
Abstract
Objective
Age, sex, and deprivation are known factors influencing colorectal (bowel) cancer screening uptake. We investigated the influence of these factors on uptake over time.
Methods
Data from the Scottish Bowel Screening Programme (SBoSP) were collected between 2007 and 2014. End-points for analysis were uptake, faecal occult blood test positivity, and disease detection, adjusted for age, sex, deprivation, and year of screening.
Results
From 5,308,336 individual screening episodes documented, uptake gradually increased with increasing age up to 65–69 and was lower in men than women (52.4% vs. 58.7%, respectively). Deprivation had a significant effect on uptake by men and women of all age groups, with the most deprived least likely to complete a screening test. Uptake has increased with time in both sexes and across the deprivation gradient. The number needed to screen to detect significant neoplasia was significantly lower in men than women overall (170 vs. 365), and this held over all age and deprivation groups. The number needed to screen was also lower in the more deprived population.
Conclusions
Although lower age, male sex, and increased deprivation are associated with lower bowel cancer screening uptake in Scotland, uptake has increased since SBoSP introduction in all age groups, both sexes, and across the deprivation gradient. Despite a lower uptake, the number needed to screen to find significant disease was lower in men and in those with higher levels of deprivation.
Introduction
Population-based colorectal cancer (CRC) screening using faecal occult blood tests (FOBT) leads to a reduction in cause-specific mortality.1–3 Risk is associated with age, sex, and socioeconomic deprivation, particularly in men. Those in the most socioeconomically deprived groups have a 20% greater incidence of CRC than those in the least deprived. 4 There is also evidence that, following a CRC diagnosis, more deprived patients have both poorer cancer-specific and overall survival. 5
Population-based CRC screening programmes using FOBT across the four countries of the United Kingdom have an overall uptake just over 50%.6,7 Age, sex, deprivation, and ethnicity are known factors that influence screening uptake, with those who are younger, male, more deprived, and from particular ethnic minority groups being less likely to engage in screening.6,8 The reasons for older age groups to be more willing to engage with CRC screening are unclear, but having more free time, higher media exposure due to increased reading and television-watching behaviours, and increasing concern with health matters might contribute. Sex is also a predictor of uptake, and while an FOBT does not require time off work, these differences may still reflect occupational demands, as men are more likely than women to be in paid employment up to age 65. 9 It may be that full-time employment reduces time spent at home and, thus, opportunities to collect samples, which may explain lower uptake in men aged 50–59. Alternatively, younger men may not be persuaded of the need for preventive healthcare, a worrying trend given that age and sex specific 10-year cumulative incidence and mortality rates of CRC suggest that men should begin screening earlier than women. 10 There are probably multiple reasons for the major effect of deprivation on uptake, but good evidence suggests that low health literacy is associated with perceived confidence to participate in screening, and literacy declines with increasing deprivation.11,12 This may be a particular problem with bowel screening programmes which, in contrast with other screening programmes, do not involve an initial interaction with a healthcare professional but rely heavily on printed information delivered by post. Access to screening is precluded as the rationale for these observations in the Scottish Bowel Screening Programme (SBoSP) because test kits are mailed and returned postage free, and the test is completed at home.
Many studies have examined strategies to improve uptake, but little is known about how uptake by age, sex, and deprivation change over time in the absence of interventions. The SBoSP was introduced over the 14 Scottish NHS Boards in a staged roll-out beginning in 2007 following three pilot screening rounds which commenced in 2000. 7 The SBoSP invites all men and women aged 50–74 to participate every two years. Recently, this has been extended to allow those aged over 74 to participate on request. Our objective was to examine, in a fully rolled out national programme, uptake trends over time between 2007 and 2014, the impact of age, sex, and deprivation, and the number needed to screen (NNS) for neoplasia detection.
Methods
Men and women aged 50–74 and registered with a General Practitioner (GP) in Scotland were initially sent a letter advising them that they would receive an invitation to participate in the SBoSP. They were then invited to participate, and each potential participant was sent a guaiac FOBT (gFOBT) kit (hema-screen, Immunostics Inc., New Jersey, USA, supplied by Alpha Laboratories Ltd, Hants, UK) and asked to provide two samples from each of three separate bowel motions. These were deposited on the six oval windows of the gFOBT card, which was then returned in a freepost envelope to the Scottish Bowel Screening Centre for analysis. Test cards were not rehydrated on arrival. Test results were classified as strong positive if five or six of the six windows were positive, and weakly positive if one to four windows were positive. In the case of a weakly positive test result, or a spoiled gFOBT kit, a qualitative faecal immunochemical test (FIT) kit (hema-screen SPECIFIC, Immunostics Inc., New Jersey, USA, supplied by Alpha Laboratories Ltd, Hants, UK), was sent. 13 Following a positive test result, individuals were pre-assessed, either face-to-face or by telephone consultation, by a bowel screening endoscopy nurse and referred for colonoscopy if this was deemed appropriate. If colonoscopy was unsuccessful, further bowel imaging by barium enema or, more recently, CT colonography was carried out.
