
Abstract
Background:
Non-pharmacological interventions show promising positive effects on dementia symptoms. Since the majority of dementia care activities are performed by family caregivers, it is important to know how they perceive and implement such approaches. We aimed to investigate the extent to which non-pharmacological interventions are considered by family caregivers in dementia care and the barriers they encounter in implementing them.
Methods:
A total of 30 family caregivers (mean age: 63.07 years, female: 70%) living inside (30%) and outside the homes (70%) of people with dementia participated. Descriptive data analysis was used to determine the frequency of non-pharmacological interventions implemented, perceived effects, lacking resources, and barriers, while inferential statistics were used to examine whether funding source varied between interventions with high versus low frequency.
Results:
The most frequently implemented non-pharmacological interventions were initiating/maintaining social contact, cognitively stimulating and rehabilitative activities, and time in nature. In general, enjoyment was the most commonly perceived effect of non-pharmacological interventions. Additional effects were reported with respect to well-being, cognitive decline, autobiographical memory, perception of competence, and other symptoms. Major barriers were organizational burden, accessibility, and a lack of funding. Further, lacking resources included a lack of services (e.g., therapies, transport, group activities) and information on possible interventions.
Discussion:
This study highlighted that family caregivers frequently implement non-pharmacological interventions in dementia care. Given the perceived positive effects on dementia symptoms, health care interventions are needed that address barriers and provide resources to foster the implementation of non-pharmacological interventions by family caregivers.
Keywords
Introduction
Dementias are not only a challenge for those affected and their family environment, it is also a major public health concern.1,2 The primary cause of this concern is the memory loss; however, the person’s thinking, behavior, and ability to perform activities of daily living also deteriorate, 3 resulting in a high financial, emotional, and social burden. 4 About 55 million people worldwide live with dementia and this situation will continue to worsen in the coming years since demographic changes such as decreasing birth rates, paired with increasing life expectancy, 5 result in a substantial increase in the number of people with dementia. 6 In light of this, identifying effective prevention strategies as well as measures to mitigate the progression of dementia has been highlighted as key elements in the public response to dementia. 1 Pharmacological treatments currently have a limited effect on the progression of the underlying disease. 7 Thus, non-pharmacological interventions have moved into the foreground with promising implications for dementia prevention and treatment.8-10
Studies have shown that non-pharmacological interventions can have positive effects for people with dementia by improving and maintaining cognitive performance, improving emotional well-being, maintaining functional daily living skills, and alleviating behavioral symptoms. 11 Among the measures that can be used to accomplish this are cognitive stimulation, 12 cognitive training, 13 occupational therapy, 14 reminiscence therapy, 15 aromatherapy, 16 and music therapy. 17 This established evidence of non-pharmacological interventions in dementia are well-recognized, so that the guidelines of the World Health Organization, 18 and the “German S3 guidelines on dementia,” 19 an evidence-based action framework for people with dementia in Germany, provide corresponding recommendations for the implementation of non-pharmacological interventions in dementia care. However, the extent to which non-pharmacological interventions are currently being considered in the treatment and care of people with dementia in Germany is unknown.
People with dementia generally require high levels of care, most of which is provided by family caregivers. 20 Most caregiving activities involve personal care,20,21 although non-pharmacological interventions aim to improve the situation for people with dementia and their environment.21,22 A systematic review indicated a general lack of funding for non-pharmacological interventions, 23 suggesting they are less likely to be due to the higher financial burden. A study investigating 3 different non-pharmacological interventions, including chair yoga, music intervention, and chair-based exercise, demonstrated how family caregivers reported noticeable changes in cognitive symptoms, physical function, mood, and behavioral symptoms in people with dementia at the end of the 12-week intervention. 22 Although the positive effects of non-pharmacological interventions on dementia symptoms are perceived by family caregivers and described in the literature,11,21,22 to our knowledge, no study has examined in more detail the extent to which family caregivers incorporate non-pharmacological interventions into the care of people with dementia and the potential barriers they experience in implementing these interventions. Therefore, this study addresses the following research question: How are family caregivers currently dealing with the implementation of such approaches, what is the perceived effect, how are they funded, and what are the barriers to incorporating these approaches.
Methods
Study Design and Materials
A structured interview study was conducted to examine the application of and attitudes toward non-pharmacological interventions in dementia care from different health professional stakeholders as well as from family caregivers and people with dementia. In this work, we focus on family caregivers’ experiences and perceptions of (1) personal experiences, including perceived barriers, and knowledge of non-pharmacological interventions, and the (2) effectiveness, applicability, and funding of non-pharmacological interventions. We investigated 2 types of family caregivers: (1) spouse caregivers (at home), and (2) relative caregivers (outside the home). Inclusion criteria were being (1) at least 18 years old, (2) capable of consent (not delirious/no impaired consciousness), (3) having sufficient visual and hearing abilities, and (4) no self-reported physical or mental instability. Participants were recruited nationwide by telephone or email from a diversity of network partners known to the study team as well as from interest groups in Germany. A total of 30 family caregivers had participated in the study by July 2022. To gain a better understanding of our sample, we examined the characteristics of participants in terms of caregiver status, gender, age, and education (see Table 1).
