
Abstract
Objective
To evaluate the association between human papillomavirus vaccination status and participation in cervical cancer screening (at age 25) by the first cohorts of girls who were offered vaccination at the age of 15 to 16 years in Italy.
Methods
Women born in 1993, 1994 and 1995 were invited to participate in cervical cancer screening between 2018 and 2020. We report participation in screening by vaccination status in three large areas, Florence province, Piedmont region and Savona province, where the Consensus Project was carried out. The relative risk of participation among vaccinated (≥2 doses) and unvaccinated women was estimated. Odds ratios (OR) of participation by vaccination status were estimated by logistic regression, adjusted by birthplace and birth cohort.
Results
Overall, 34,993 women were invited for screening: 13,006 (37.2%) participated and 10,062 of these agreed to participate in the Consensus intervention study. Among the invited women and screening participants, vaccinated women were 51.0% and 60.6%, respectively. Comparing vaccinated and unvaccinated women, the adjusted OR of screening participation was 1.80 (95% confidence interval (CI): 1.72–1.89), 2.17 (95% CI: 1.94–2.42), 1.59 (95% CI: 1.50–1.68) and 1.15 (95% CI: 0.86–1.54) for overall, Florence, Piedmont and Savona, respectively. About 33% of the invited women were unvaccinated and did not participate in screening: 25.8%, 59.5% and 64.2% of women born in Italy, in high migration pressure countries and in advanced development countries, respectively.
Conclusions
Screening participation was higher among vaccinated than unvaccinated women. Active policies are needed to reduce inequalities, targeting the unscreened and unvaccinated population, particularly non-native women, to accelerate cervical cancer elimination in Italy.
Keywords
Introduction
In Italy, in 2007 to 2008, the National Human Papilloma Virus (HPV) Vaccination Programme introduced free vaccines for 12-year-old girls. 1 In 2008, 5 regions (Valle d’Aosta, Piedmont, Friuli-Venezia Giulia, Basilicata and Tuscany) initiated free, multi-cohort, HPV vaccination campaigns targeting also 15–16-year-old girls (born in 1993, 1994 and 1995). 2 The first available vaccines were the bivalent (HPV 16, 18) and the quadrivalent (HPV 6, 11, 16, 18). 3 In 2017, the nonavalent vaccine (HPV 6, 11, 16, 18, 31, 33, 45, 52, 58) became available in Italy to both sexes. 4
The introduction of HPV vaccination programmes has had a substantial impact on the incidence of HPV infections and preneoplastic lesions of the cervix in almost all countries in which it has been assessed. 5 An Italian study 6 within organised screening (mean age 27.5 years) reported a significantly lower adjusted odds ratio (OR) of abnormal cytology in unvaccinated than in vaccinated women (OR: 0.52; 95% confidence interval (CI): 0.34–0.79). Another Italian study 7 showed a significantly higher prevalence of HPV 6, 11, 16, and 18 in unvaccinated than in vaccinated women (5.5% vs 0.6%, p < 0.001) in the 18 to 24 age group. This new epidemiological situation calls for a reorganisation of cervical cancer screening programmes for girls vaccinated at 11 to 12 years who reach the age of onset of screening (25 years in Italy). It would be an inefficient allocation of resources if the same screening protocol (screening test, age of onset of screening and screening interval) were applied for both vaccinated and unvaccinated women. Therefore, the goals of the Consensus Conference for cervical cancer screening of vaccinated women, held in Florence in 2015 and sponsored by the Italian Ministry of Health, were to define the best screening policies for vaccinated and unvaccinated girls, and to identify actions to implement evidence-based screening strategies.8,9
The Consensus Project was set up to assess the feasibility of and prepare for the implementation of the conference's recommendations for cervical cancer screening. 10 The project has involved 5 regions: 3 of them (Piedmont, Liguria and Tuscany) have introduced a multi-cohort vaccination programme that includes 15–16-year-old girls, and 2 of them (Emilia-Romagna and Veneto) have only implemented opportunistic vaccination for these birth cohorts. 11 Supplemental File S1 reports the project goals and protocol of the Consensus Intervention Study.
The aim of this study was to evaluate the association between HPV vaccination status and participation in the first round of cervical cancer screening (at age 25) for the first cohorts of 15–16-year-old girls offered HPV vaccination.
Methods
Setting
In Italy, organised screening programmes for cervical cancer actively invite all resident women aged 25 to 64 years. HPV vaccination and cervical cancer screening policies are described in Table 1.12,13 In 2020 to 2021, whether on their own initiative (30.9%) or through organised programmes (39.5%), 71.4% of women aged 25 to 34 years underwent cervical screening. 14 The reported mean age at sexual debut for females was 15.7 ± 1.6 in a survey 15 of representative samples of students from 5 Italian cities carried out between 2008 and 2011.
