
Abstract
Objectives
Despite recommendations to increase the uptake of colorectal cancer (CRC) screening, trends in CRC screening vary with sociodemographic status. We aimed to evaluate trends in CRC screening in the US population and subpopulations.
Methods
A total of 1,082,924 participants aged 50 to 75 from five cycles (2012, 2014, 2016, 2018, and 2020) of the Behavioral Risk Factor Surveillance System were involved. Multivariable logistic regression models were performed to evaluate linear trends in CRC screening utilization from 2012 to 2018. Rao-Scott chi-square tests were used to assess the differences in CRC screening utilization between 2018 and 2020.
Results
The estimated percentage reporting up-to-date with CRC screening increased significantly (P for trend <0.001), from 62.8% (95% CI, 62.4%−63.2%) in 2012 to 66.7% (95% CI, 66.3%−67.2%) in 2018 and 70.4% (95% CI, 69.8%−71.0%) in 2020, in accordance with 2008 US Preventive Services Task Force recommendations. Trends followed similar patterns in most subgroups, although with different magnitudes in several subgroups, primarily those underweight showed a stable percentage over time (P for trend = 0.170). In 2020, 72.4% of participants reported they were up to date with CRC screening, including the utilization of stool DNA tests and virtual colonoscopy. Colonoscopy was the most commonly used test in 2020 (64.5%), followed by FOBT (12.6%), stool DNA test (5.8%), sigmoidoscopy (3.8%), and virtual colonoscopy (2.7%).
Conclusions
In this nationally representative survey of the US population from 2012 through 2020, the percentage reporting up to date with CRC screening has increased, but not equally among all subgroups.
Introduction
Colorectal cancer (CRC) is the third leading cause of cancer death both worldwide and in the United States. 1 It is also considered to be a nearly ideal disease for screening with a lengthy, trackable, premalignant phase, during which early detection and simple interventions can prevent progression to advanced and metastatic stages. 2 Decades-long declines in both CRC incidence and mortality have been demonstrated, largely attributed to the early promotion of guidelines from the American Cancer Society (ACS) and other key organizations.3,4 The ACS guidelines for CRC screening were first presented to the public and health professionals in 1980, and have been updated periodically since then.5,6 Other professional organizations have also released regular screening for CRC with both invasive and noninvasive options, particularly the US Preventive Services Task Force (USPSTF), the American College of Radiology, and the US Multi-Society Task Force on Colorectal Cancer.7,8 The organizational guidelines have grown similar over time, and the combination with coverage for Medicare beneficiaries reflects the consensus on the value and patterns of CRC screening in the United States. 6
Despite recommendations and emerging strategies, CRC screening rates had not yet met the Healthy People 2020 target of 70.5% within most “vulnerable” subpopulations, including racial and ethnic minorities, and low-income, uninsured, and rural populations. 9 Moreover, the broad variation in preference for and adherence to the CRC screening tests is not only attributable to the inequalities in socioeconomic status, healthcare access, and awareness of the growing problem of CRC, but also largely a function of which tests are offered by referring physicians and gastroenterologists. 10 Although each adult should be offered the full range of CRC screening options, colonoscopy and fecal occult blood test (FOBT) or fecal immunochemical test (FIT) are principally recommended regardless of how screening is offered, and the simpler, lower-budget options are available in most settings. 11 Furthermore, multiple screening options and subsequent practical considerations challenge the physicians to offer optimal screening for an individual patient in the setting of opportunistic screening, which may also influence the screening uptake.12,13
Trends in CRC screening remain poorly described in the US for adults and subpopulations with varying sociodemographic status. Prior studies did not report trends by various subgroups and were limited by regional data or small sample sizes.14,15 Understanding trends in the uptake of CRC screening may be of benefit to identify potential problems of underuse and misuse of screening and guide the development of national public health policies for targeted interventions aimed at eliminating health disparities. To address these issues, trends in the utilization of CRC screening in time overall and by sociodemographic status were evaluated in this study using a large nationally representative sample of US adults.
Methods
Study population
The Behavioral Risk Factor Surveillance System (BRFSS) is an annual, nationwide, telephone-administered survey of randomly sampled US adult residents to collect information on health-related risk behaviors, chronic medical conditions, preventive health practices, and healthcare access. 16 Survey data were available for all 50 states and the District of Columbia. This study used publicly available BRFSS data and was thus exempt from Centers for Disease Control and Prevention institutional review board approval.