Characteristics of the Study Participants.
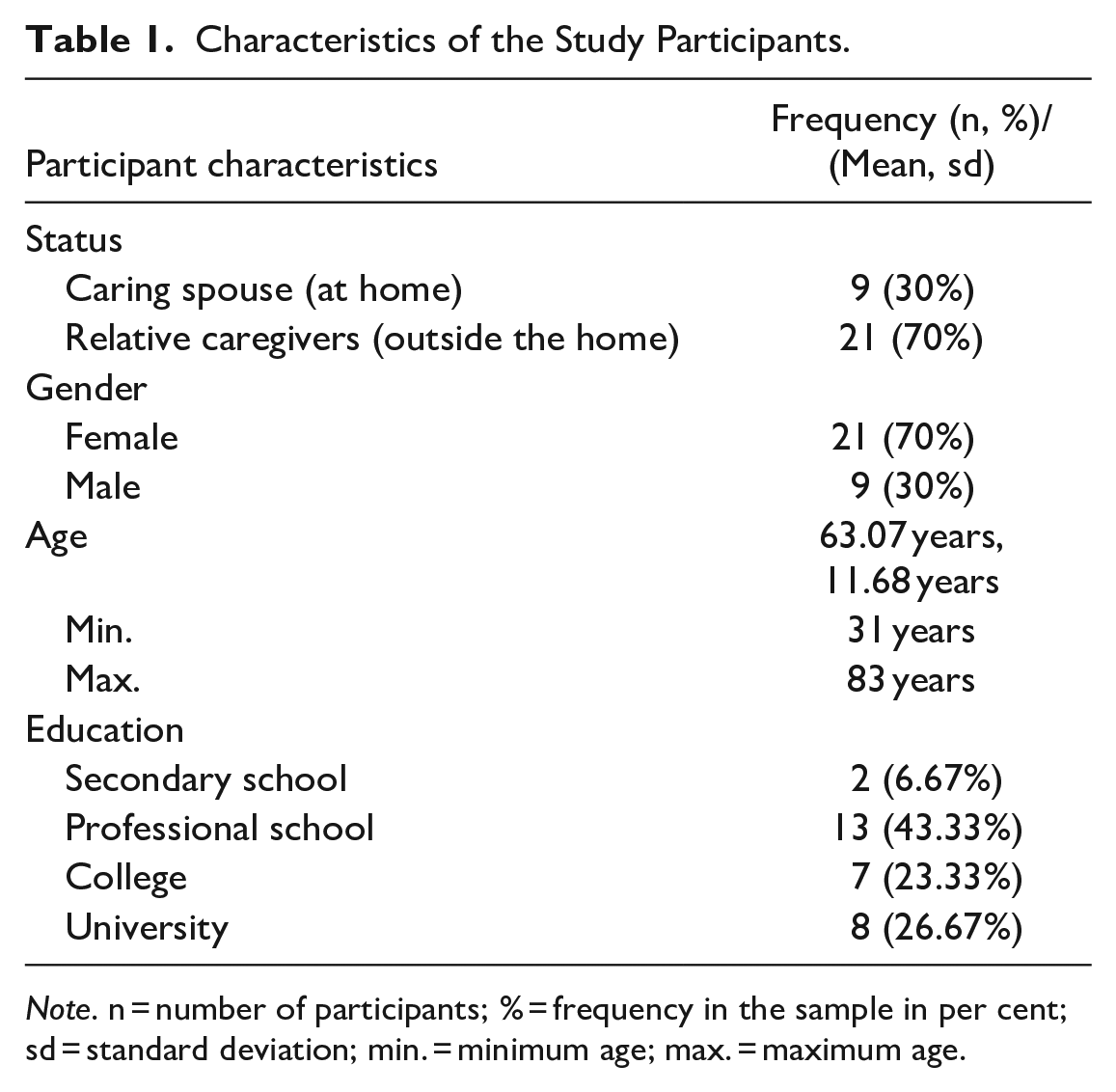
Note. n = number of participants; % = frequency in the sample in per cent; sd = standard deviation; min. = minimum age; max. = maximum age.
Due to the nationwide recruitment approach, designed to obtain a comprehensive overview of non-pharmacological measures in dementia care across the country, interviews were conducted by telephone. If a participant requested an interview in person and this was logistically feasible, this request was complied with. A total of 5 interviews were conducted in person, 25 interviews by telephone.