Summary of HPV vaccination and cervical cancer screening policy implemented in Italy.
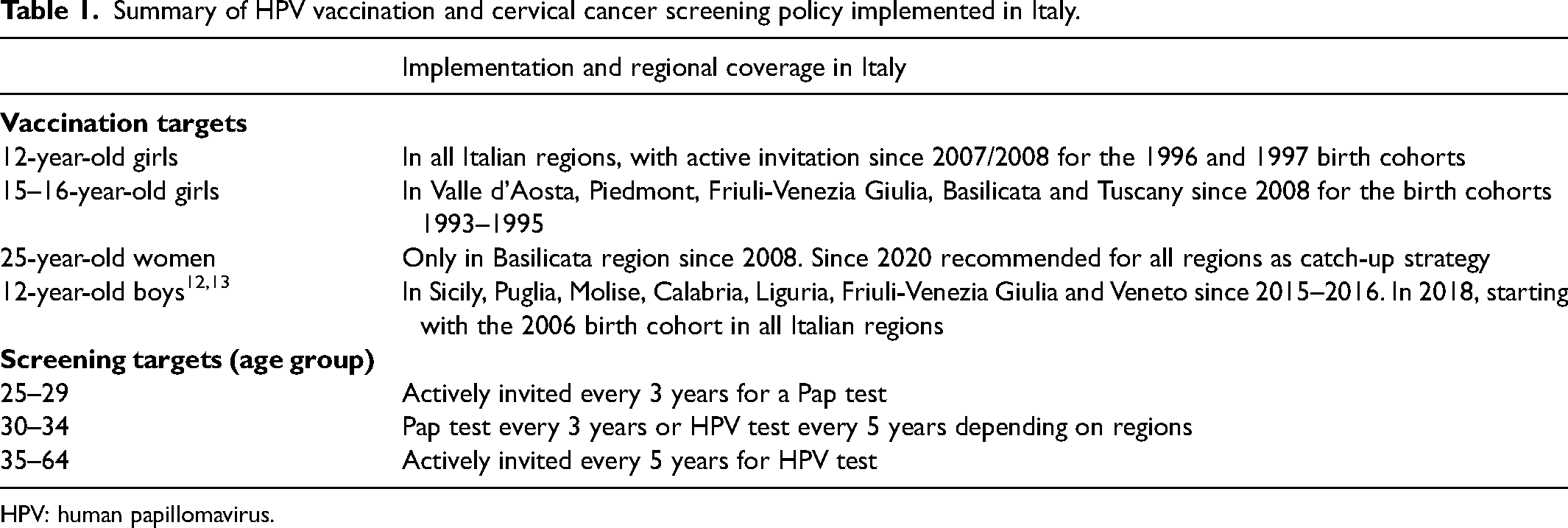
HPV: human papillomavirus.
The Consensus Intervention Study design
The Consensus Intervention Study is a single-arm, multi-centre, prospective, intervention study, nested in the organised screening programmes. The study protocol is reported in Supplemental File S1. A further analysis of real-world HPV vaccine effectiveness will be the subject of upcoming papers.
Study population
The study population consisted of 25-year-old women (born in 1993, 1994 and 1995) at their first round of cervical cancer screening and residing in regions where on-call HPV vaccination programmes for girls aged 15 to 16 years (multi-cohort strategy) were implemented from 2008 to 2010. Three screening programmes met these conditions: Florence (Tuscany region), Savona (Liguria region) and the Piedmont region. Invitations started in November 2018 and ended in September 2020. However, the invitation periods differed among centres. Florence and Piedmont invited women of the 1993, 1994 and 1995 birth cohorts in the years 2018, 2019 and in the first quarter of 2020. Currently, Savona, contrary to the national guidelines, is not inviting women aged 25 to 29 years. For the study, this screening centre specifically invited women who were born between 1994 and 1995 and would turn 25 between January and March 2020. It was possible to send a routine screening reminder letter only for the 1993 and 1994 birth cohorts in the Florence and Piedmont programmes. All women received information on the study along with the screening invitation letter, as well as additional information from midwives when the screening tests were performed. The women who agreed to participate in the intervention study were asked to sign an informed consent form and were tested for HPV, while the other participants underwent a Pap test. Screening programmes were suspended by all centres in March 2020, during the national lockdown due to the Sars-CoV2 pandemic. In June 2020, Florence and Piedmont managed to recall the previously invited women whose screening had been suspended. A further recovery of invitations continued until September 2020 in Piedmont.
