
Abstract
Background
In Turkey, dementia care is largely provided by family members due to limited formal services and strong cultural expectations regarding familial responsibility. This situation places caregivers under considerable burden and exposes them to complex ethical dilemmas, particularly when balancing patient autonomy and safety.
Research aim
This study aimed to explore the ethical challenges and dilemmas faced by family caregivers providing dementia care in Turkey.
Research design
A descriptive qualitative design using interpretative phenomenological analysis (IPA) was employed to explore caregivers’ lived experiences. Data were collected through semi-structured interviews (June–July 2024), audio-recorded, and transcribed verbatim. Methodological rigor was ensured using COREQ guidelines.
Participants
Participants comprised 12 family caregivers of individuals with dementia receiving home-based care coordinated by a state hospital in Turkey. Purposive sampling was used. Eligible participants were Turkish-speaking adults who had provided unpaid care for at least 6 months.
Ethical considerations
Ethical approval was obtained from the Koç University Social Sciences Ethics Committee (Approval No: 2024.022.IRB3.005). Written informed consent was obtained, confidentiality was ensured using pseudonyms, and participants could withdraw at any time without consequences.
Findings
Three themes emerged: dissatisfaction with formal dementia care services; caregiving shaped by cultural values, moral responsibility, and emotional burden; and ethical dilemmas related to dignity, autonomy, informed consent, daily care practices, and medical decision-making. Caregivers frequently described tensions between protecting their relatives and respecting autonomy, often in the absence of professional ethical guidance.
Discussion and conclusions
The findings highlight how ethical dilemmas in dementia care are not solely individual but are shaped by cultural norms and systemic limitations. The lack of accessible formal services and ethical support structures intensifies caregivers’ moral distress and decision-making burden. Culturally sensitive, ethically informed, and family-centred support systems are essential to strengthen caregivers’ decision-making and well-being.
Introduction
Dementia is a progressive neurodegenerative condition characterized by cognitive deterioration and functional impairment, eventually leading to dependency.1,2 While early diagnosis can delay function loss, disease progression inevitably increases the care burden. 3 Globally, dementia prevalence is rising dramatically, projected to increase from 57.4 million in 2019 to 152.8 million by 2050.4,5 A similar trend exists in Turkey, driven by a rapidly aging population and increasing life expectancy.6,7
Family caregivers play a central role in supporting people with dementia, often assuming responsibility for complex and long-term care. In the context of dementia care, ethical dilemmas often arise when caregivers must choose between competing moral values, such as respecting the autonomy of the person with dementia and ensuring their safety or well-being. These situations frequently involve tensions between ethical principles, including autonomy, beneficence, non-maleficence, and respect for dignity. 8
The existing literature in Turkey largely focuses on quantitative measures of caregiver burden, offering limited insight into caregivers’ ethical decision-making processes and lived experiences.9–11 This study aims to bridge this gap by exploring the ethical dilemmas and care challenges faced by family caregivers of people with dementia in Turkey, contributing to a more context-sensitive understanding of family caregiving.
Background
In Turkey, care for people with dementia is provided primarily within the family, as state-supported services and professional support remain limited and trust in institutional care is generally low.9,12–14 Although certain services, such as home healthcare visits, primary care follow-up, and social assistance programs, are provided by the state, family caregivers continue to assume responsibility for most aspects of dementia care, including daily personal care, management of symptoms, and supervision. Family caregivers of PwD perceive their caregiving role in diverse ways, reflecting both positive and negative aspects of the caregiving experience. While some describe caregiving as a source of personal growth and maturity, the majority emphasize the significant physical and emotional difficulties it entails.9,10