Interview structure
The interviews lasted approximately 90 minutes, during which, first, the participants’ demographic data were requested. Subsequently, structured questions were used to determine the use of non-pharmacological interventions in the following areas: (1) cognitive measures, (2) sensory measures, (3) therapeutic treatments, (4) physical activity programs, (5) measures to promote functional ability in daily life, (6) household activities, (7) educational opportunities, (8) social relationship management, and (9) leisure activities. The non-pharmacological interventions were based on the recommendations in the “German S3 guidelines on dementia.” 19 In addition, we inquired regarding the perceived effectiveness and funding of the reported non-pharmacological interventions as well as which non-pharmacological interventions were considered most useful for common dementia symptoms, what resources concerning the use of non-pharmacological interventions were missing, and what barriers they experienced when implementing non-pharmacological interventions.
Data Analysis
Descriptive data analysis was conducted to examine the differences in the use of non-pharmacological interventions as well as reported helpful non-pharmacological interventions for common dementia symptoms, missing resources, and barriers to implementing non-pharmacological interventions for family caregivers in dementia care. Because a general lack of funding for non-pharmacological interventions has been noted in the literature, 22 we wanted to investigate whether funding source varied between non-pharmacologic interventions with high versus low frequency. To access those differences in the type of funding, we grouped the reported non-pharmacological interventions into interventions mentioned by at least 50% of family caregivers and such that were not mentioned by as many caregivers (<50%). Between group differences were estimated using chi square tests for the type of funding. All analyses were carried out using Stata version 16 and a significance level of p = .05.
Ethical Approval
Prior to recruitment and data collection, the study was approved by the University Medicine Greifswald’s ethics committee (BB 024/21).
Results
Use of Non-pharmacological Interventions
The most frequently implemented non-pharmacological interventions (over 80%) were, in descending frequency, regular visits from family, friends, and acquaintances, cognitive stimulation, cognitive rehabilitation, and spending time in nature. In contrast, all sensory procedures except massage, all therapy programs, the household activity baking, and leisure activities such as volunteering, drawing, handicrafts, playing musical instruments, learning or using foreign languages etc. were implemented by fewer caregivers (<20%, see Table 2).
Reported Use of Non-pharmacological Interventions in Dementia Care by Family Caregivers.
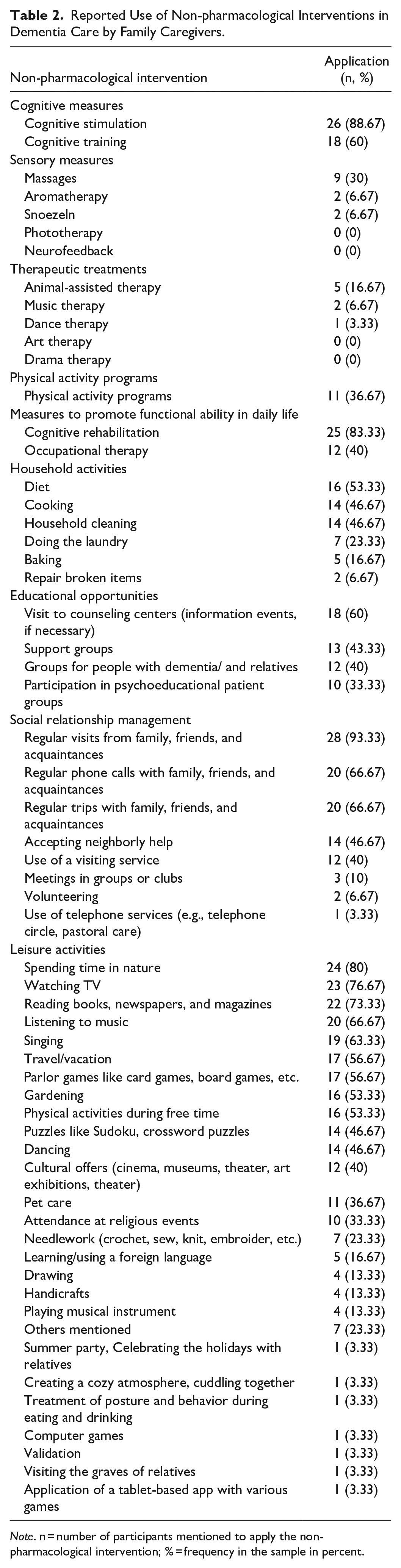
Note. n = number of participants mentioned to apply the non-pharmacological intervention; % = frequency in the sample in percent.
Perceived Effects of non-pharmacological Interventions
Enjoyment (86.67%) was the most frequently cited effect of the non-pharmacological interventions used, followed by perceptions of competence (50%) and well-being (46.67%). A total of 37 different effects were mentioned by family caregivers and addressed a wide range of improved domains, including cognitive-related areas as well as relaxation, social contact, effectiveness in daily living, support, health-related, and emotional aspects (see Table 3).
Most Common Perceived Effects of Non-pharmacological Interventions in Dementia Care by Family Caregivers.