Linkage between vaccination and screening databases
The vaccination status of the study population was established through a record linkage between the Local Health Unit (LHU) registry and the screening archive. The Piedmont and Florence centres adopted different strategies to assess the completeness of the HPV vaccination information in the LHU registry (see Supplemental File S2).
Definitions of vaccinated women and place of birth
Women with at least two doses of vaccine in LHU vaccination registries were considered vaccinated. In the period 2008 to 2010, the full vaccination schedule was three doses. However, we considered two doses to be an effective vaccination schedule when the first dose was given at or before 18 years of age, according to Markowitz et al. 16
The birthplace of invited women was categorised as follows: Italy; countries with high migration pressure (HMP) which covers central and eastern Europe; south-central America; north and sub-Saharan Africa and Asia (except Israel and Japan); and high-income or advanced development (AD) countries.
Ethical approval
The project was approved by the Regional Ethics Committee for Clinical Trials of the Tuscany Region (registration number: 11932_spe).
Statistical analysis
The proportion of invited women who participated in screening whether by HPV or Pap test was calculated for each birth cohort, screening centre and place of birth and, in a similar fashion, the proportion of those screened who participated in the intervention study.
We present the relative risk (RR) of participation in the screening programme having been invited to screening and of participation in the intervention study having been screened, for vaccinated versus unvaccinated women. ORs of screening participation and of intervention study participation by vaccination status were estimated using a logistic regression model adjusted by place and cohort of birth. The unadjusted proportion of women participating in screening after invitation according to vaccination status was calculated for the 1993 and 1994 birth cohorts of Florence and Piedmont.
The analysis of variance and chi-square tests were used where appropriate. A p-value of <0.05 was considered significant. Statistical analyses were performed using Stata, version 16.0 (StataCorp LP, College Station, TX, USA).
Results
Overall, 34,993 women were invited to their first cervical cancer screening: 7679 in Florence, 26,088 in Piedmont and 1226 in Savona. Of these women, a total of 13,006 (37.2%) underwent screening. The overall mean age of screening participants was 25.6 years (SD: 0.63).
The bivalent vaccine was prevalent (73.0%): 97.1% (2581 of 2659) in Florence, 81.4% (79 of 97) in Savona and 60.4% (3096 of 5124) in Piedmont. The mean age at the first vaccine dose for screening participants differed significantly (p < 0.01) among centres: 15.1 (SD: 0.97) in Florence (44.6% < 15 years), 15.4 (SD: 2.07) in Savona (46.9% < 15 years) and 15.8 (SD: 0.85) in Piedmont (1.5% < 15 years). According to the number of HPV vaccine doses recorded in the LHU vaccination registries, 724 (3.9%) invited women received one dose, 794 (4.3%) two doses and 17,067 (91.8%) three doses.
Table 2 shows HPV vaccination coverage (≥ 2 doses) of birth cohorts 1993, 1994 and 1995 among women invited for screening, screening participants after invitation and participants in the intervention study. HPV-vaccinated women represented 51.0% of the invited women, 60.6% of screening participants and 63.1% of intervention study participants. The proportion of vaccinated women increases by birth cohort (from 1993 to 1995). The proportion of women who were vaccinated and born in Italy was two to three times higher than that of women born in HMP countries. Screening participation increased significantly (p < 0.01) with the number of vaccine doses: 30.5% (221 of 724), 38.8% (308 of 794) and 44.4% (7575 of 17,067) for 1, 2 and 3 doses, respectively.
HPV vaccination coverage (≥ 2 doses) of birth cohorts 1993–1995 by centre and country of birth among women invited for screening, screening participants after invitation and participants in the intervention study.