The study involved five cycles (2012, 2014, 2016, 2018, and 2020), with 2012 representing the first cycle of continuous BRFSS because of the new weighting procedures, which are likely to affect trend lines when comparing BRFSS data collected before and after 2011. Each cycle is an independent sample. Of 1,172,842 participants aged 50–75 years, we excluded 89,918 participants who declined to answer, had a missing answer, or who answered “don’t know/not sure” to CRC screening status. Finally, 1,082,924 participants were involved in our study.
Assessment of CRC screening
BRFSS respondents aged ≥50 years were asked whether they had ever used “a special kit at home to determine whether the stool contains blood (stands for FOBT)”; whether they had ever had a colonoscopy to check the entire colon or a sigmoidoscopy which checks part of the colon; and when these tests were last performed. In 2020, for the first time, the BRFSS included questions on stool DNA testing and computerized tomographic colonography. However, because CRC screening was disrupted in the US during the first quarter of 2020 with the emergence of the COVID-19 pandemic, 17 2018 represents the most recent cycle for which data are available and comparable in the analysis for linear trends for consistency over time.
In accordance with the USPSTF recommendations for CRC screening in 2008, 18 up to date with CRC screening (i.e. have completed a CRC screening test within the recommended time interval) through 2012 to 2020 was defined as having had (1) a home stool blood test (FOBT or FIT) within 1 year, and/or (2) sigmoidoscopy within 5 years with FOBT or FIT within 3 years, and/or (3) colonoscopy within 10 years.
In addition, we described the utilization of CRC screening in 2020 in accordance with current USPSTF recommendations for CRC screening in 2021. 1 Up to date with CRC screening was defined as having had an FOBT within the past year, sigmoidoscopy within the past 5 years, colonoscopy within the past 10 years, stool DNA test within the past 3 years, virtual colonoscopy within the past 5 years, and/or sigmoidoscopy within the past 10 years combined with a blood stool test in the past year.
Assessment of demographic characteristics
Self-reported characteristics included gender, age (50–64, 65–75 years), race/ethnicity (non-Hispanic White, non-Hispanic Black, other/multiracial, and Hispanic), educational level (less than high school graduate, high school graduate, attend college/technical school and college/technical school graduate), annual household income (<$15,000, $15,000 to <$25,000, $25,000 to <$35,000, $35,000 to <$50,000, ≥$50,000), insurance status (yes, no), could not see doctor because of cost (yes, no). In addition, BMI was categorized as underweight (BMI < 18.5 kg/m2), normal weight (18.5 ≤ BMI < 25 kg/m2), overweight (25 ≤ BMI < 30 kg/m2), class I obesity (30 ≤ BMI < 35 kg/m2), class II obesity (35 ≤ BMI < 40 kg/m2), and class III obesity (BMI ≥ 40 kg/m2).
Statistical analysis
Estimates on proportions and 95% confidence intervals (95% CIs) of up to date with CRC screening and utilization of specific screening modalities were separately calculated by cycle. Multivariable logistic regression models were used to evaluate linear trends in CRC screening utilization (up to date with CRC screening, colonoscopy within 10 years, and FOBT within a year) across survey cycles and to estimate regression coefficients (β) and 95% CIs for every 2-year change, adjusted for age (50−64 and 65−75 years). P for trends was estimated using the survey cycle as a continuous variable. Absolute differences in the estimated percentage of CRC screening were calculated by comparing the 2018 cycle with the 2012 cycle. Rao-Scott chi-square test was performed to assess the differences between 2018 and 2020. Stratification analyses by gender, race/ethnicity, education level, annual household income level, insurance status, and BMI category were performed. All statistical analyses incorporated the individual weights, strata, and cluster variables to account for the survey sampling strategy and enhance generalizability to the US population, and were performed using SPSS (Version 24.0, IBM SPSS), with a 2-sided significance level set at P-value <0.05. In the results presentation, a P for trend <0.05 and β > 0 represent an “increase”, a P for trend <0.05 and β < 0 represent a “decrease,” and P for trend ≥0.05 represent “stable.”
Results
The main characteristics of 1,082,924 participants are presented in Table 1, and the study population per cycle ranged in size from 175,698 to 238,425. The percentage of participants with less than high school education decreased from 13.5% in 2012 to 13.0% in 2018, and 12.2% in 2020, whereas those with at least college graduate education increased from 27.0% to 29.1%, and then 30.4% during the same period. The percentage of participants with annual household income ≥$50,000 varied from 46.7% to 53.1% from 2012 to 2018 and increased to 55.4% in 2020, and those with health insurance from 88.8% in 2012 to 93.0% in 2018 and 2020.
Sociodemographic characteristics of US adults aged 50–75 by BRFSS survey cycle, 2012 to 2020.