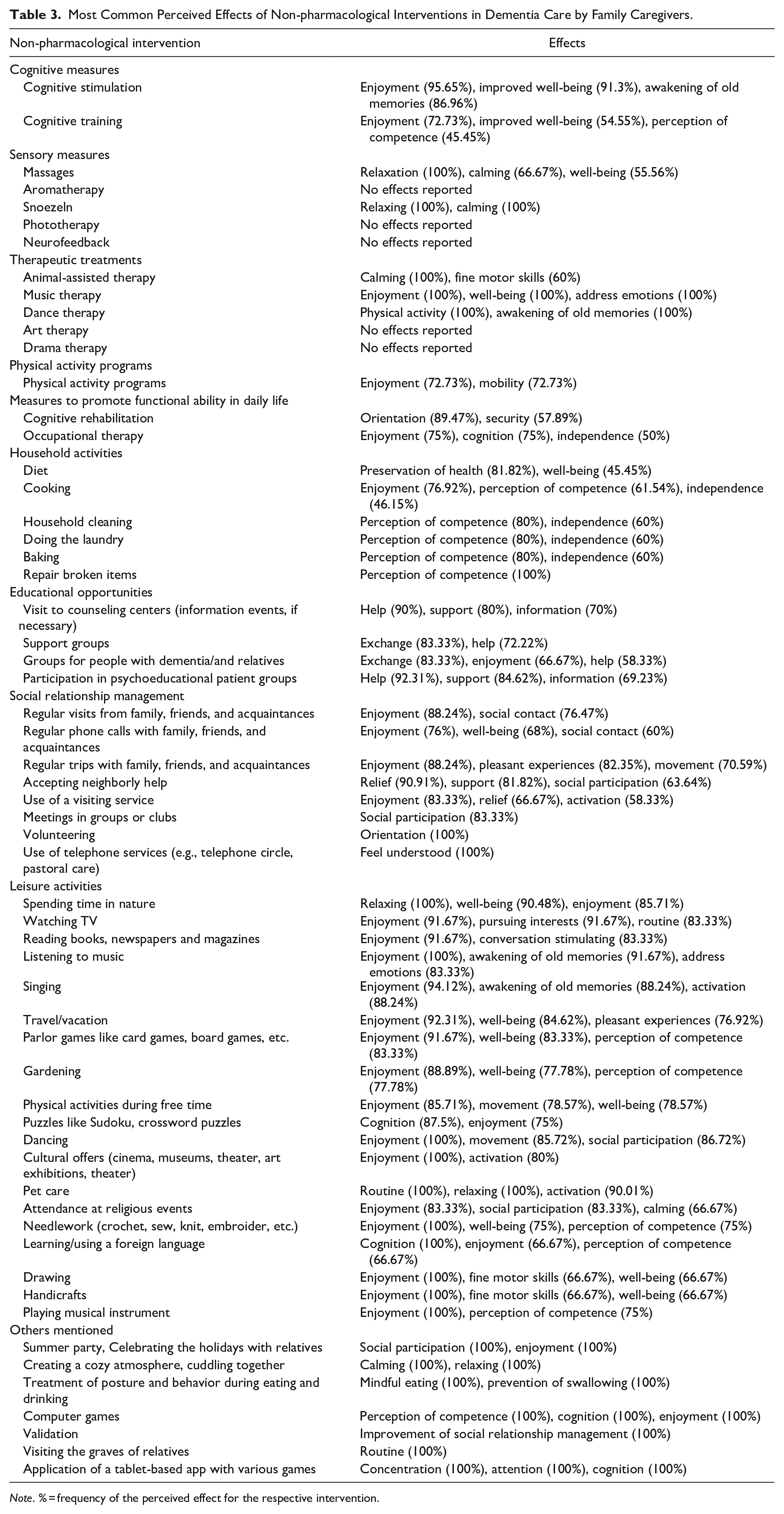
Note. % = frequency of the perceived effect for the respective intervention.
Funding of Non-pharmacological Interventions
Just over 69% of non-pharmacological interventions were reported as not funded. Specifically, either the people with dementia themselves or the caregiver initiated the intervention so that no external costs occurred. This type of funding was reported significantly more frequently for interventions mentioned by at least 50% of caregivers than for interventions that were mentioned by less than 50 % of caregivers (X2 [15, N = 30] = 33.3, p > .004). No significant difference was found for any other funding source (see Table 4).
Reported Funding for Non-pharmacological Interventions.