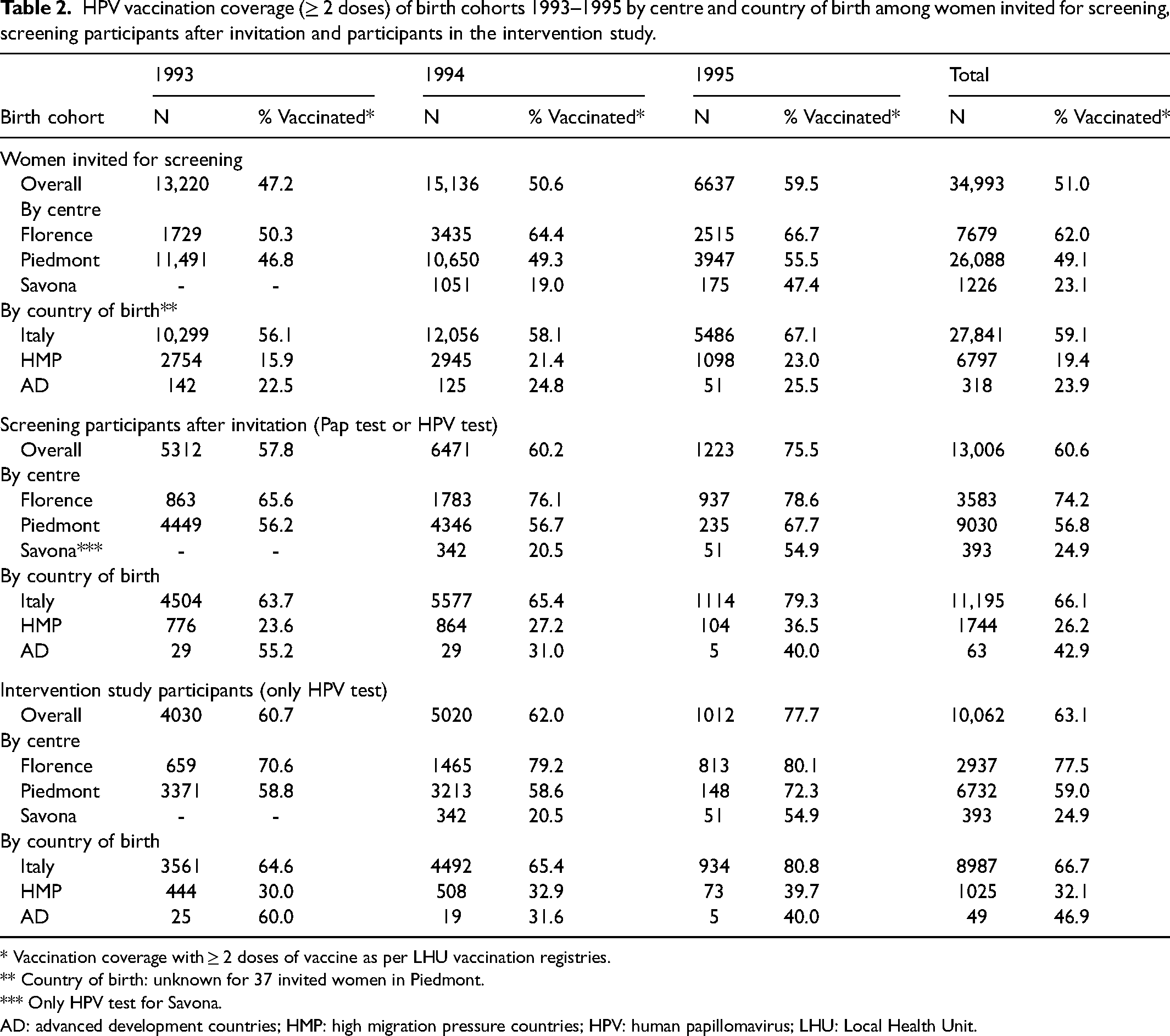
* Vaccination coverage with ≥ 2 doses of vaccine as per LHU vaccination registries.
** Country of birth: unknown for 37 invited women in Piedmont.
*** Only HPV test for Savona.
AD: advanced development countries; HMP: high migration pressure countries; HPV: human papillomavirus; LHU: Local Health Unit.
The RRs are shown in Table 3. Overall, the RR of screening participation was 48% (RR: 1.48, 95% confidence interval (CI): 1.44–1.52) higher among vaccinated compared to unvaccinated women. In Florence, vaccinated women were 76% more likely to participate in screening than unvaccinated women, while that excess was reduced to 36% in Piedmont. In terms of country of birth, women born in HMP and AD countries were 36% (25.7 of 40.2 = 0.64, 95% CI: 0.61–0.67) and 51% (19.8 of 40.2 = 0.49, 95% CI: 0.40–0.62) less likely to participate in screening after invitation, respectively, than women born in Italy. Vaccinated women born in AD countries were 2.4 times more likely to participate in screening than unvaccinated women, while the excess was 47% for women born in HMP countries. Vaccinated women also showed a slightly higher probability of participating in the intervention study than unvaccinated women, once participating in screening.
RR of participating in screening after invitation and participating in the intervention study among all screening participants of vaccinated versus unvaccinated women by centre and country of birth.