In low- and middle-income countries, most dementia care costs are attributable to informal care (65%). 15 In Turkey, dementia care is largely organized around family-based support, reflecting both structural limitations in long-term care services and strong cultural expectations regarding familial responsibility. Although certain formal services exist, including home healthcare visits coordinated by public hospitals, follow-up by family physicians, and social assistance allowances for dependent individuals, these services remain limited in scope and continuity. As a result, family members assume responsibility for most aspects of dementia care, including supervision, personal hygiene, medication management, and emotional support. Consequently, informal caregiving is the dominant form of dementia care in Turkey, while formal services primarily serve as supplementary support rather than as primary providers of care. 16
These challenges are further intensified by the limited scope, fragmentation, and implementation gaps in national dementia care policies and models. Although a national dementia care model has been proposed, existing services remain limited, unevenly distributed, and insufficiently coordinated, placing a substantial burden on families and informal caregivers. 17 In the cultural context, institutional care is often perceived as “abandoning” or “leaving a relative on the street,” reflecting a culturally embedded stigma and sense of filial obligation. Which introduces a unique ethical complexity and intensifies caregivers’ sense of moral responsibility and emotional burden. As reported by Kucukguclu et al., 18 family members often delayed decisions about institutional care despite recognizing the need for professional support, due to social pressure and internal conflict. This situation leads caregivers to face both extensive difficulties and challenging ethical dilemmas in accessing formal and informal healthcare services for their loved ones. International studies indicate that these dilemmas commonly revolve around balancing individuals’ desire to remain at home with the need to ensure safety, frequently placing caregivers between respecting autonomy and preventing harm.8,19 In advanced dementia, ethical challenges are further intensified when practices such as restricting nutrition and fluid intake conflict with the wishes of people with dementia and may lead to harmful outcomes. 20 Overall, family caregivers often struggle to balance safety and autonomy, which may result in involuntary treatment and underscores the growing need for professional support. 21
In Turkey, these challenges may be further compounded by cultural coping mechanisms, including reliance on religious beliefs and fatalistic attitudes. 9 The limited availability of day care centres and similar support services means that family caregivers are largely left to manage these ethical and practical challenges on their own, which negatively affects the quality of life of people with dementia and increases the socio-economic burden on families and the state. 14 Moreover, caregiving burden in Turkey is exacerbated by sociodemographic factors, as caregivers are most often female, unemployed, or have lower levels of education, contributing to emotional distress, financial strain, and social isolation. 12 Understanding ethical dilemmas in dementia care is essential not only for supporting caregivers but also for informing healthcare policy and practice, as these dilemmas reflect broader systemic challenges related to care provision, ethical guidance, and the allocation of resources. 22
Methods
Study design
A descriptive, qualitative design using Interpretative Phenomenological Analysis (IPA) was employed to explore the challenges and ethical dilemmas faced by family caregivers of people with dementia. IPA was selected for its capacity to examine complex, emotionally laden, and ethically sensitive lived experiences, 23 addressing the limited context-specific research in Turkey. Data were collected between June and July 2024. The COREQ checklist was used to guide the reporting of the study design, participant recruitment, data collection, and analysis processes to ensure transparency and methodological rigor. (Appendix I). The study was conducted as initial part of the cross-country study.