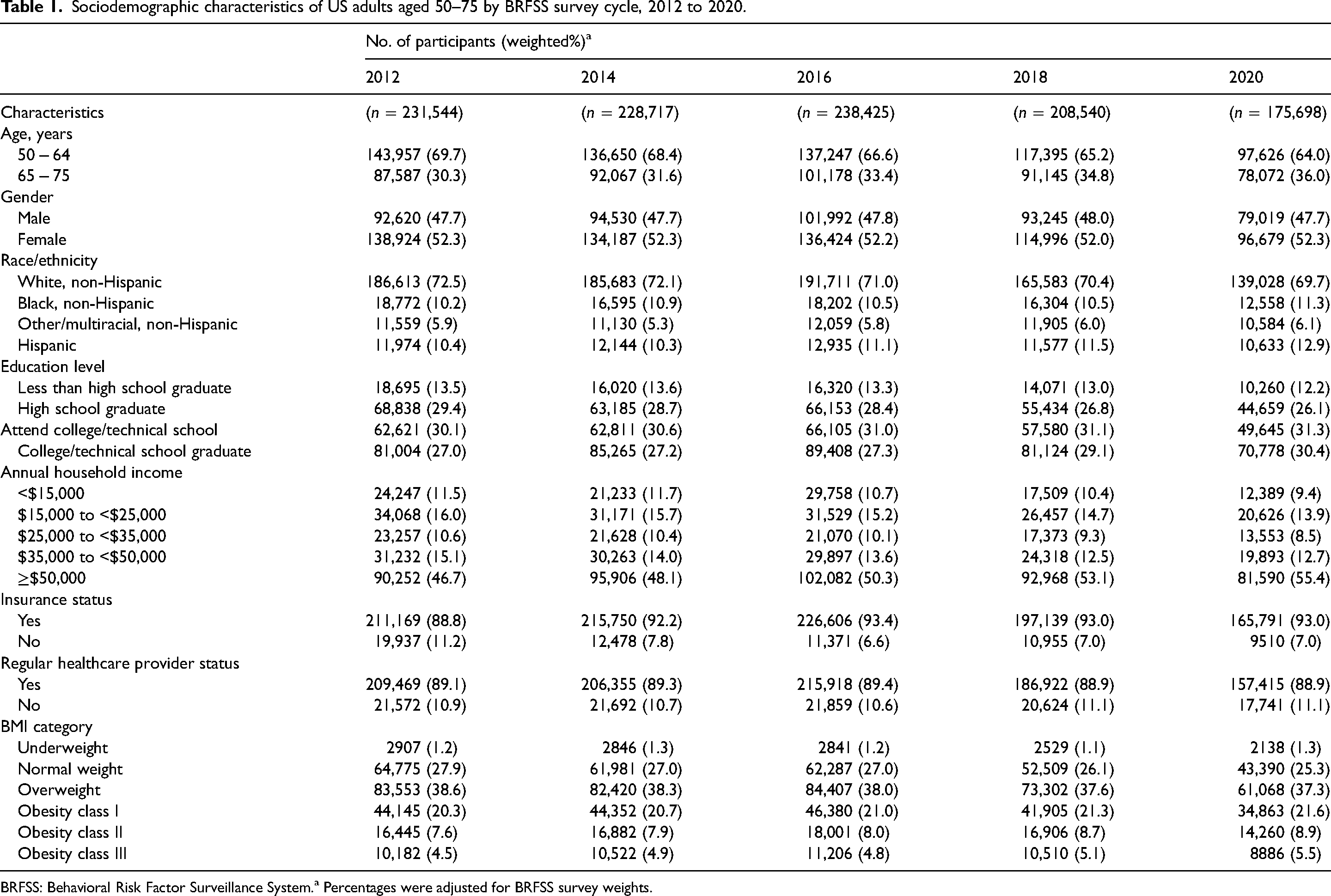
BRFSS: Behavioral Risk Factor Surveillance System.a Percentages were adjusted for BRFSS survey weights.
CRC screening from 2012 to 2018
From 2012 to 2018, the estimated percentage reporting up to date with CRC screening and use of either colonoscopy or FOBT in time significantly increased (P for trend <0.001). The percentage reporting up to date with CRC screening increased from 62.8% (95% CI, 62.4%−63.2%) in 2012 to 66.7% (95% CI, 66.3%−67.2%) in 2018 (difference, 4.3% [95% CI, 3.6%−5.0%]) (Figure 1a; Supplemental Appendix Table 1). Similar patterns could be observed in colonoscopy and FOBT or FIT use (Supplemental Appendix Tables 2 and 3).