The study population dataset was assembled by the Information Services Division of NHS National Services Scotland using data extracted from the Scottish Bowel Screening Database. Data on participant age, sex, and postcode were recorded centrally. Deprivation category was calculated using the Scottish Index of Multiple Deprivation 2012 (SIMD), 14 an index of relative deprivation providing a weighted rank for each of seven domains: income (28%), employment (28%), health (14%), education, skills and training (14%), geographical access to facilities (9%), crime (5%), and housing (2%), for the 6505 data-zones in Scotland. Each data-zone represents a small geographical area identified by postcode and containing around 750 people. Using quintiles of deprivation, individuals were assigned to a relative deprivation category based on their postcode at invitation, the first quintile representing the most deprived and the fifth quintile the least deprived.
The positive predictive value (PPV) for detecting CRC was defined as the number of individuals with detected CRC divided by the number undergoing colonoscopy. The PPV for neoplasia was defined as the number of individuals in whom CRC or an adenomatous polyp was identified on histology, divided by the number of individuals undergoing colonoscopy. The NNS was defined as the number of individuals needed to invite to screen to detect one individual with CRC or neoplasia.
Because there was no single intervention during the study period, interrupted time series analyses were deemed inappropriate to assess trends. Further, correlation coefficients determined by simple regression analysis were low and not statistically significant (not shown). Data over time were not linear and simple regression was inappropriate. Consequently, simple visual inspection of graphical of data was performed. Associations between categorical variables were examined using χ2 tests for linear trend unless otherwise specified. A p-value of <0.05 was considered statistically significant. Statistical analysis was performed using SPSS software (SPSS Inc., Chicago, USA).
Results
Numbers and percentages of men and women invited for screening by age and deprivation quintile.
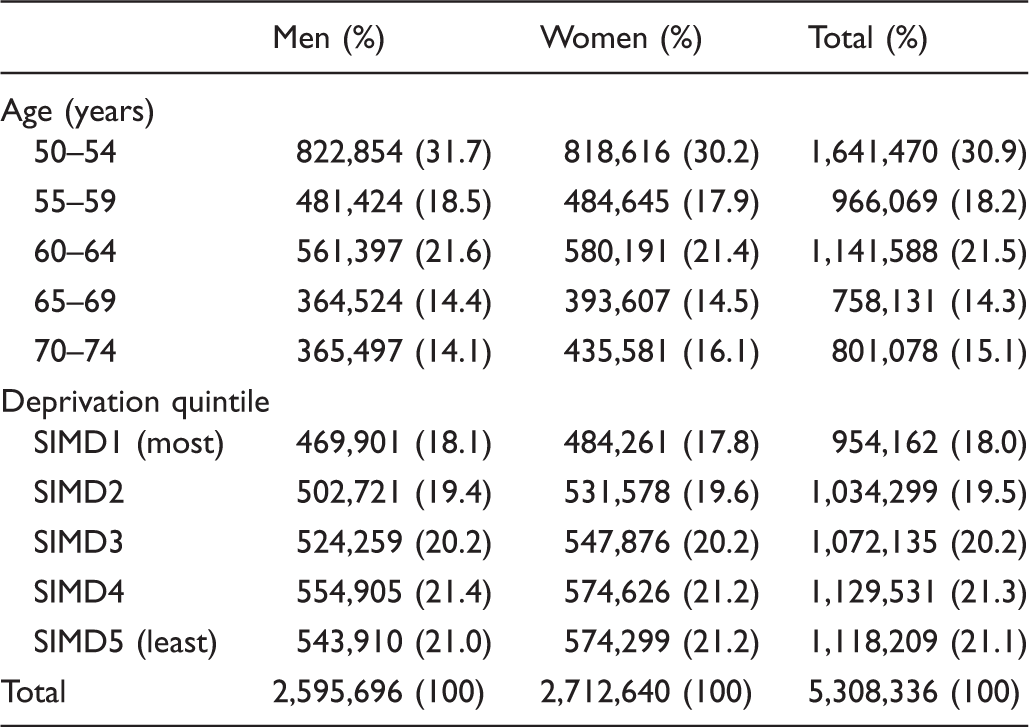
SIMD: Scottish Index of Multiple Deprivation.