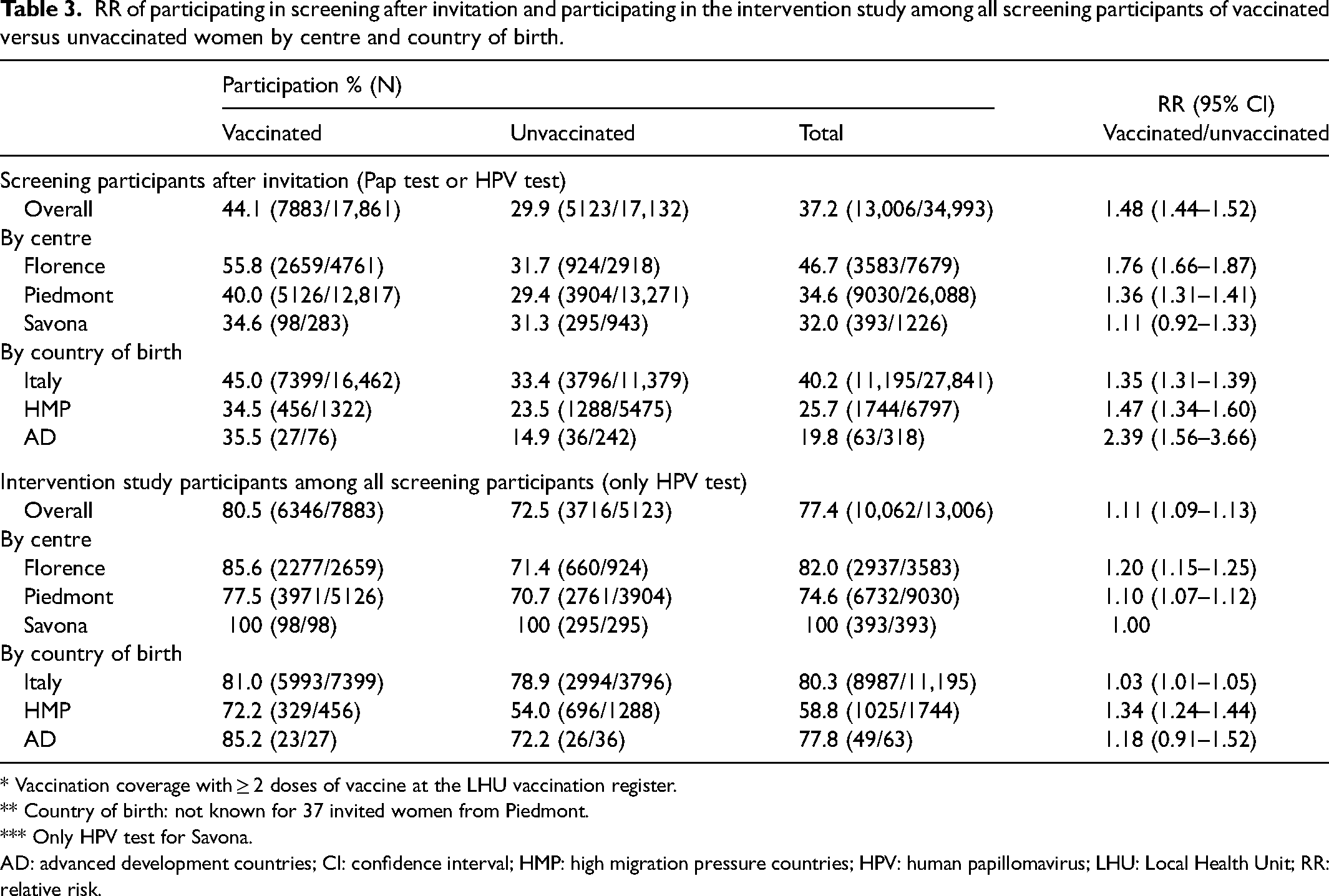
* Vaccination coverage with ≥ 2 doses of vaccine at the LHU vaccination register.
** Country of birth: not known for 37 invited women from Piedmont.
*** Only HPV test for Savona.
AD: advanced development countries; CI: confidence interval; HMP: high migration pressure countries; HPV: human papillomavirus; LHU: Local Health Unit; RR: relative risk.
In evaluating participation by birth cohort, the restrictions imposed because of the COVID-19 pandemic in 2020 should be considered: <20% (1223 of 6637 = 18.4%) of the 1995 birth cohort invited in 2020 participated in the screening, while this was over 40% (6471 of 15,136 = 42.7%) for the 1994 birth cohort invited in 2019. This situation was important for the Piedmont centre where a large number of invitations were sent just before the suspension of screening in 2020.