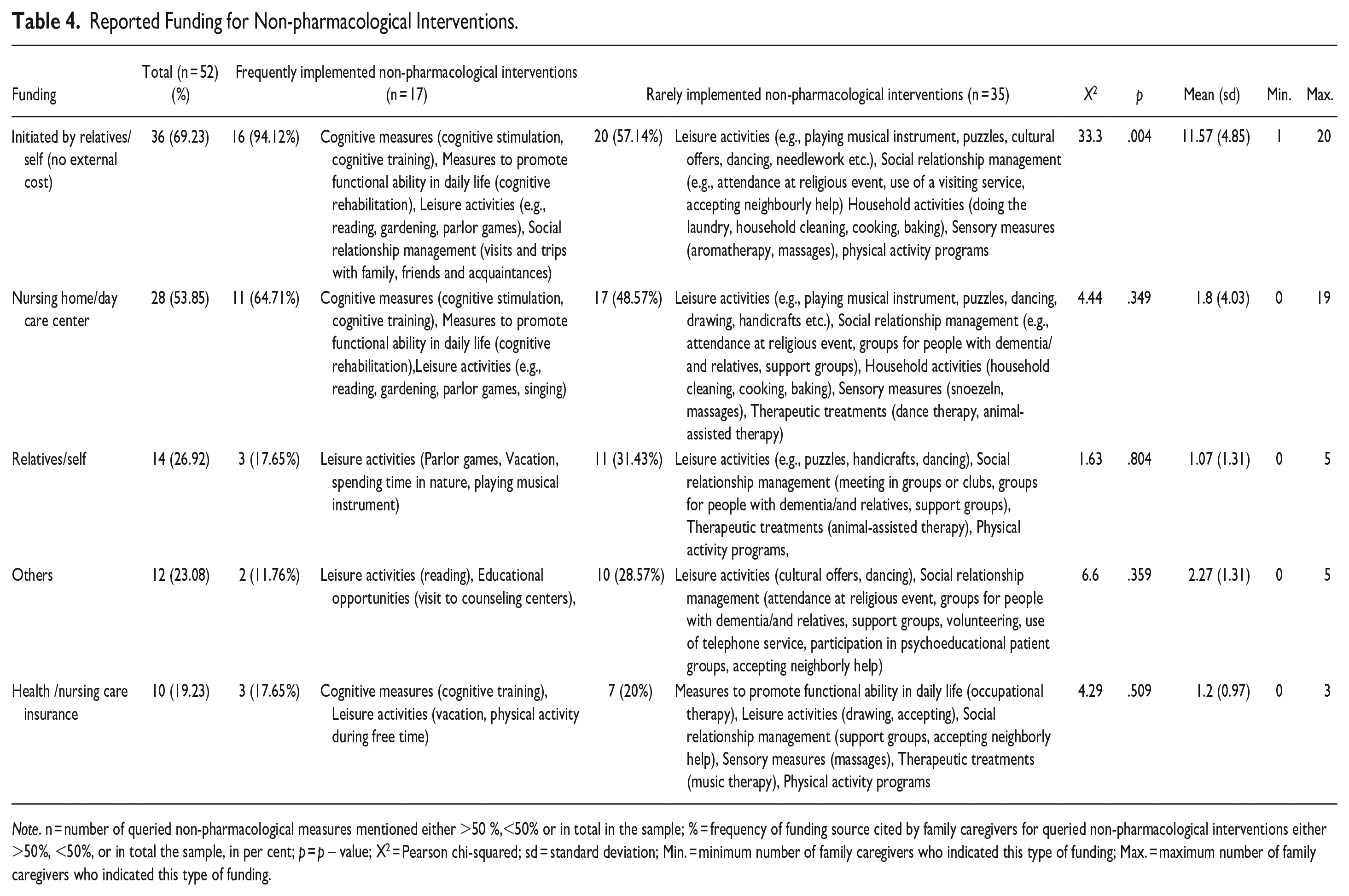
Note. n = number of queried non-pharmacological measures mentioned either >50 %,<50% or in total in the sample; % = frequency of funding source cited by family caregivers for queried non-pharmacological interventions either >50%, <50%, or in total the sample, in per cent; p = p – value; X2 = Pearson chi-squared; sd = standard deviation; Min. = minimum number of family caregivers who indicated this type of funding; Max. = maximum number of family caregivers who indicated this type of funding.
The second most common source of funding was the nursing home or day care center (53.85%), where complete care is financed by nursing care insurance and personal contributions, but family caregivers and people with dementia do not have to pay separately for non-pharmacological interventions, followed by self-funding (26.92%), other funding sources (23.08%) such as association funds, donations and voluntary work, and health or nursing care insurance (19.23%). Rarely implemented interventions (mentioned by less than 50% of the caregivers) were significantly more often paid for by the person with dementia or the caregiver themselves or funded from other sources than frequently implemented interventions (see Table 3). In comparison, frequently implemented interventions (mentioned by at least 50% of the caregivers) were funded by the nursing home or day care center (see Table 4).
Effective Non-pharmacological Interventions for Common Dementia Symptoms
On the questions around family caregiver perceptions as most effective for dementia symptoms, social inclusion was reported by most participants (see Table 5), particularly visits and shared activities. Family caregivers perceived social inclusion to have a positive effect on people with dementia, promoting well-being, delaying cognitive decline, helping with depression, and help with disorientation.