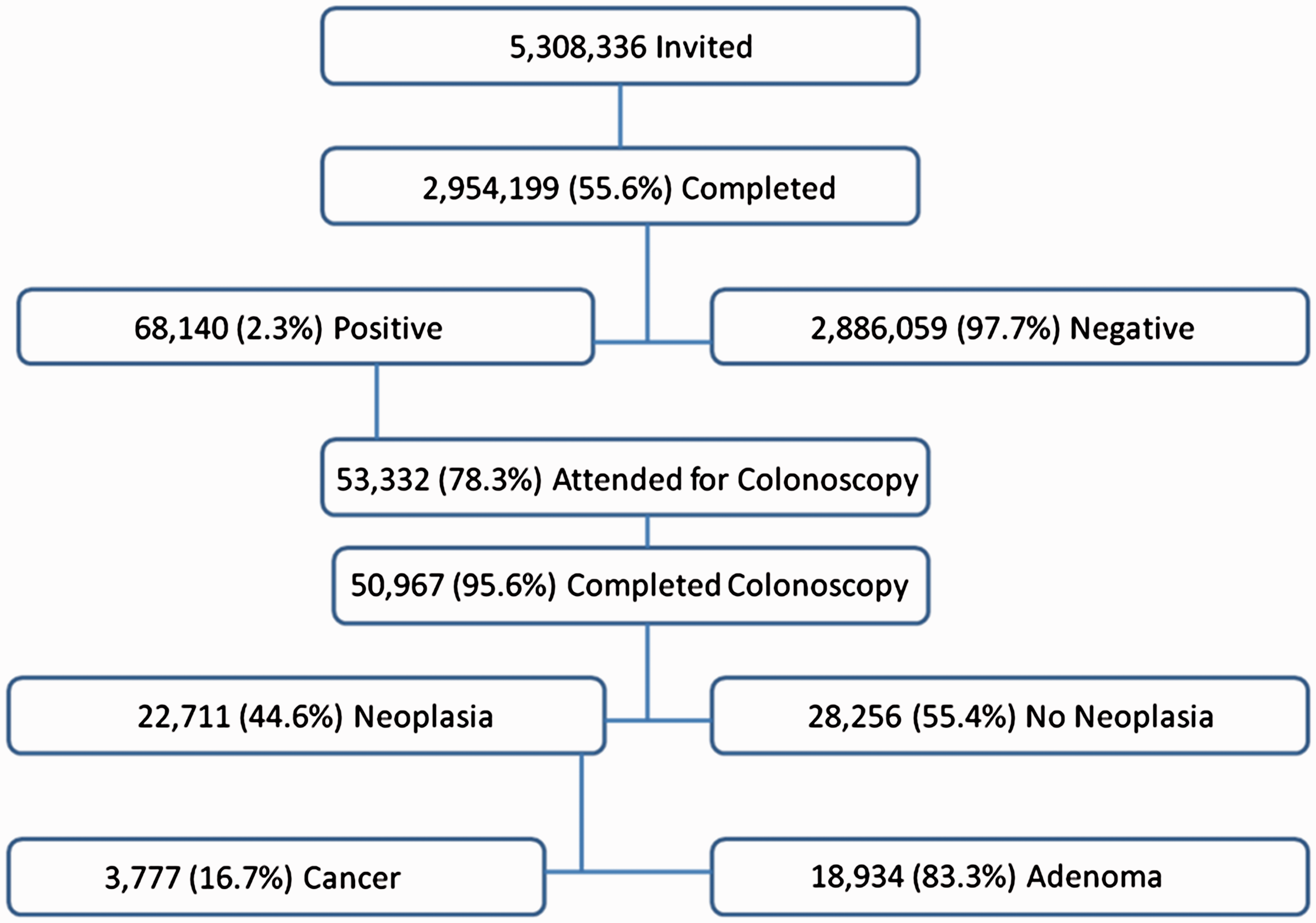
Summary flow diagram of Scottish Bowel Screening Programme 2007–2014.
Numbers and percentages of men and women completing a screening test by age and deprivation quintile.
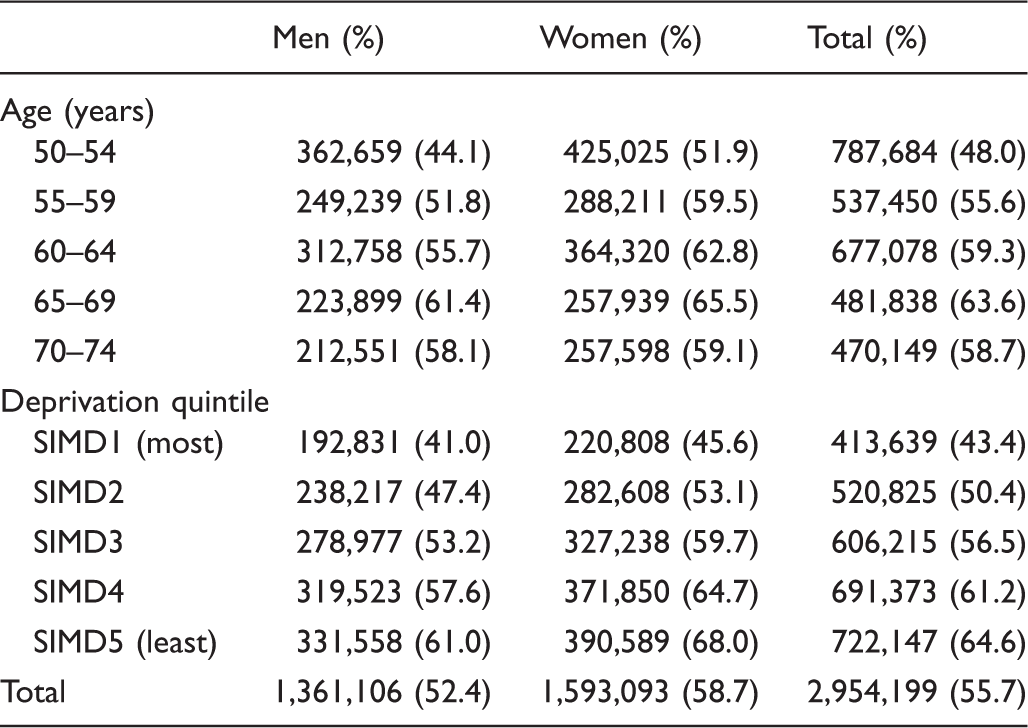
SIMD: Scottish Index of Multiple Deprivation.