The higher participation in vaccinated women was appreciable also when adjusting for cohort and country of birth category (OR: 1.80, 95% CI: 1.72–1.89) (Table 4).
OR of screening participation after invitation in vaccinated versus unvaccinated women, adjusted by country and birth cohort.
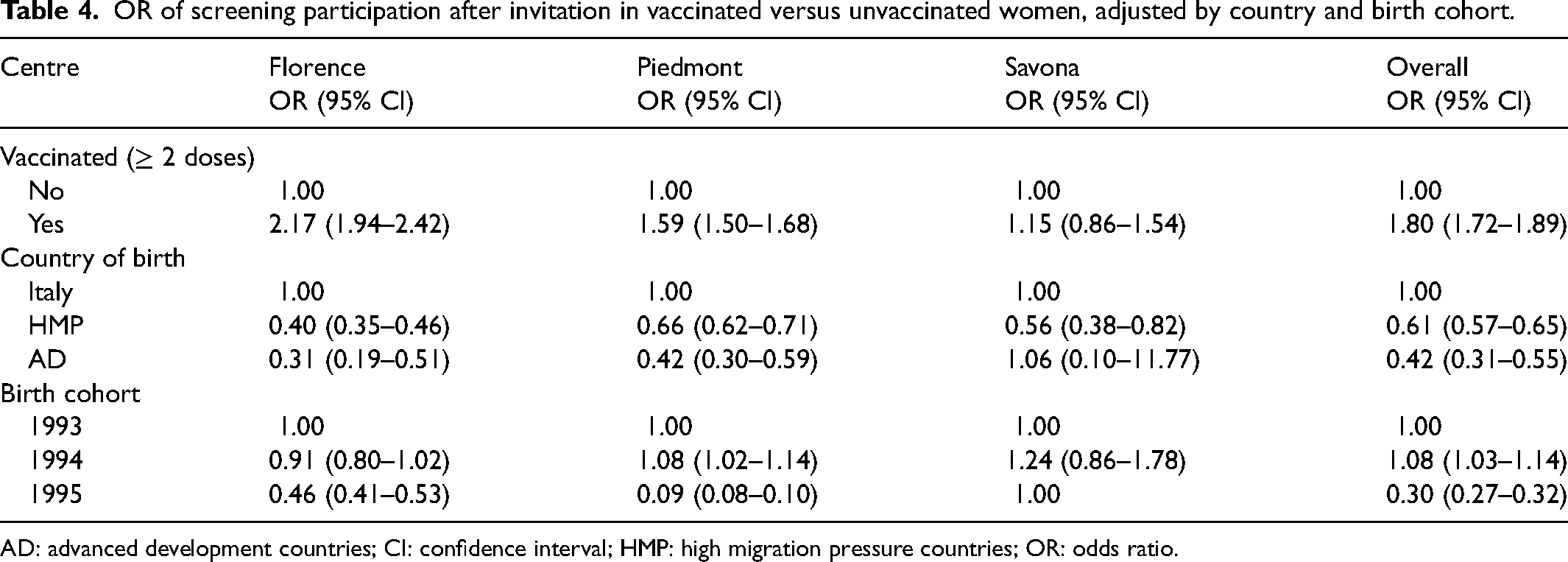
AD: advanced development countries; CI: confidence interval; HMP: high migration pressure countries; OR: odds ratio.
Table 5 shows the unadjusted proportion of women participating in screening after invitation according to vaccination status, considering only the 1993 and 1994 birth cohorts for Florence and Piedmont (27,305 invited women). The proportion of vaccinated and screened women (maximum protection) was 25.2%, whereas the proportion of unvaccinated and unscreened women (unprotected) was 33.1%. The proportion of women with maximum protection declines from 30% (Italian-born women) to 9.4% (women born in AD countries) and 7.5% (women born in HMP countries), while the proportion of completely unprotected women rises from 25.8% (Italian-born women) to 59.5% (women born in HMP countries) and 64.2% (women born in AD countries).
Unadjusted proportion of screening participation after invitation (screened/unscreened) according to vaccination status (vaccinated/unvaccinated) for the 1993 and 1994 birth cohorts of Florence and Piedmont, overall and by country of birth.