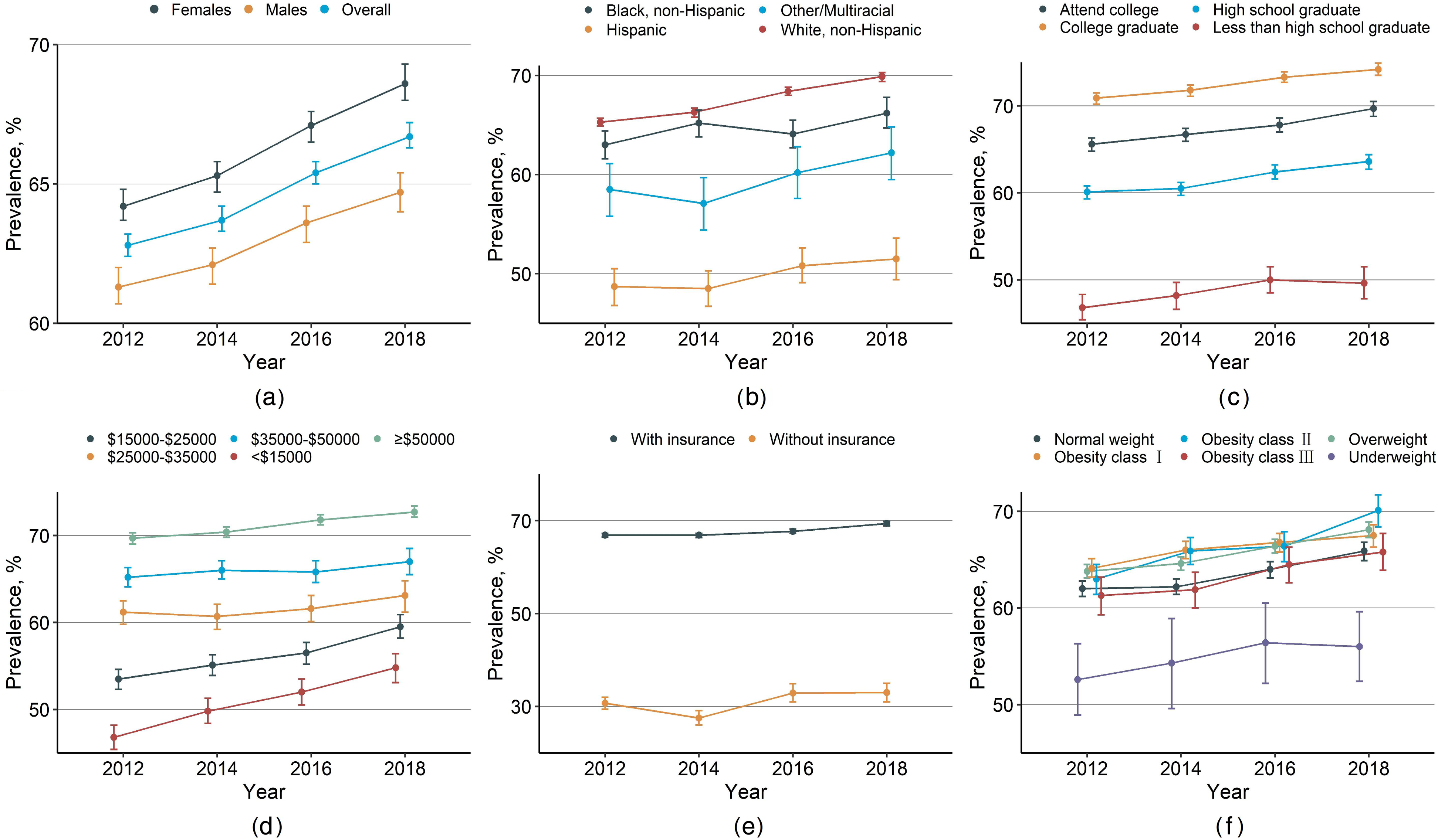
Crude weighted trends in CRC screening in US adults aged 50–75. Trends in CRC screening by: (a) gender, (b) race/ethnicity, (c) education level, (d) annual household income, (e) insurance status, and (f) BMI category. Data were weighted to be nationally representative. Error bars indicate 95% CIs.