Reports of Effective Measures for Various Dementia Symptoms.
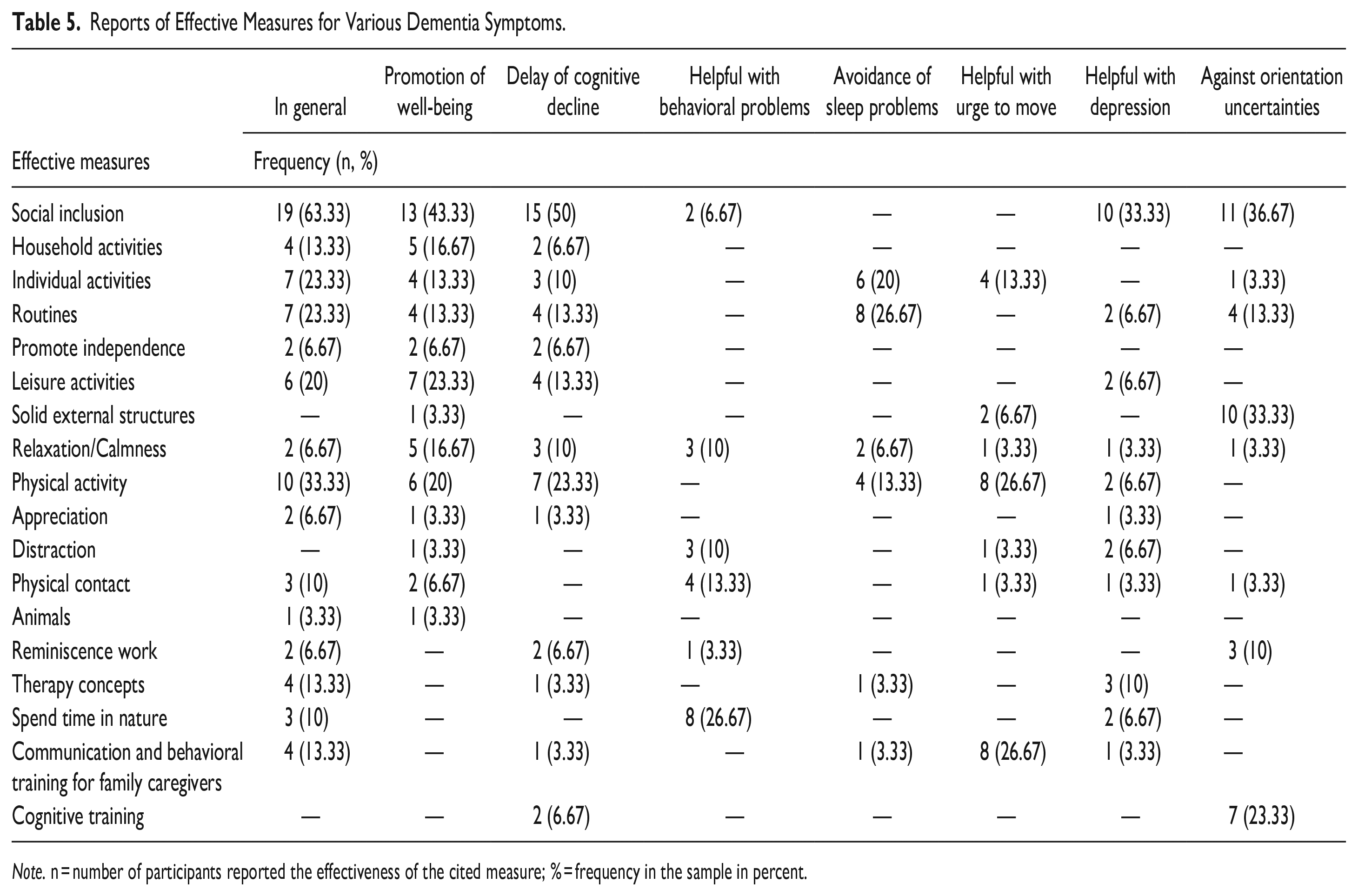
Note. n = number of participants reported the effectiveness of the cited measure; % = frequency in the sample in percent.
For behavioral problems, time in nature was perceived as the best mean to manage this problem. For aggression, physical activity, communication, and behavioral training for family caregivers were reported as effective measures. For sleeping problems, routines were the most frequently cited intervention. Other frequently mentioned effective interventions reported by over 20% of the sample were leisure activities, cognitive training, and a stable structure of daily routines and environmental surrounding that help people with dementia navigate their surroundings and reduce confusion or disorientation. Further details can be found in Table 5.