Participants and setting
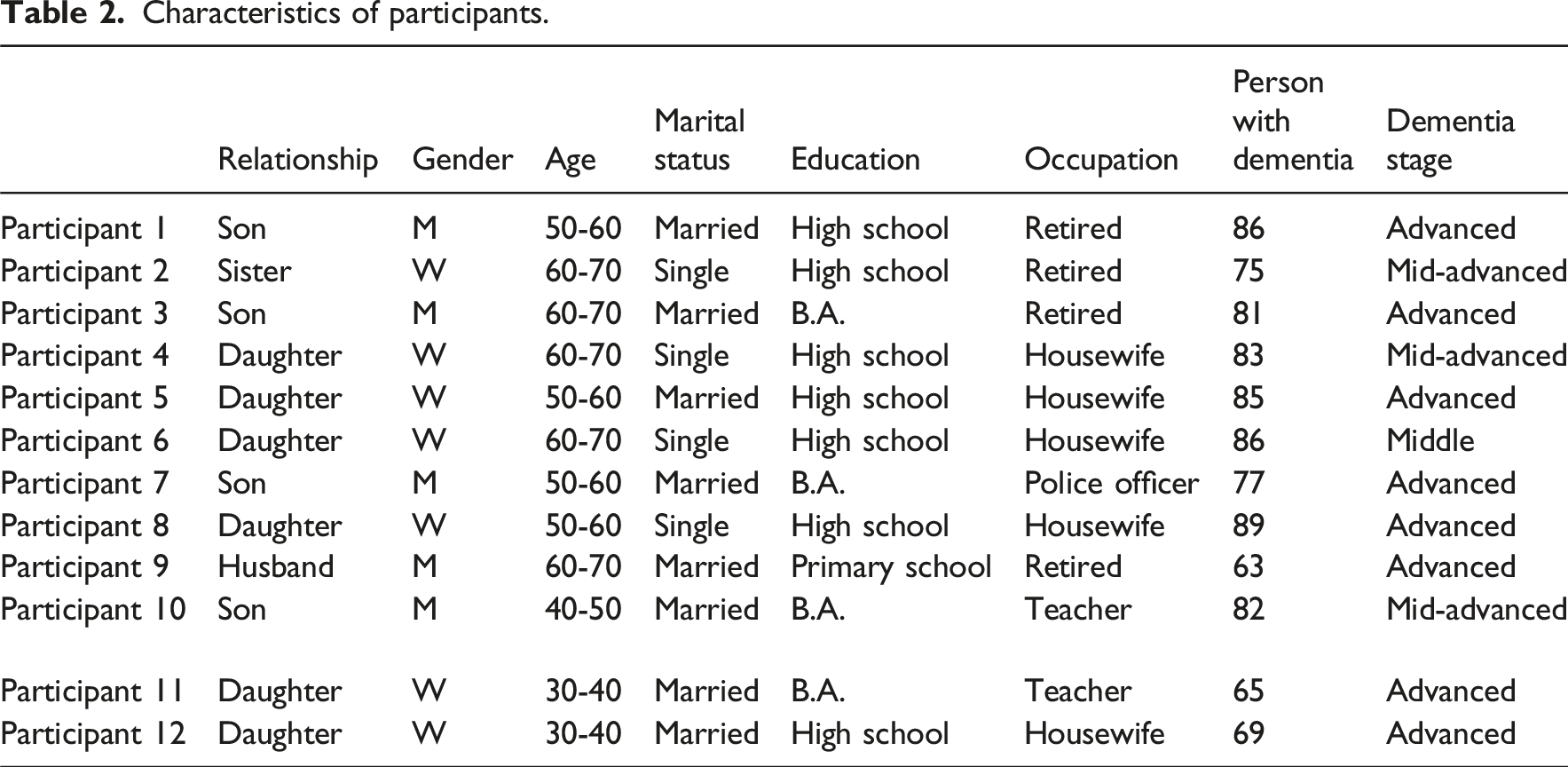
The study sample consisted of 12 family caregivers (six daughters, four sons, one husband, and one sister) of people with dementia who were receiving home-based healthcare services coordinated by a state hospital. These services were provided in the individuals’ homes and supervised by the hospital’s home healthcare unit. To be eligible for inclusion, participants were required to speak Turkish and to have provided unpaid, informal dementia care to their family member for at least six months. Participants were recruited using purposive sampling based on predefined inclusion criteria.
Data collection continued until data saturation was achieved, with no new themes or significant insights emerging from the interviews. Potential participants were identified through the hospital’s home healthcare unit and were approached by healthcare staff who informed them about the study. Caregivers who expressed interest were then contacted by the researcher and provided with detailed information before being informed of the study’s purpose and procedures.
Data collection
Data were collected via semi-structured, in-depth interviews between June and July 2024, following Kallio et al. 24 A literature-based interview guide (Appendix II) was used to explore ethical dilemmas and care challenges. The first author conducted face-to-face interviews in Turkish at participants’ preferred locations. Interviews averaged 60 min (range: 47–72) and were audio-recorded and transcribed verbatim with informed consent.
The interviews were conducted by the first author, a nursing researcher with professional experience in dementia care and training in qualitative research methods. The researcher also had prior familiarity with dementia care through clinical and academic work, which facilitated rapport with participants while maintaining reflexive awareness throughout the interview process. To minimize potential bias, the researcher followed the semi-structured interview guide and encouraged participants to freely express their experiences and perspectives. To enhance rigor, interview recordings were transcribed verbatim and checked for accuracy by a second author. Regular team meetings were held to discuss emerging insights and ensure consistency in data collection and interpretation.
The interview guide included a range of contextual and background questions to support a comprehensive understanding of the caregiving situation and to facilitate in-depth exploration during interviews. Although not all collected data were directly presented in the results, these data informed the analytical process and helped contextualize participants’ experiences in relation to ethical challenges and dilemmas.
As some participants were unfamiliar with the concept of an “ethical dilemma,” a brief, neutral explanation was provided at the beginning of the interview. To minimize potential interviewer influence, the explanation was kept general and non-directive, and participants were encouraged to describe their experiences in their own words. The researcher avoided leading questions, used open-ended prompts, and maintained reflexive awareness throughout the data collection process.
Data analysis
Example of the IPA analysis process.

Rigor and trustworthiness
To ensure rigor and trustworthiness, the study followed the criteria proposed by Lincoln and Guba, 25 including credibility, transferability, dependability, and confirmability. Credibility was enhanced through prolonged engagement with the data, repeated reading of transcripts, and the use of verbatim quotations to accurately reflect participants’ experiences. Transferability was supported by providing detailed contextual descriptions of the study setting and participants. Dependability and confirmability were ensured through maintaining an audit trail of analytical decisions, researcher reflexivity during data interpretation, and collaborative discussions among the research team during coding and theme development.
Ethical considerations
Ethical approval was obtained from the Koç University Social Sciences Ethics Committee (Approval No: 2024.022.IRB3.005, dated January 25, 2024). All participants provided written informed consent prior to participation, and confidentiality was maintained through the use of pseudonyms. Participants had the right to withdraw at any stage without consequences.