In most subgroups, trends in being up to date between 2012 and 2018 followed similar patterns, although with different magnitudes in subgroups including non-Hispanic Blacks and underweight participants, which remained stable over time (Figure 1). Despite a significant increase being observed for those with annual household income <$15,000 (P for trend <0.001; difference, 8.0% [95% CI, 5.8%−10.1%]), the percentage reporting up to date was consistently lower than for the higher-income subgroups in all time periods. As educational and annual household income levels increased, the percentage reporting up to date increased and the difference between subgroups decreased (Figure 1c and d). The percentage of participants with health insurance reporting up to date was more than twice that of those without any health care coverage (Figure 1e). Similar trends were evident in the use of either colonoscopy or FOBT (see detailed subgroup results in Supplemental Appendix Tables 2 and 3).
Percentage reporting CRC screening test use, by test type and selected characteristics: BRFSS, United States, 2018 and 2020 a .
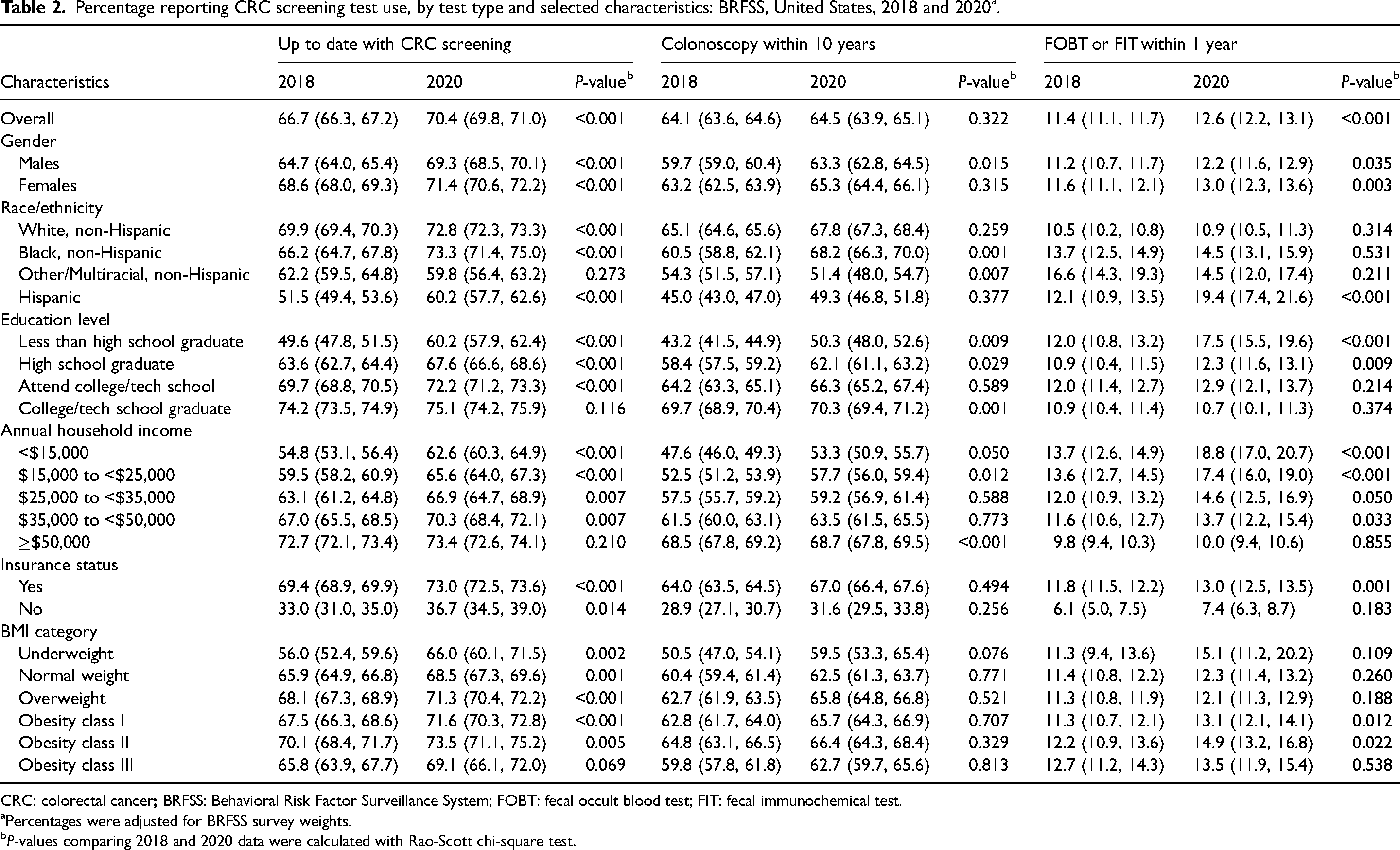
CRC: colorectal cancer
Percentages were adjusted for BRFSS survey weights.