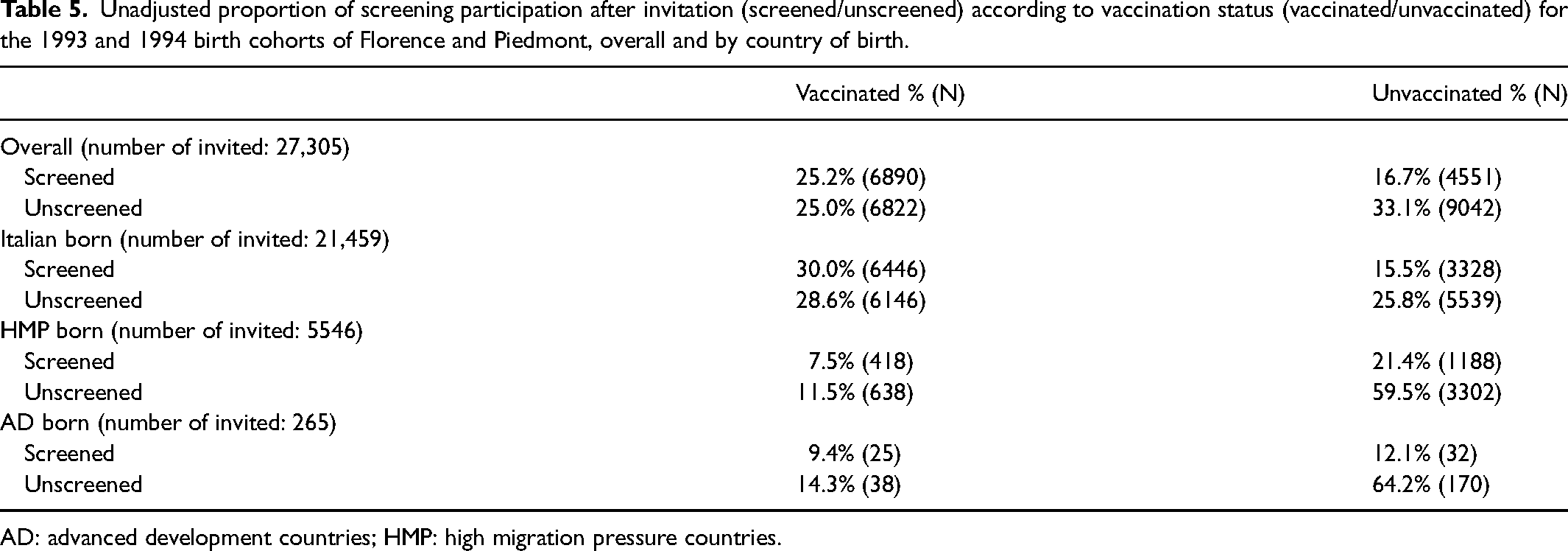
AD: advanced development countries; HMP: high migration pressure countries.
Discussion
This study found a positive association between HPV vaccination and screening participation in the first cohorts of girls offered HPV vaccination at age 15 to 16 years at their first invitation to cervical cancer screening (aged 25) in organised Italian screening programmes. Screening participation among vaccinated women (44.1%) was higher than among unvaccinated women (29.9%). The proportion of unvaccinated and unscreened women was 33%. This proportion increases to about 60% in immigrant women.
The results of our study are consistent with previous studies in young women.17–19 In a Canadian study 17 the age-adjusted screening participation (aged 18 to 21) was 13.0% for vaccinated versus 11.4% for unvaccinated women (vaccination coverage at least 2 doses: 40.8%). In a Danish study, 20 the screening participation (aged 23) was 61.4% for vaccinated women versus 39.0% for unvaccinated women (vaccination coverage at least 1 dose: 91.2%). In a large American study, 21 screening participation among privately insured women (aged 21–26) was 34% higher in vaccinated (at least 1 dose) than in unvaccinated women. A study 22 in Scotland, reported a risk ratio of 0.59 for the participation of unvaccinated women compared to vaccinated women with 3 doses. The adjusted OR of participation for unvaccinated versus vaccinated women in Wales (aged 20) was 0.58 (95% CI: 0.55–0.61). 23 The screening participation in Japan (aged 20–21) was 6.2% for vaccinated and 3.1% for unvaccinated women. 24 In 2013 to 2014, the Australian Institute of Health and Welfare (IHW) reported higher screening participation at age 25 years for vaccinated (54.0%) than for unvaccinated women (39.3%). 25 The positive association between HPV vaccination and participation in cervical screening programmes was also found for opportunistically vaccinated young women in Italy, 11 Switzerland 26 and Sweden, 27 a selected population potentially more motivated to join the screening programme. Only a few previous studies have found lower compliance among vaccinated compared to unvaccinated women, for example Budd et al., 28 in Australia, in women aged 20 to 29 years (later recognised as incorrect due to data linkage issues), 25 and Garrido et al., 29 in the United States, in women aged 21 to 29 years.