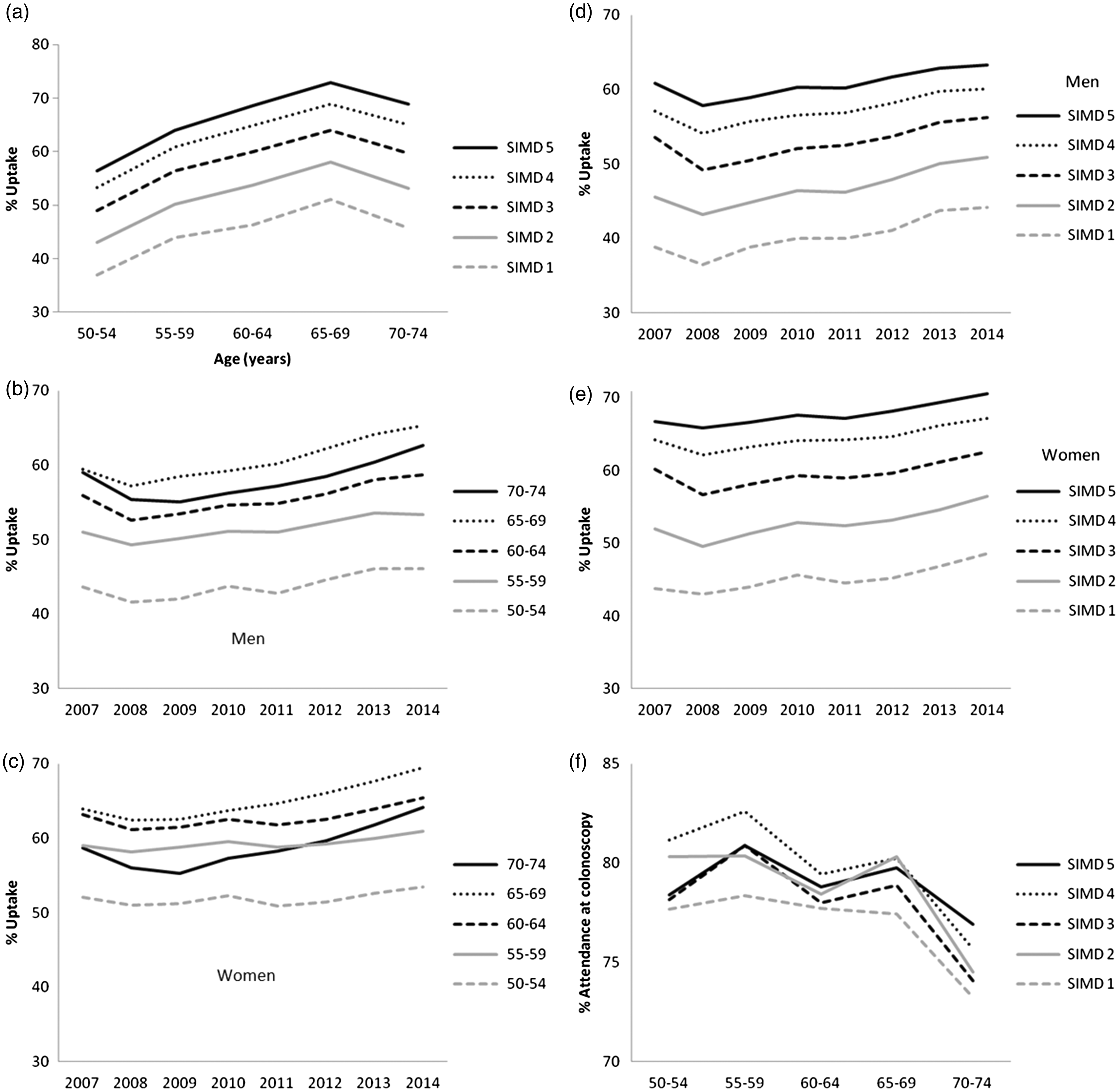
Uptake (%) in the Scottish Bowel Screening Programme by: (a) age and deprivation quintile (SIMD); (b) year and screening age group (years) in men; (c) year and screening age group (years) in women; (d) year by deprivation (SIMD) in men; (e) year by deprivation (SIMD) in women; (f) percentage attendance at colonoscopy after a positive screening test result.
Positivity (%) and positive predictive value (PPV, % with 95% CI) in men and women by age and deprivation category.