P-values comparing 2018 and 2020 data were calculated with Rao-Scott chi-square test.
Percentage reporting CRC screening test use in accordance with 2021 USPSTF recommendations: BRFSS, United States, 2020 a .
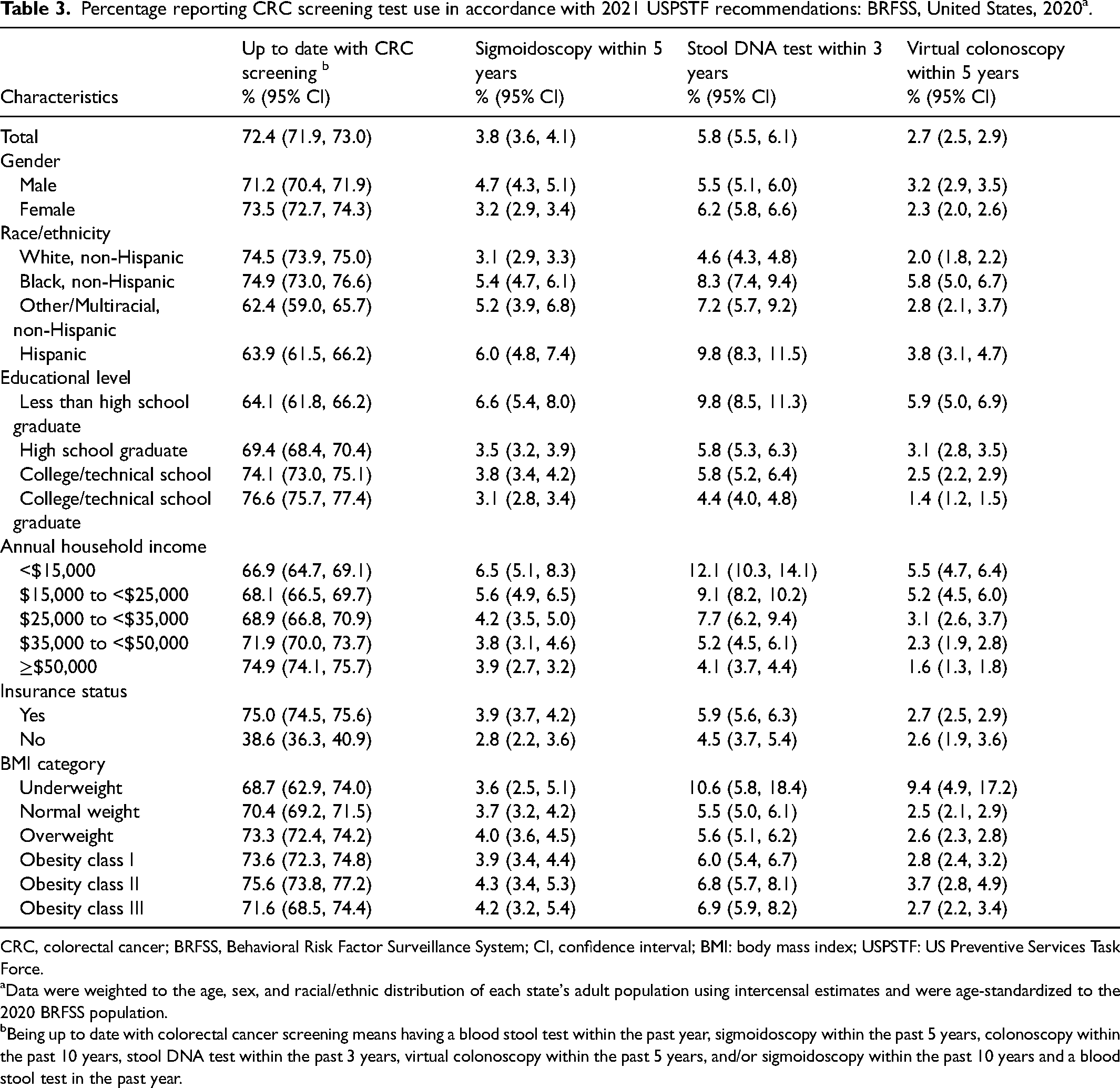
CRC, colorectal cancer; BRFSS, Behavioral Risk Factor Surveillance System; CI, confidence interval; BMI: body mass index; USPSTF: US Preventive Services Task Force.
Data were weighted to the age, sex, and racial/ethnic distribution of each state's adult population using intercensal estimates and were age-standardized to the 2020 BRFSS population.