Lacking Resources for Implementing Non-pharmacological Interventions
Family caregivers desire for the person with dementia to access on-site services, however, there is a shortage of resources available. These include general care services such as visiting services, day care, animal-assisted therapy, art and occupational therapy, and recreational activities such as senior sports and group activities. Further, family caregivers would like to see additional services for people with dementia such as transport services to the respective interventions. Another missing resource is knowledge and support for dealing with behavioral symptoms (such as the reversed day-night rhythm).
Barriers to the Use of Non-pharmacological Interventions
Caregivers cited difficulties in organizing the (participation in the) intervention as the major barrier (46.7%), followed by poor local accessibility, lack of funding, and no discernible benefit of the intervention (see Figure 1). In contrast, insecurity regarding contact with strangers, fear of stigmatization, and lack of knowledge about the content of the offer do not seem to be major barriers to the use of non-pharmacological interventions (see Figure 1).
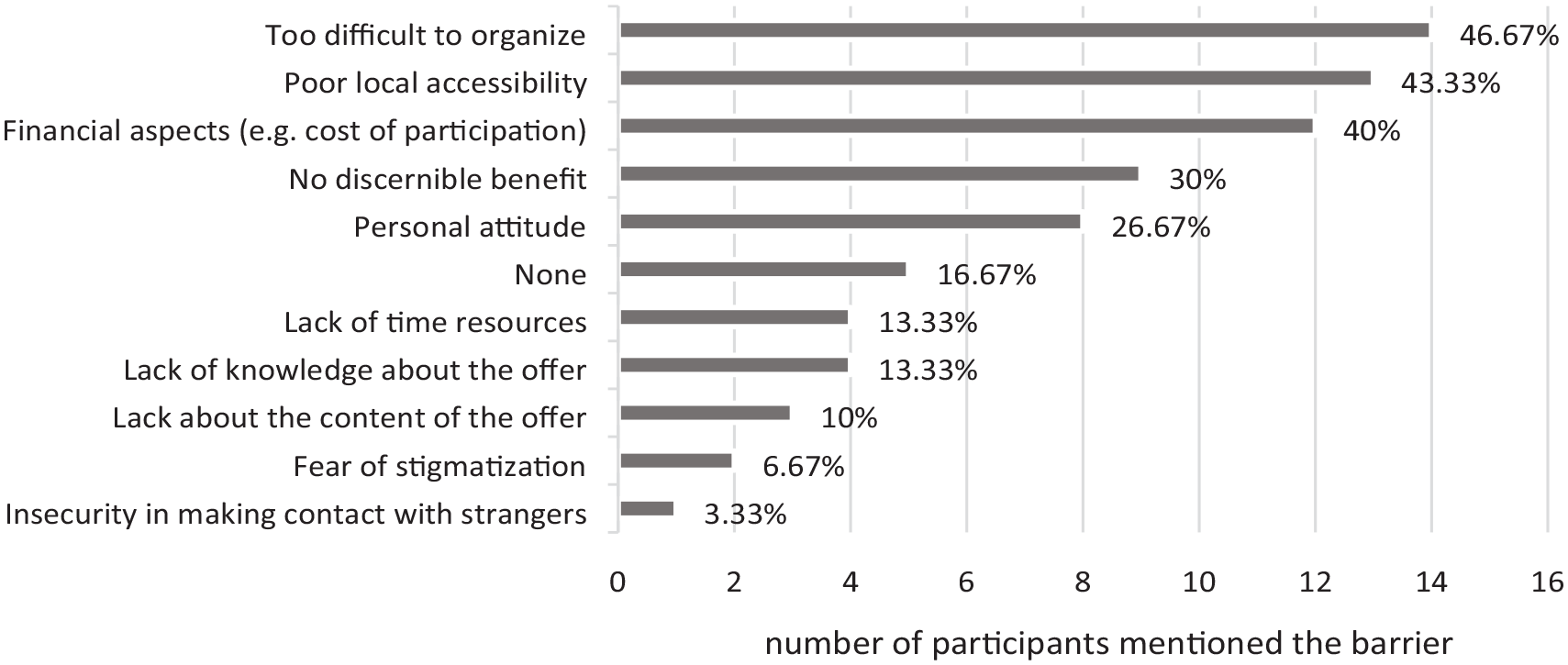
Family caregivers’ barriers to implementing non-pharmacological interventions in dementia care.
Discussion
The aim of our study was to investigate what kind of non-pharmacological interventions are implemented into dementia care by family caregivers, how they are funded and what effects, lack of resources, and barriers they perceive when implementing these interventions. Family caregivers mentioned that maintaining/initiating social contact, cognitively stimulating and rehabilitative activities, and time spent in nature were frequently implemented. Non-pharmacological interventions such as sensory or therapeutic approaches were least frequently implemented.