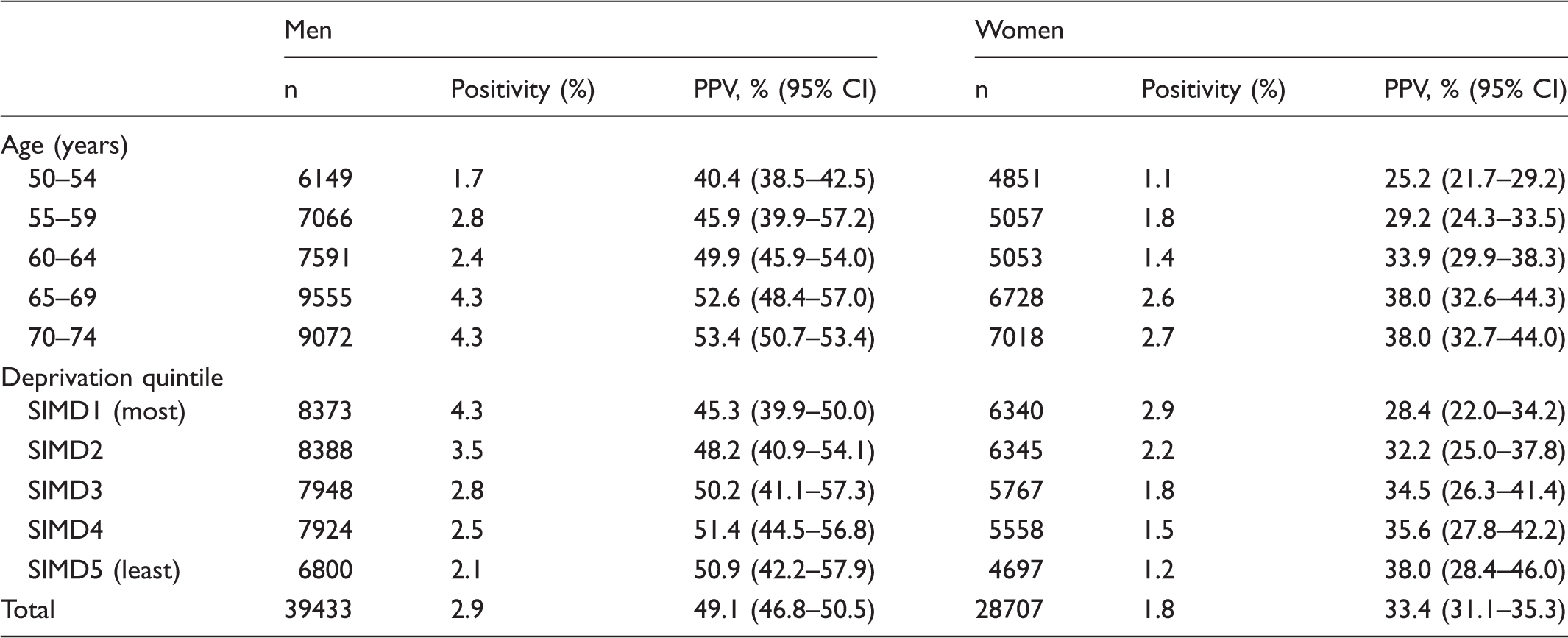
SIMD: Scottish Index of Multiple Deprivation.
Note: Positivity was calculated as the percentage of positive test results in the total number of tests completed. PPV was calculated by adding the percentages of colorectal cancers and adenomas detected in the number of colonoscopies performed.
Detection rates (%) for cancer and adenoma calculated by the number with cancer or adenoma divided by the number who completed the screening test.
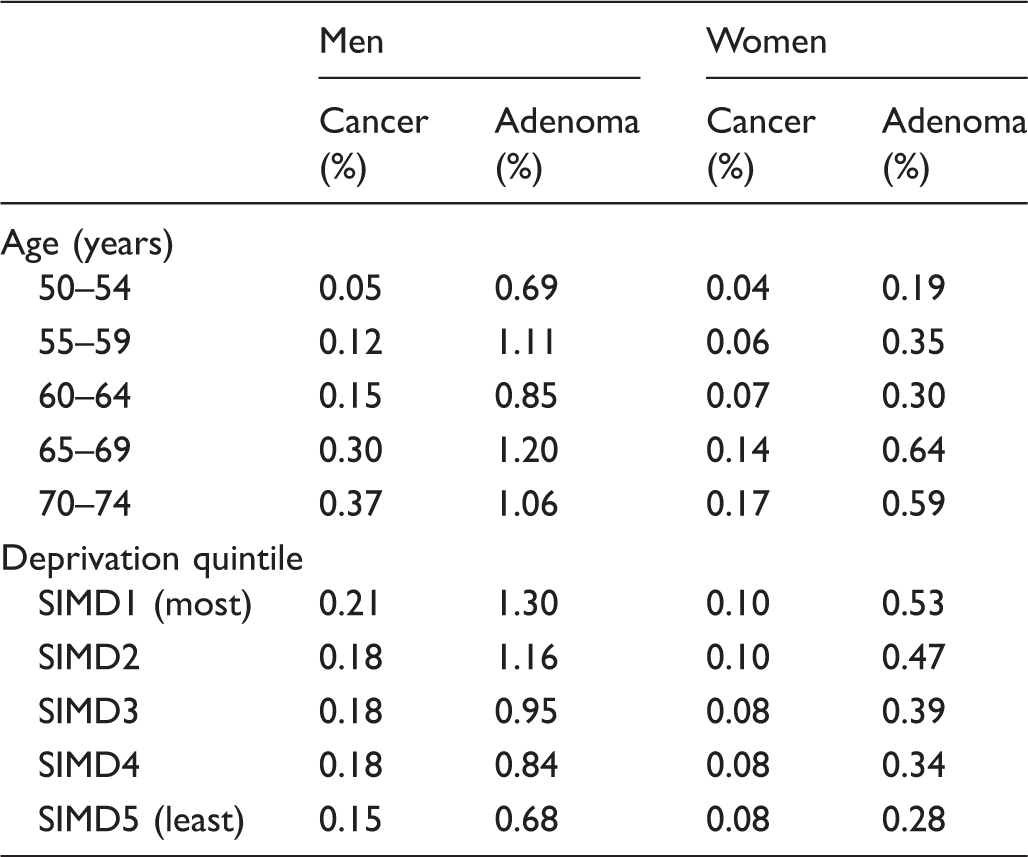
SIMD: Scottish Index of Multiple Deprivation.