Being up to date with colorectal cancer screening means having a blood stool test within the past year, sigmoidoscopy within the past 5 years, colonoscopy within the past 10 years, stool DNA test within the past 3 years, virtual colonoscopy within the past 5 years, and/or sigmoidoscopy within the past 10 years and a blood stool test in the past year.
CRC screening from 2018 to 2020
Between 2018 and 2020, the estimated percentage reporting CRC screening in time increased by 5.5% (from 66.7% (95% CI, 66.3%−67.2%) to 70.4% (95% CI, 69.8%−71.0%), P < 0.001) and the use of FOBT increased by 11% (from 11.4% (95% CI, 11.1%−11.7%) to 12.6% (95% CI, 12.2%−13.1%), P < 0.001) (Table 2). No similar trend was found in the use of colonoscopy (P = 0.322). Although the proportions reporting utilization of a specific screening test were significantly greater in 2020, the colonoscopy use in subgroups including the participants with other or multiracial race/ethnicity decreased (from 54.3% (95% CI, 51.5%−57.1%) in 2018 to 51.4% (95% CI, 48.0%−54.7%) in 2020, P = 0.007) (Table 2).
In accordance with current 2021 USPSTF recommendations, 72.4% of participants in 2020 reported they were up to date with at least one of the CRC screening tests, and colonoscopy was the most commonly used test (64.5%), followed by FOBT (12.6%), stool DNA test (5.8%), sigmoidoscopy (3.8%), and virtual colonoscopy (2.7%) (Table 3). Percentages reporting stool DNA test and virtual colonoscopy use were notably higher among participants with an education level less than high school, participants with annual household income <$15,000, and Hispanics.
In multivariate logistic regression models that adjusted for age and other covariates, the survey cycle was significantly associated with being up to date with CRC screening, with the likelihood of CRC screening compliance tending to increase over time (odds ratio (OR) for CRC screening compliance was 1.12 (95% CI, 1.07−1.17) in 2018 compared with 2012, P for trend <0.001; and 1.11 (95% CI, 1.07−1.16) in 2020 compared with 2018). Similar patterns were found for FOBT use. In contrast, an inverse association was observed between the survey cycle and the use of colonoscopy (OR = 0.94 (95% CI, 0.90−0.98)). The ORs for the likelihood of being up to date, colonoscopy use, and FOBT or FIT use in time were 0.73 (95% CI, 0.66−0.82), 0.67 (95% CI, 0.60−0.74), and 1.58 (95% CI, 1.34−1.85), respectively, for participants with other or multiracial race/ethnicity, and were 0.87 (95% CI, 0.80−0.94), 0.76 (95% CI, 0.70−0.82), and 1.71 (95% CI, 1.53−1.92), respectively, for Hispanics. For whole models of multivariate logistic regression see Supplemental Appendix Tables 4 and 5.
Discussion
From 2012 to 2018, the estimated percentage reporting up to date with CRC screening and use of either colonoscopy or FOBT in US adults aged 50−75 years rapidly and significantly increased, and increases can also be observed between 2018 and 2020. Although these trends were comparable among most subgroups, for participants with health insurance, higher education level, or higher income a higher estimated rate was reported. In 2020, 72.4% of participants reported they were up to date with CRC screening, which did reach the Healthy People 2020 target (70.5%).