The fact that sensory or therapeutic approaches were used least frequently is probably not due to lower efficacy. Indeed, literature reviews show positive effects for sensory and therapeutic approaches24,25 of which the effectiveness to improve behavioral and psychological symptoms of dementia and to increase well-being and quality of life is perceived by both, people with dementia and their caregivers.24,25 Rather, the relatively low frequency of use could be related to the fact that these therapies usually have to be self-financed. Our study finds evidence that rarely used interventions were more likely to be self-paid or funded from other sources. In contrast, interventions that can be implemented at little or no financial cost by the person with dementia themselves or by the caregiver are implemented significantly more often. In the literature, this observation is supported by studies indicating a high financial burden for dementia care activities, 20 suggesting that non-pharmacological interventions that need to be self-funded have little to no implementation. On the other hand, we observe a high frequency of self-initiated interventions indicating that caregivers show a great interest in using non-pharmacological interventions in dementia care but try to avoid costs. In addition, the use of fee-based services often involves more organizational effort, a lack of knowledge or information about the possibility of these services, and a lack of availability close to home.
Among the implemented non-pharmacological interventions, family caregivers frequently perceived enjoyment, sense of competence, and well-being as the effects. This observation is consistent with a previously conducted systematic review that examined the efficacy of non-pharmacological interventions in dementia patients, showing that activities perceived as enjoyable by the person with dementia have a positive effect on well-being, self-perception, and self-esteem. 26 An important aspect for experiencing positive effects is the consideration of the interests of people with dementia. 27
The greatest impact on dementia symptoms is the result of social inclusion, as our participating family caregivers reported. Indeed, regular visits are the most commonly mentioned non-pharmacological intervention by our caregivers. Previous research has shown that being socially active can be protective against cognitive decline, 28 enhance quality of life for people with dementia,29,30 and have also beneficial effects on behavioral symptoms. 31 This is particularly true when a social activity is combined with other non-pharmacological interventions, such as musical activities as singing or listening to music together. 32 It is therefore of great importance to involve people with dementia in social activities in order to improve both dementia symptoms and the quality of life of those affected.
Family caregivers indicated that they need effective support services for the implementation of non-pharmacological interventions in dementia care, such as transportation services or appropriate services in rural areas. The need also reflects caregivers’ perceived barriers to implementing non-pharmacologic interventions: difficulties in organizing and lack of local offers. Funding and no discernible benefit of the intervention were also cited as barriers. Several studies report that caring for a person with dementia results in psychological distress, physical illness, and high financial expenses for family caregivers.33,34 It is therefore particularly important to relieve the burden on family caregivers with appropriate support. The need to allocate more resources to non-pharmacological interventions and to increase education about their beneficial effects was identified not only in our study in the German context, but also in a systematic review that included several studies within and outside Europe. 35 Findings from an intervention study highlight that referral and support of family caregivers through appropriate strategies such as communication techniques, environmental adaptations, task simplification, or use of meaningful activities can help manage the behavioral symptoms of dementia and also result in reduced financial expenditures. 36 This underscores the importance of supporting family caregivers more by teaching everyday techniques in dementia care.
There are some limitations to this research. One aspect is that the current study was conducted in Germany. Nonetheless, we believe that many of the points raised are relevant to other countries facing similar challenges for family caregivers, as our results broadly line up with previous findings in the literature. It should be noted that the results provide only an initial, descriptive overview of family caregivers’ views and differentiation regarding the type of dementia and the characteristics of the caregiving situation must be evaluated in further research. Moreover, caregivers can report only their individual experiences that are based on access to information. These represent not an objective but a subjective view on the situation.
Conclusion
Findings from our study suggest that non-pharmacological interventions are frequently implemented by family caregivers who notice positive effects on dementia symptoms. Social contact, in particular, is perceived to promote well-being, delay cognitive decline, help with depression, and eliminate orientation uncertainties. However, the implementation of non-pharmacologic interventions depends on organizational effort, funding, local access to offers, and whether benefit of the intervention is discernable. Therefore, education about non-pharmacological interventions in dementia care should be part of the counseling provided to people with dementia and their family caregivers and to support them in their implementation. In home care, informal caregivers can engage the person with dementia in daily activities with as little assistance as possible, allow them to participate in social life, create memory books to relive memories, and find meaningful activities based on the current interests and abilities of the person with dementia. Future investigations should develop programs that support caregivers in implementing simple and cost-effective non-pharmacological interventions. Only in this way, the full potential of non-pharmacological interventions can be realized in order to maintain a good quality of life for as long as possible. Effective implementation of non-pharmacological measures might also alleviate caregiver burden as well as nursing care costs and therefore be considered as critical components of home health care management and practice.
Footnotes
Acknowledgements
We thank all study participants for their contributions.
Previous Publications
None.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: F.S.R. received a research grant by Anoia GmbH to evaluate the usability of a tablet app for people with dementia. S.D.R. and N.Z. declare that they have no conflict of interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Availability of Data and Materials
Data available only for proof of scientific validity. Due to privacy/ethical requirements data cannot be made accessible to external persons.