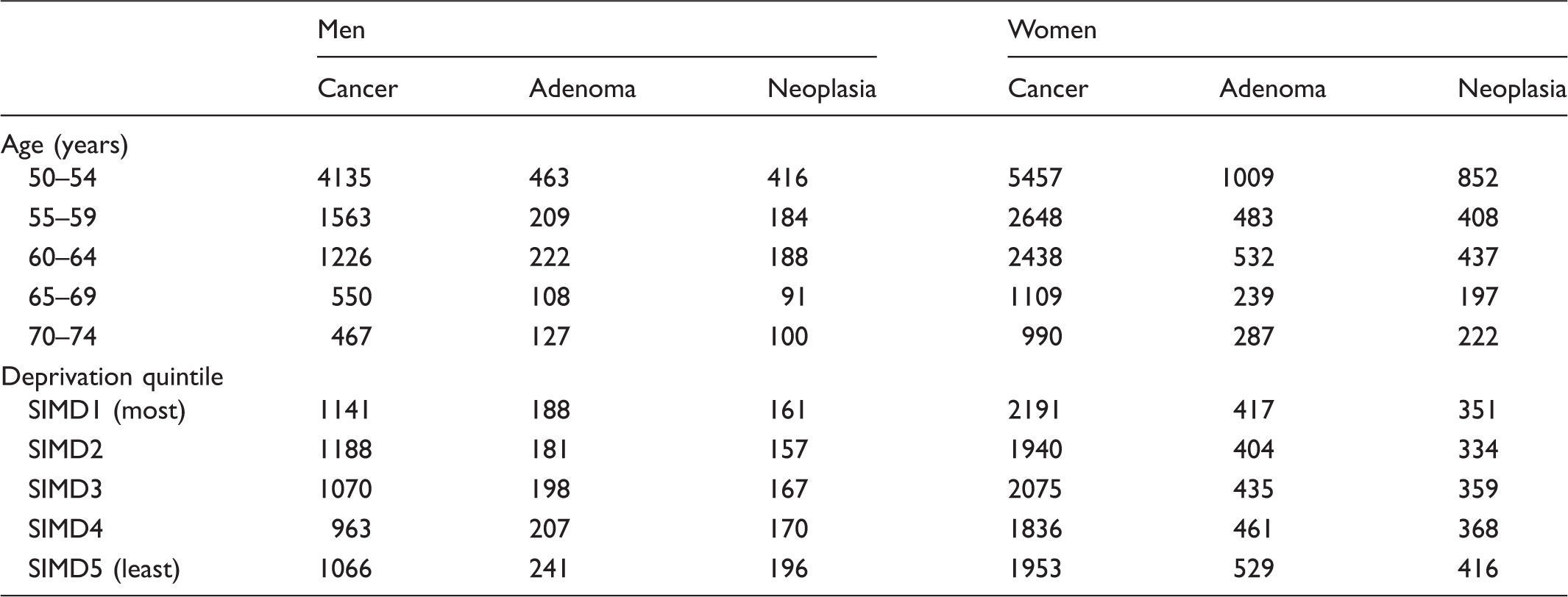
The NNS to detect neoplasia was 234, to detect CRC 1405, and for adenomas 208. The NNS to detect neoplasia fell with increasing age (559 at 50–54 vs. 142 at 70–74), with the steepest gradient evident in the 50–59 age group (Figure 3). The effect of age on NNS was observed in both men and women. Overall, the NNS to detect one case of CRC or adenoma was significantly lower in men than in women (170 vs. 365; p < 0.001), with the largest difference observed in the 50–54 age group (416 vs. 852; p < 0.001). Deprivation had a less marked effect on NNS but was numerically lower in the most deprived groups (Table 5).