Prior studies from the CDC reported that the percentage of US adults reporting up-to-date with CRC screening increased from 65% in 2010 to 65.1% in 2012, 62.4% in 2015, and 68.8% in 2018, which are all below the rate in 2020.19–21 Despite no national program, the United States has achieved the world's highest rates of CRC screening compliance, using an almost entirely opportunistic approach. 12 Moreover, the removal of cost-sharing enacted in 2010 by the Affordable Care Act has provided federal support for states to expand Medicaid insurance coverage to low-income adults, which has been hypothesized to improve screening and other health outcomes.22,23 An immediate effect of CRC screening may not be visible due to the delay between gaining insurance and completing multi-step screening, and most uninsured people have the need to treat more immediate health conditions or symptoms than cancer screening, but the modest improvements in screening uptake could progress further. 24 Moreover, the nationwide goal launched in 2014 by the National Colorectal Cancer Roundtable that 80% of adults aged 50 and above be routinely screened by 2018 has strengthened the capacity to address screening and benefited the screening rates measurably.25,26
It is important to highlight that disparities in CRC screening uptake still persist. 27 For instance, CRC screening rates among Whites and English-speaking Hispanics were substantially and consistently higher than for Spanish-speaking Hispanics, according to prior studies and reports from the CDC.21,28 It is worth noting that although screening rates for Blacks have been lower than for Whites historically,28,29 these two groups had similar rates in 2020 as shown in Table 3, which may be attributable to the expanding health insurance access to low-income individuals. In addition to presenting racial/ethnic screening disparities, prior studies also highlighted disparities by socioeconomic status and access to healthcare.14,30 National suspensions following the emergence of COVID-19 have contributed to an approximately 25% drop from baseline levels in cancer screening, which then created backlogs that systems will need to address, such as the already disproportionate and pronounced disparities experienced by medically underserved communities.17,31 Nevertheless, the ACS is leading a 17-month intervention with 22 federally qualified health centers across the nation to alleviate additional strain caused by COVID-19, and CRC-specific calls to action were recommended, which may all have contributed to the striking increases in reporting up to date with screening.31,32
Fedewa et al. 17 found that an increase in conventional stool testing counterbalanced a 16% decline in colonoscopy, allowing CRC screening to remain stable during the pandemic. The uptake of stool testing is continuously promoted by most organizations that promote CRC screening, and the ACS 2015 guideline also listed stool testing as one of the options that all adults should receive. 33 Nevertheless, of the CRC screening tests, colonoscopy still predominates in a number of countries including the United States, which is consistent with our study.10,34 We boldly hypothesize that the increases in CRC screening compliance in recent years may be attributed partly to the development of less invasive and inexpensive screening modalities, which may counterbalance the slight decline in the uptake of invasive screening tests including colonoscopy. Prior studies have reported that the availability of new, non-invasive screening modalities, referring to stool and blood-based tests along with radiologic tests like the stool DNA test, provides yet other viable options for CRC screening.7,35 Despite the continued development of noninvasive tests and improved understanding of optimal screening intervals, whether these contribute to further shifting among existing screening modalities and improvements in efficiency and adherence in the long term is yet to be determined.1,36
Meanwhile, obesity, particularly of class II/III, which is associated with a higher incidence of CRC and a higher mortality from the disease, appears to be a deterrent to screening, and could also be a vital clinical marker of the need for screening.37,38 To boost CRC screening rates, strategies have been described that emphasize the importance of identifying adults with higher CRC risk in a systematic way. For instance, risk stratification models with substantial accuracy in defining high- and low-risk subgroups have been proposed to predict the risk of important precancerous lesions. 39 The subgroups with a predicted higher risk of such lesions, including those with obesity, are referred directly to colonoscopy, whereas those with lower risk are referred to screening tests with less risk and cost than colonoscopy. 12 However, given the fact that the BRFSS as the largest telephone survey has raised concerns on its reliability and validity, especially when reporting data such as height and weight, further studies and efforts to identify CRC screening rates among patients with obesity appear well justified.
Limitations
This study has several limitations. First, although we excluded participants who declined to answer, had a missing answer, or who answered “don’t know/not sure” to CRC screening status, it is possible that some tests considered as screening were for diagnosis or surveillance. Second, changes in the CRC screening database and assessments of ‘up to date’ over the study period may have affected estimated trends in CRC screening. Third, CRC screening and characteristics including BMI were self-reported and not verified by medical records or claims data, and some states paused interviews during COVID-19-related shutdowns.
Conclusions
In this nationally representative survey of the US population from 2012 through 2020, the percentages of up to date with CRC screening, colonoscopy within 10 years and FOBT within a year have increased, but not equally among all subgroups.
Human rights
All studies involving human participants were approved by the institutional review committee, and were performed in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Supplemental Material
sj-docx-1-msc-10.1177_09691413231174163 - Supplemental material for Trends in colorectal cancer screening in the United States, 2012 to 2020
Supplemental material, sj-docx-1-msc-10.1177_09691413231174163 for Trends in colorectal cancer screening in the United States, 2012 to 2020 by Yue He, Tong Xu, Jiaxin Fang, Li Tong, Wenhui Gao, Yuan Zhang, Yanfang Wang, Yan Xu, Shunyao Shi, Siyu Liu and Lina Jin in Journal of Medical Screening
Footnotes
Data availability statement
The data that support the findings of this study are openly available at ![]() . Information from the BRFSS is made available through an extensive series of publications and articles in scientific and technical journals. For data users and researchers throughout the world, survey data are available on the internet and on easy-to-use CD-ROMs.
. Information from the BRFSS is made available through an extensive series of publications and articles in scientific and technical journals. For data users and researchers throughout the world, survey data are available on the internet and on easy-to-use CD-ROMs.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
All participants signed written informed consent, and the National Center for Health Statistics ethics review committee approved the study protocol.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.