Potential emotional risks were considered prior to data collection, particularly the possibility that participants might reflect on their caregiving practices and experience distress or self-criticism. To mitigate this, interviews were conducted in a supportive and non-judgmental manner, participants were reassured that there were no right or wrong answers, and they were informed of their right to pause or withdraw at any stage without any consequences.
During the interviews, some participants described situations that could be interpreted as potentially inadequate or ethically challenging care practices. In such cases, the researcher maintained a non-judgmental stance during data collection to avoid influencing participants’ responses. However, participants were treated with sensitivity, and where appropriate, general information about available healthcare support services was provided. No immediate risk requiring formal reporting was identified during the study.
Results
Characteristics of participants.
Theme 1: Family caregivers’ perceptions regarding formal dementia care
This theme reflects caregivers’ overall appraisal of the formal care system, highlighting how unmet needs, limited professional involvement, and structural barriers contribute to dissatisfaction and mistrust toward care services. At the same time, caregivers’ narratives reveal strong expectations for more responsive, coordinated, and person-centred support. This theme includes three major categories: dissatisfaction with care services and providers, health system–related challenges, and expectations from care services. This theme reflects not only caregivers’ dissatisfaction with formal services but also the ethical tensions arising from inadequate care, lack of support, and perceived neglect within the healthcare system.
Category 1a. Dissatisfaction with formal care services and providers
Caregivers reported dissatisfaction with the limited scope of formal services and minimal medical involvement, leading to significant mistrust. This was particularly pronounced among those with negative experiences in hospitals or nursing homes. Caregivers often felt that hospitalization worsened their relative’s condition rather than improving it. For instance, one participant noted, “She was hospitalized for 10–1 days... It is a different world before and after the hospital” (Participant 7).
Another major source of dissatisfaction was the lack of proactive medical follow-up. Caregivers felt that doctors rarely investigated the individual's status or drug efficacy, assuming “there is no cure.” Financial inadequacy was also highlighted; rising costs and insufficient state support made it difficult to afford basic supplies like diapers. “Financial support is insufficient; only money for diapers is provided. I wish diapers were given free of charge” (Participant 1).
Category 1b. Health system–related challenges
Participants identified insufficient governmental support and bureaucratic hurdles as key systemic challenges. The financial burden of essential supplies was a primary concern, with one caregiver stating, “My biggest problem will be after the New Year. I am retiring” (Participant 7), fearing future income insecurity.
Bureaucratic procedures, such as frequent renewal of health reports for disability benefits, were described as repetitive and unnecessary. Caregivers questioned why reports were required every few months when the disease is progressive and permanent. “Now, a health report is required every three months... You know, it is already communicated in cases of death” (Participant 3).
Additionally, the lack of accessible transportation for hospital visits created a severe physical burden. Ambulance services were often delayed or provided only one-way transport, leaving families to struggle with immobile individuals on stairs. “We wait for 2-3 h for the ambulance to return... Even if they bring her, they do not take her upstairs” (Participant 11).
Category 1c. Family caregivers’ expectations concerning care services
Participants identified a critical need for accurate information on disease progression and management, noting that standard home care services were often insufficient. Consequently, they expected continuous follow-up by specialized healthcare teams rather than generalist providers. “A special healthcare team should be established for these individuals rather than ‘regular’ home care services” (Participant 1). “I think doctors should come and see the individuals at home... Because after the disease progresses... No one can go to the doctor” (Participant 12).
Caregivers also emphasized the necessity of social engagement and psychological support to combat isolation and restore a sense of normalcy. “People like us, who stay at home and become socially withdrawn, should receive psychological support. At first, I might say that nothing is wrong with me, even though I feel overwhelmed” (Participant 2).
Finally, participants expressed a strong need for respite support temporary caregivers to assume responsibilities during daily errands though some remained skeptical about the state’s capacity to provide this. “I wish there was someone or somewhere to entrust. These are beyond impossible. How can the state afford it?” (Participant 4).
Theme 2: Participants’ views on caregiving
Participants’ reflections reveal that caregiving is a complex, relational, and value-driven role shaped by personal attributes, emotional capacity, and moral commitment. Beyond practical tasks, caregiving is sustained by resilience, love, and deeply held values such as patience and obligation. Narratives highlighted everyday practices that often involved ethical reflection on doing what was perceived as ‘right’ under difficult circumstances. This theme comprises four categories: personal attributes, care with love and shared responsibility, motivational resources, and the impact on caregivers’ lives.