Number needed to screen to detect neoplasia (cancer plus adenoma), cancer and adenoma by age group for men and women. Number needed to screen in men and women for cancer, adenoma and neoplasia, calculated by dividing number of participants invited divided by the number of participants with cancer, adenoma or any neoplasia. SIMD: Scottish Index of Multiple Deprivation.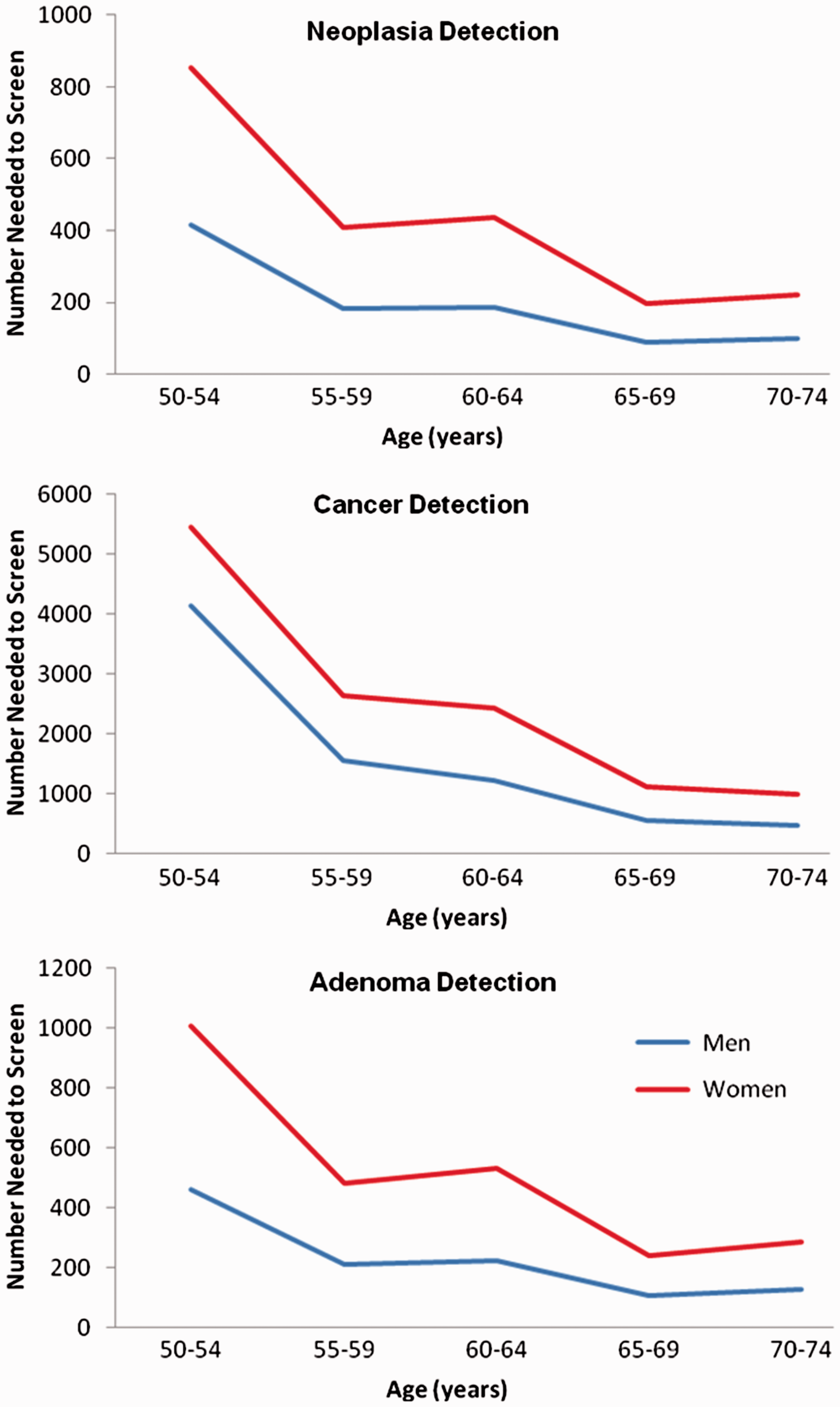
Discussion
This is the first study to report on trends of bowel screening uptake within a fully rolled out national screening programme and to describe the impact of these factors over time. The results show that age, sex, and deprivation have a significant impact on a number of important variables in a population-based CRC screening programme. Men were less likely to respond to the invitation to screening, more likely to have positive FOBT results, and more likely to have CRC detected following a positive test result than women. Furthermore, the more deprived were less likely to respond to the screening invitation, more likely to test positive, less likely to proceed to colonoscopy, and less likely to have CRC or adenoma found at colonoscopy.
These results and those from other studies6,8 demonstrate the impact of age, sex, and deprivation on screening uptake. The observed overall uptake was 55.6%, similar to that obtained in the Scottish and English pilot studies.7,15 Following the national roll-out of screening in Scotland using a two-tier gFOBT/qualitative FIT reflex screening algorithm, overall uptake was 53.2%. During the study period, this overall uptake gradually increased year on year to 58.4%. 13 The trend in uptake is likely to be confounded by the structure of the population invited and re-invited. We and others have demonstrated the benefit of repeat invitations. 16 A slight dip in uptake between 2007 and 2008 was probably due to previously unscreened areas being brought into the SBoSP, adding large numbers of less well-informed, screening naïve people, and increasing numbers living in socio-economically deprived areas.
The upward trends in uptake in the 60–74 age groups in men and women across the deprivation gradient were clear. Assessment of the impact of individual strategies on screening uptake is beyond the scope of this study, but local, regional and national public awareness campaigns, informative leaflets, telephone advice, and face-to-face health promotion may have had positive effects. We observed no such improvement in either men or women in the 50–59 age group. As this group represents nearly half of all invited participants, further research is required to improve this uptake.
