingested, the patient can be decontaminated by administering activated charcoal or fuller’s earth. Further symptomatic management includes oxygen therapy, intravenous fluids and electrolyte replacement. In severe cases, hemoperfusion or haemodialysis may be considered to remove paraquat from the bloodstream. Currently, to treat paraquat poisoning no specific antidote is available. 2 Thus, with no effective treatment for paraquat poisoning, understanding this case will help not only in the early diagnosis and prompt treatment of the cardiac complications of paraquat poisoning but also with the effect of this chemical on the body as a whole.
Paraquat can enter the body by both ingestion and inhalation. Direct skin contact for a long duration of time has also been reported to cause poisoning. Owing to its colourless and odourless properties, this potent toxin can be readily mixed with food or water prior to consumption. Consumption of excess paraquat can damage the kidney, liver, lungs, gastrointestinal tract, as well as the heart which is often severely injured and causes death at early stages. On histopathology, high concentrations of paraquat in the myocardium often present as haemorrhage and congestion. 4
On hospital admission, the patient had normal ECG findings and a mild tricuspid regurgitation on two-dimensional (2D) echocardiogram (ECHO). Within 24 hours, he persisted to have hypotension with repeated bouts of bradycardia, and despite therapeutic interventions he succumbed to death. The histopathology report of the heart of this patient revealed acute MI as a complication associated with the consumption of paraquat. Further, it was observed that multiple epicardial haemorrhages were present over the anterior and posterior surface of the left ventricle of the heart and the wall of the aorta showed multiple atheromatous streaks.
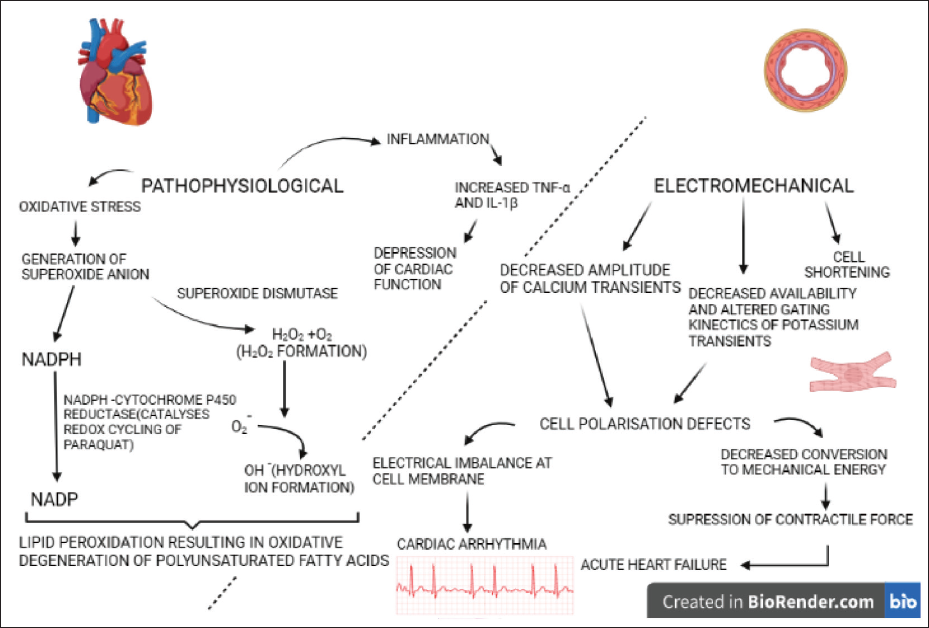
As depicted in Figure 1, at the cellular level paraquat toxicity causes generation of superoxide anion, in turn leading to the formation of more toxic reactive oxygen species, such as hydrogen peroxide and hydroxyl radical and the oxidation of the cellular nicotinamide adenine dinucleotide phosphate (NADPH), the major source of reducing equivalents for the intracellular reduction of paraquat, which results in the disruption of important NADPH requiring biochemical processes. 5
Paraquat causes oxidative stress by generating superoxide anions; these ions predominantly have three effects on the normal functioning of the heart and the body as a whole. First, it causes lipid peroxidation in a concentration-dependent manner when incubated with NADPH and NADPH cytochrome P450 reductase (catalyses redox cycling in paraquat) and thus altered lipid metabolism. Next, it forms hydrogen peroxide in the presence of the enzyme superoxide dismutase. Lastly, on reacting with the hydrogen peroxide formed, subsequent generation of hydroxyl free radical occurs. This leads to the destruction of nucleic acids, proteins and polysaccharides. 6
Paraquat poisoning induces tumour necrosis factor-alpha (TNF-α) and interleukin-1 (IL-1-β) production. These substances act as proinflammatory cytokines whose expression is mediated by the toll like receptor (TLR-4) consequently causing myocardial damage. 7
In a study associated with haemodynamic and electromechanical effects of paraquat in rat heart, paraquat decreased the amplitude of Ca2+ transients, reduced the availability, altered the gating kinetics of K+ transients and caused cell shortening in ventricular myocytes. This led to cell polarisation defects and subsequently electrical imbalance at cell membrane precipitating as cardiac arrythmias. Paraquat decreased heart rate, arterial blood pressure and cardiac contractility, as well as prolonged the PR, QRS, QT and QTc intervals in a dose-dependent manner leading to a suppression of left ventricular contractile force and thus acute heart failure. 8
Thus, the oxidative stress, proinflammatory cytokine production, TLR-4 expression and electrocardiographic changes culminate in myocardial dysfunction and severe heart damage.
Through our study we have generated a hypothesis on the effect of paraquat on the heart; however, it may not have sufficient statistical power to detect meaningful associations and it would be difficult to generalise the findings to a larger population. To overcome these limitations, our findings should be corroborated by more rigorous study designs such as randomised controlled trials or cohort studies.
Conclusion
Paraquat can enter the body by ingestion or inhalation. It generates superoxide anions leading to the formation of more toxic reactive oxygen species and the oxidation of NADPH. It increases the production TNF-α and IL-1β substances that act as proinflammatory cytokines consequently causing myocardial damage. It reduces the availability and decreases the amplitude of Ca2+ transients, alters the gating kinetics of K+ transients and causes cell shortening in ventricular myocytes. This can lead to cell polarisation defects and subsequently electrical imbalance at cell membrane precipitating as cardiac arrythmias. It decreases heart rate, arterial blood pressure and cardiac contractility, as well as prolongs the PR, QRS, QT, intervals in a dose-dependent manner leading to a suppression of left ventricular contractile force and thus acute heart failure. The oxidative stress, proinflammatory cytokine production, TLR-4 expression and electrocardiographic changes culminate in myocardial dysfunction and severe heart damage. Hence, it is important for clinicians to continuously monitor the heart and for forensic pathologists to keep this inference in mind while ascertaining the cause of death.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval and informed consent have been obtained for the study.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.