This theme highlights how caregiving is shaped by moral responsibility, emotional commitment, and ethical tensions related to doing what is perceived as ‘right’ under challenging circumstances.
Category 2a. Personal attributes shaping the caregiving role
Participants emphasized that traits such as patience, compassion, and conscientiousness were essential for sustainable care. Caregivers noted that a lack of these attributes could negatively impact the individual. “The basis of this is patience, patience, patience” (Participant 1). “I have conscience and compassion. I can’t say no if someone needs me” (Participant 2). “If he [another caregiver] complains while changing diapers... This affects the people with demantia. So you have to be patient” (Participant 10).
However, the capacity to care was also strained by conflicting commitments. Participant 12 highlighted the difficulty of balancing care with personal family duties: “You want to take care of everything... but you have your own family... It is very heavy.”
Additionally, caregivers with professional medical experience or networks reported a distinct advantage in managing clinical tasks (e.g., medication, wound care) and navigating the health system. “While I follow this process myself as someone who retired from the hospital, it is very difficult for those who do not know anything” (Participant 1). Others noted that personal connections with hospital staff facilitated access to home services. Finally, adopting a mindset of acceptance and responsibility was deemed crucial for preventing complications and maintaining resilience.
Category 2b. Providing care with love and sharing responsibilities with others
Participants identified caregiving as a priority rooted in love, gratitude, and filial obligation. As one son noted, “She is the first to be taken care of” (Participant 1). Another added, “She is a person who has fed and raised us” (Participant 10).
Sharing responsibilities was a common strategy to ease the burden, though the extent of support varied. While some distributed tasks effectively, others faced isolation when family members withdrew. “My father withdrew... I took care of my mother alone while I was pregnant” (Participant 11). Furthermore, the attitude of auxiliary caregivers was crucial; participants noted that if a family member approached care with frustration or disgust, it caused fear and distress for people with demantia (Participant 10).
Often, shared responsibility was a physical necessity rather than a preference. Tasks such as bathing required multiple people: “It's very difficult to wash her... Not by myself, but my sister or someone else comes” (Participant 8). Additionally, caregivers assumed quasi-professional roles, meticulously monitoring nutrition and medical values to ensure the individual's well-being (Participant 3).
Category 2c. Motivational and supportive resources for caregiving
Family caregivers stated that their care for a loved one was motivated primarily by love and faith. They emphasized that being spiritually faithful was also an important motivating factor in sustaining the caregiving role.
Our faith comes into play. If there is no faith, no one can handle it (Participant 1).
My faith. This disease is a test for the whole family. When you think like this, believe me, it does not hurt, it gives you more strength (Participant 7).
Category 2 d. Impact of caregiving on caregivers’ health and lives
Participants reported that the physical and emotional demands of caregiving exacerbated their own severe health conditions. Some managed care duties while undergoing treatment for life-threatening illnesses. “I had two major surgeries and... Was receiving chemotherapy for stomach cancer” (Participant 9). “I had a heart attack. I have a clot in my brain right now... Of course, there are tranquilizers in it” (Participant 2). Others described persistent fatigue, such as while providing care after hip surgery and while walking with canes (Participant 6).
Caregiving also restricted personal lives; some caregivers remained single or separated due to their responsibilities. Those caring for multiple family members described an inability to spare time for themselves, struggling to coordinate conflicting medication and hygiene schedules (Participant 3).
Furthermore, safety concerns such as wandering and falls were major sources of tension. The constant vigilance required for fall prevention led to significant emotional strain. One caregiver revealed the desperate perspective that immobility could be safer than mobility: “Last time her leg was broken because she fell. So actually, we say it is better for us that my mother is in bed” (Participant 5). Others described falls as a repetitive and sometimes inevitable challenge despite their best efforts (Participants 8, 9). This finding reflects a fundamental ethical tension between ensuring safety and preserving the autonomy of the person with dementia, highlighting the complexity of decision-making in everyday caregiving practices.
Theme 3: Ethical issues and dilemmas
This theme captures ethical challenges where caregivers navigate tensions between care responsibilities, respect for the person, and systemic limitations. Ethical concerns emerged in interactions with formal services, daily care practices, and complex decision-making. Caregivers often struggled to balance their loved ones’ safety and wishes with their own capacities. This theme comprises three categories: ethical issues in formal care, dignity in daily care, and decision-making dilemmas.
Category 3a. Ethical issues related to formal care
Caregivers reported dilemmas stemming from providers treating care as routine, task-oriented work rather than human interaction. Issues included inadequate follow-up, privacy violations, and “bureaucratic” approaches to care. “Unfortunately, it is more like work than care... I can say it is like work, without hesitation” (Participant 1).