Overall, a poorer response to invitations was observed in younger invitees, men, and the more deprived. This effect appeared cumulative; younger men who were most deprived had a 34.4% uptake compared with an uptake of 74.4% in older women who were least deprived. The differences observed in uptake of the screening invitation were largest in the deprived, highlighting the pervasive role of deprivation in determining screening uptake.
Our study supports previous results advocating increasing the upper age range of bowel screening 8 ; however, uptake and CRC detection do not continue to increase with age, but plateau and even decrease in those aged over 70. Plausible reasons for this include difficulty with collection of samples, unwillingness of carers to assist, poor eyesight, and frailty in general. The importance of these trends is unknown as the impact of adenoma detection and removal on CRC mortality in this age group has been questioned.
The adverse effect of deprivation on CRC screening uptake is well documented.6,8,17 The striking decrease in uptake observed in this study with increasing deprivation mirrors the results from the Scottish and English pilot studies and was observed across the whole population.7,14 Our method of measuring deprivation with the SIMD assumes that individuals living in the same area share similar characteristics; however, this approach may disguise considerable ethnic and deprivation variability affecting the perceived benefits of screening.
NNS decreased with increasing deprivation, despite the decrease in both uptake and the PPV of colonoscopy. This reflects the marked increase in positivity and neoplasia detection rates with increasing deprivation. This anomaly makes efforts to increase the proportion of deprived communities that engages in screening all the more worthwhile.
The failure to proceed to colonoscopy following a positive test result is a matter that requires further research. 18 Our results suggest that the effect of age is small and unrelated to sex. Although higher deprivation is associated with lower uptake of colonoscopy, this is not nearly so marked as the effect of deprivation on uptake of the screening test itself. Overall health is a facet of deprivation, and deprived individuals may be less fit to undergo a colonoscopy compared with more affluent individuals. 18 Data regarding the reasons for non-attendance at colonoscopy were not in this study, but our previous work has demonstrated that replacing the routine face-to-face specialist nurse consultation with a choice of telephone interview or face-to-face consultation reduced colonoscopy non-attendance rates from 14.9% to 0.8%. 19
How best to screen the group aged 50–59 remains a contentious issue. In our study, the lowest uptake of screening was observed in this youngest age group; the NNS to detect neoplasia was predictably higher, given the lower incidence of CRC and adenoma. Despite a lower uptake of the test, there is a significant difference in the NNS between men and women of the same age in this group. Within the SBoSP, women aged 50–59 have the lowest FOBT positivity rate, the lowest PPV with the lowest detection of pathology, both CRC and advanced adenomas. These results support conclusions of previous work.20–22 A Polish study found a higher incidence of advanced neoplasia in men than in women, and the NNS for men aged 50–54 was similar to that for women aged 60–66 years. 21 In a US study using population-based cancer registry data, 10-year cumulative CRC incidence rates among men aged 50, 55, and 60 were found to be similar to rates among women four to six years older. 22 In addition, at the 30-year follow-up of the Minnesota CRC screening trial, no cancer-specific survival benefit was observed in women aged under 60 at the time of screening. 20 This conclusion is supported by other evidence from the SBoSP that concluded that women are disadvantaged in bowel screening programmes that use FOBT, both because they are at a higher risk of right-sided cancers, which are less likely to generate a positive test result, and because they are inherently less likely to have a positive test result with CRC at any site. The authors calculated that only about one-third of cancers were detected by screening in 50–59-year-old women who participated. 23 Further research is required regarding the benefits and how best to screen women aged below 60. A quarter of all invitations and 45% of completed tests are in women aged 50–59. In the absence of any proven benefit, this represents an area where a more tailored approach may be appropriate.
Although this study used a prospectively maintained database, it has a number of limitations. Firstly, the proportion of individuals in the study who had previously undergone colonoscopy or other lower gastrointestinal investigation is unknown. This may have affected both an individual’s attitude towards engaging in the screening process and the likelihood of finding significant pathology at colonoscopy. Further, this study was not able to assess reasons for non-participation, or outcomes in those who chose not to participate, although CRC mortality is lower in those who participate than those who do not.24–28 In addition, a positive test result in this study actually represents possible outcomes from three separate screening pathways; strong positive gFOBT, positive FIT following a weak positive gFOBT, or a positive FIT following a spoiled gFOBT. National data on the type of positive test result of the participants (either gFOBT or FIT) or compliance with FIT in those who had weak positive test results on initial gFOBT were unavailable and therefore not included in our analysis. Data from NHS Tayside have shown similar overall neoplasia detection rates by both strong positive gFOBT and positive FIT following a weak positive gFOBT. 13
Conclusions
Our results demonstrate wide variations in CRC screening uptake and outcomes associated with age, sex, and deprivation. They also demonstrate increasing uptake with time across age and deprivation gradients in both sexes. Further work is required to improve uptake in those from deprived communities and in those aged 50–59. Our data reinforce the need for questioning the strategies and benefits of screening women aged 50–59.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.