A significant source of distress was insufficient or misleading information regarding disease progression. Participant 12 described a doctor dismissing her anxiety about her mother’s breathing as merely “part of the process.” Similarly, Participant 9 highlighted the ethical impact of contradictory prognoses: “(The doctor said) 'We will progress one stage in 5 years.'... After a year, I noticed something was wrong... When we went back, he said... sometimes all seven stages can occur within a single year.”
Systemic rigidities also caused ethical friction. Some families were denied financial support due to technicalities, despite evident need. “They did not approve the care allowance because the physical environment... Was inadequate. Since we take care of my mother alternately... She does not stay in a fixed place” (Participant 10).
Category 3b. Ethical concerns in daily life and dilemmas
Ethical concerns arose when caregivers or family members ignored the agency of the person with dementia, treating them as invisible during conversations about their own care. “You ask too often what she wants to eat. We do not ask; we just give her whatever we cook” (Participant 10). In more severe instances, caregiver stress manifested as harsh verbal or behavioral treatment, raising serious ethical concerns about dignity. “Shut up. Shut up. You made me angry again... I will tie you up” (Participant 8). Decisions regarding medical interventions were often characterized by uncertainty and a lack of clear guidance. Caregivers struggled to balance prolonging life with minimizing suffering/disability. Participant 7 described the agonizing choice between risky surgery and a bedridden life: “My biggest dilemma there was the lack of information... If I have it done, there is death, disability. If I don’t, she will be bedridden... At least... My mother is alive.”
Others wrestled with the trade-off between medication side effects and disease control, questioning if treatment was compromising the individual’s essence. “I wonder if my mother has... dementia, since these drugs... made her completely robotic. Should she not use them? But even if she doesn't, I see that she will get worse” (Participant 12).
Discussion
This study explored the experiences and perspectives of family caregivers providing caring for people with dementia in Turkey, highlighting three major themes: (1) family caregivers’ perceptions regarding formal dementia care, (2) participants views on caregiving, and (3) ethical issues and dilemmas.
Regarding formal care, caregivers consistently reported dissatisfaction with the quality, accessibility, and individualisation of services. Despite these shortcomings, expectations for more comprehensive, empathetic, and specialized dementia care persisted. Caregivers frequently described formal services of dementia care as inadequate and reported declining trust in the healthcare system, which often led them to prefer home care. Financial strain and the lack of established home care services emerged as major concerns, with many caregivers reporting that current allowances were insufficient to meet essential home care needs. Beyond these structural limitations, the findings also reveal important ethical tensions related to justice, access to care, and the unequal distribution of responsibility between families and the healthcare system. In this context, inadequate formal support may place a disproportionate moral burden on family caregivers, raising ethical concerns about equity and responsibility in dementia care.
Previous studies confirm these findings, although the reasons for dissatisfaction vary. For example, Dombestein et al. 26 reported that adult child caregivers experienced challenges when their own needs were assessed independently of their parents’ care needs, resulting in fragmented support and insufficient consideration of the caregiving context. Frequent changes in professionals visiting the home, referring to the lack of continuity and the involvement of multiple, frequently changing care personnel, created feelings of insecurity among caregivers. Caregivers in the present study similarly emphasized the need for specialized dementia care teams, regular physician follow-up, and home visits. In the Turkish context, such specialized and coordinated dementia care services remain limited, and caregivers’ narratives reflected expectations rather than experiences of structured dementia-specific teams. These findings are consistent with international literature, which emphasizes respect for caregivers, inclusion in decision-making, and the provision of timely, professional information and guidance. 26
In Theme 2, informal caregiving was strongly influenced by caregivers’ personal characteristics, cultural values, and motivations. Patience, empathy, knowledge, and experience were reported as critical qualities for effective care. Consistent with previous research, caregiving in Turkey is predominantly family-based due to strong cultural expectations that frame caring for dependent family members as a moral and familial responsibility. 9 Qualitative evidence further suggests that institutional care is often perceived as morally problematic and associated with feelings of guilt and social pressure among families.18,27 In the present study, participants explicitly described placing family members in nursing homes as morally unacceptable, frequently equating institutionalization with abandonment or “leaving their relatives on the streets”. Caregivers frequently expressed guilt when prioritizing their own needs, and uncertainty about disease progression heightened distress. 13
At the same time, caregiving was also described as an act of love, responsibility, and gratitude, which fostered family solidarity and personal growth. Literature confirms this duality, noting that caregiving can result in both burden and positive transformation.9,10 However, findings from the present study suggest that caregivers did not experience this duality as a balanced or coherently or consistently integrated process; rather, love, responsibility, and moral obligation coexisted with guilt, self-neglect, and emotional distress, and were experienced as ongoing moral and emotional tensions. Motivational sources such as love, kinship ties, and moral values and faith-based beliefs played an important role; however, these were expressed primarily as generalized moral duties and acceptance rather than as references to specific religious doctrines.28,29 While religious beliefs were described as an important source of coping and meaning for caregivers, they may also have more complex implications. In some cases, interpreting caregiving challenges as a “test” or part of a divine plan may discourage or delay seeking professional support, thereby reinforcing reliance on family-based care.
Theme 3 integrates caregivers’ accounts of care-related burdens with the ethical issues and dilemmas embedded in dementia caregiving. The continuity, intensity, and complexity of dementia care placed significant demands on both caregivers and the healthcare system. Participants described structural and bureaucratic difficulties such as scheduling appointments, accessing diagnostic tests, and securing emergency care. Transporting the individuals with advanced dementia also emerged as a significant burden. These challenges reflect systemic and geographical inequalities in access to long-term care, consistent with Penneau and Or. 30
The long-term nature of caregiving negatively affected caregivers’ physical, psychological, and social well-being. Health problems, sleep disturbances, depression, and social isolation were commonly reported, with women disproportionately affected. This finding aligns with research by Adana et al. 12 and Sajwani, 31 who noted that caregiving responsibilities often lead to sleep problems, restricted social lives, and concerns about sexuality. Supporting caregivers through training, psychosocial interventions, and targeted policies is therefore crucial.10,11 However, in the Turkish context, the feasibility of such interventions is shaped by structural limitations and prevailing social stigma surrounding dementia. Caregivers’ narratives suggest that stigma, shame, and fears of social judgment may hinder help-seeking behaviors and limit engagement with formal psychosocial support services. Therefore, caregiver support initiatives in Turkey may be more effective when integrated into existing home care services, delivered in family-centred formats, and designed to reduce stigma by normalizing dementia as a medical condition rather than a source of social shame.
Within this theme, ethical challenges in dementia care are not confined to isolated incidents but are deeply embedded in both formal and informal caregiving contexts. Rather than reflecting individual shortcomings, these ethical tensions point to structural, relational, and cultural dimensions of care that shape how decisions are made and experienced by both caregivers and people with dementia. In formal care settings, ethical concerns related to routine and impersonal care practices, insufficient communication, limited access to information, and difficulties in accessing financial support raise broader questions regarding dignity, justice, and trust within healthcare systems. Similar ethical vulnerabilities have been reported in previous studies on dementia care, particularly those demonstrating that inadequate communication and lack of ethical guidance can undermine care quality and increase distress among families.21,32 Although conducted in different healthcare contexts, these studies illustrate ethical challenges that are widely recognized across dementia care settings, supporting the relevance of the present findings beyond national boundaries.
Ethical tensions were also evident in home care contexts, where issues related to the individual privacy, inappropriate communication styles, and controlling caregiving behaviors underscored the moral vulnerability of people with dementia and the emotional strain placed on family caregivers. These findings suggest that, in the absence of formal ethical support, caregivers are often required to rely on personal judgment when navigating complex moral situations, increasing the risk of moral distress and ethical uncertainty.
A distinctive contribution of the present study lies in illustrating how ethical dilemmas are intensified within the Turkish context, where strong familial responsibility, social stigma surrounding dementia, and limited access to structured support intersect. Decision-making dilemmas particularly those concerning medical interventions, disclosure of diagnosis, and end-of-life care were frequently shaped by moral uncertainty, emotional pressure, and cultural expectations rather than by structured ethical frameworks. While previous research highlights the importance of clear communication, transparency, and shared decision-making in addressing ethical dilemmas in dementia care,8,19,21,32 caregivers in this study often described managing these dilemmas largely on their own.
Coping strategies such as fatalism, acceptance, or faith-based interpretations previously described in the literature as ways of managing uncertainty in dementia care.8,9 emerged in this study as culturally situated responses to both emotional burden and limited systemic support. Rather than serving solely as individual coping mechanisms, these strategies appeared to function as moral frameworks through which caregivers made sense of ethically challenging situations.
Although some themes initially appear to reflect practical caregiving experiences, they also reveal underlying ethical tensions related to responsibility, autonomy, dignity, and justice. Some reported practices, such as restricting mobility to prevent falls or expressing frustration during care, may raise ethical concerns regarding dignity and autonomy. These findings highlight the complexity of caregiving under resource constraints and should be interpreted within the broader context of limited formal support and caregiver burden, rather than as intentional neglect.
An additional ethical consideration concerns the researcher’s responsibility when encountering potentially inadequate or neglectful care practices during interviews. Although no cases requiring formal reporting were identified in this study, such situations raise important ethical questions regarding the balance between maintaining participant confidentiality and ensuring the safety and well-being of vulnerable individuals. Researchers conducting studies in sensitive care contexts should remain aware of these responsibilities and be prepared to act in accordance with ethical guidelines if serious risks are identified.
Taken together, the findings suggest that ethical issues and dilemmas in dementia care should be understood as systemic and relational phenomena, shaped by healthcare structures, cultural norms, and caregiving relationships. Addressing these challenges requires not only individual-level support but also ethically informed, culturally sensitive, and context-specific care models that strengthen communication, guidance, and shared decision-making for family caregivers and people with dementia.
The findings of this study have important implications for nursing practice both in Turkey and internationally. First, the ethical dilemmas experienced by healthcare professionals highlight the need for structured ethical guidance and decision-support tools in dementia care, particularly in community settings. Nurses, who often serve as the primary point of contact for patients and families, are uniquely positioned to facilitate shared decision-making, advocate for patient autonomy, and support caregivers navigating complex care transitions such as institutionalization.
In the Turkish context, where dementia care is largely family-centered, nurses play a critical role in providing education, emotional support, and care coordination for family caregivers, who frequently assume extensive responsibilities with limited formal support. Strengthening community-based nursing services, including home care and follow-up systems, may help alleviate caregiver burden and improve continuity of care.
Beyond Turkey, these findings underscore the importance of culturally sensitive, person-centered approaches in dementia care, as ethical dilemmas are often shaped by sociocultural values and healthcare system structures. Integrating ethics education, communication training, and interdisciplinary collaboration into nursing practice and curricula may enhance nurses’ capacity to manage such dilemmas effectively across diverse care settings. For example, incorporating brief ethical consultations or decision-support approaches into routine home visits by healthcare professionals could reduce the ethical burden on caregivers, enhance confidence in decision-making, and improve the overall quality of care. Overall, these findings underscore the importance of addressing ethical dilemmas in dementia care to support both caregivers and care recipients.
Limitations
This study has several limitations. First, dementia caregiving in Turkey is a socially sensitive and ethically complex issue, often associated with stigma and moral burden. Some potential participants were reluctant to share their experiences or to be audio-recorded, which may have limited the diversity of perspectives. Although several caregivers initially hesitated to participate, they agreed after receiving further explanation of the study. Second, participants were not initially familiar with the term ethical dilemma and were able to reflect on ethical challenges only after the concept was explained by the researcher. This explanation may have influenced how some participants articulated their experiences.
Third, the inclusion criteria and time constraints of caregiving limited recruitment, resulting in a relatively small sample size. As with qualitative research, these factors may limit the generalisability of the findings. Finally, the study focused solely on family caregivers’ perspectives; the views of formal caregivers and people living with dementia were not included, which may restrict the scope of applicability of the results. The type of dementia diagnosis was not systematically collected, which may limit the interpretation of symptom variability across participants.
Conclusion
This study highlights the ethical challenges faced by family caregivers providing dementia care in Turkey and underscores the interdependent nature of formal and informal care. The findings emphasize the need to support caregivers through professional guidance, ethical counseling, and psychosocial interventions to improve care quality. Policymakers should use these insights to strengthen dementia-specific services and develop ethically informed, person-centred care models. The results also offer direction for future research on culturally sensitive and sustainable dementia care in Turkey.
Supplemental material
Supplemental material - Family caregivers’ perspectives on ethical challenges in dementia care
Supplemental material for Family caregivers’ perspectives on ethical challenges in dementia care by Nadiye Bariş Eren, Seda Güney, Daniel Sperling in Nursing Ethics
Supplemental material
Supplemental material - Family caregivers’ perspectives on ethical challenges in dementia care
Supplemental material for Family caregivers’ perspectives on ethical challenges in dementia care by Nadiye Bariş Eren, Seda Güney, Daniel Sperling in Nursing Ethics
Footnotes
Acknowledgements
The authors thank the participants who participated in this study for their valuable time, insights, and contributions, and to the COST Action CA21137 (EDEM) support and their collaboration.
Ethical considerations
Ethical approval was obtained from the Koç University Social Sciences Ethics Committee (Approval No: 2024.022.IRB3.005).
Consent to participate
Written informed consent was obtained from all participants prior to participation.
Consent for publication
Written informed consent for publication of anonymized data was obtained from all participants.
Author contributions
N.B.E. contributed to data collection and analysis, manuscript writing. S.G. contributed to study design, analysis, and manuscript writing. D.S. contributed to conceptual development and critical revision of the manuscript. All authors approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to confidentiality agreements but are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.