Some studies have also shown that participation in screening programmes increased with increasing number of vaccine doses received21,22,25 (a dose–response relationship), further supporting the association between HPV vaccination and screening. Our study confirms this trend: 30.5%, 38.8% and 44.4% for 1, 2 and 3 doses, respectively.
Based on our results and considering only the screening rounds of the 1993 and 1994 cohorts from Florence and Piedmont, 33.1% of the invited population may be considered at high risk for cervical cancer having been neither vaccinated nor screened. Beer et al., 23 in the United Kingdom, reported a similar result (31.6%), but in women from socially deprived areas. Badre-Esfahani et al., 20 in Denmark, found only 5.4% of women in this situation, but the population had a very high childhood vaccination coverage (91%), thus only a small number of unvaccinated women remain who may also be unscreened women. In evaluating these data, it should be considered that screening participation is related only to one screening session at age 25 years and only within organised screening. It is well known that young women have lower screening participation rates30–32 and that participation increases with age. In Italy, a large part of test coverage does not take place through organised programmes (Progressi delle Aziende Sanitarie per la Salute in Italia (PASSI) 14 surveillance system participation 25–34 years: 39.5% in organised screening and 30.9% in spontaneous screening). Furthermore, women both unvaccinated and unscreened might in some way benefit from a herd immunity effect. Evidence of herd protection against high-grade cervical disease was found in unvaccinated girls in Scotland. 33 This result was also confirmed by a recent systematic review. 5
In our study, the situation is particularly worrisome: the proportion of non-native women who are both unvaccinated and unscreened (HMP born: 59.5%, AD born: 64.2%) is more than double that of native women (25.8%). The vaccination of girls at 15 to 16 years was a parental choice and may have been influenced by parental attitudes and education. The Australian IHW report 25 suggests that vaccinated women may have greater awareness of cervical screening and healthier behaviours. A Danish study 20 suggested that the barriers to participation and vaccination may be different between natives and non-natives and that they may require different approaches. The main barriers to vaccination and screening among migrant women in Europe, 34 that is, language difficulties, lack of knowledge about cervical cancer risk factors and difficulties in navigating the health system, are probably the same. Furthermore, for women born abroad, having a vaccination recorded in LHU archives 35 is associated with a long-term stable residence in the study area, which is also associated with participation in screening, through several intermediate determinants: sending the invitation to a valid address, not having screening performed in the home country, and being familiar with and trusting in the Italian health system. Therefore, the association between non-vaccination and non-participation in screening would be stronger in immigrant women. In particular, in our study, the figure is expected for the small group of AD-born women who moved mostly for study and have still strong links with their home countries.
The low vaccination coverage (51%) of invited women reported in this study suggests that to accelerate cervical cancer elimination in Italy it will be necessary to implement active catch-up policies, targeting both the women who do and who do not participate in the first screening round, as already recommended by the National Immunization Plan. 13 Furthermore, actions are needed to reduce inequalities between non-native and native women. Previous studies36,37 in Italy have already described a lower cervical cancer screening participation rate among immigrant women, who are also at greater risk for cervical pathological findings compared to Italian women, although this low coverage tends to change as the length of stay in Italy increases (PASSI 14 ). Finally, it is worth noting that, because of the active invitation and communication campaigns that were put in place through the most widespread school channels, vaccination at age 11 to 12 years attained a higher coverage (60% national average) 35 and much lower socio-demographic inequalities than the catch-up campaigns targeting the 15-year-old girls included in this study. 38
Study strengths and limitations
This is the first analysis of participation within organised cervical cancer screening programmes of a large cohort of girls who were offered the HPV vaccine at age 15 to 16 years.
This study has some limitations. Firstly, it includes only three regions from north-central Italy, even though other regions (such as Valle d’Aosta, Friuli-Venezia Giulia and Basilicata) have actively offered HPV vaccines to 15–16-year-old girls. Secondly, vaccination status may be underestimated for several reasons: (1) only women with at least two HPV vaccine doses according to LHU registries were considered vaccinated, while women with only one dose were considered unvaccinated (724 (3.9%) out of 34,993 invited women) despite it having been demonstrated that a single-dose vaccination at age 10 to 18 years 39 has a long-lasting efficacy against persistent HPV infection; (2) the reconstruction of vaccine status depends on the extent of the geographical coverage of the LHU vaccination archive, especially in light of residential mobility due to work or study, indicating that a national vaccination register is needed; (3) some vaccinations may have slipped in the record linkage between vaccination and screening registers or might not have been recorded in the vaccination register; and (4) vaccinated women in their home country were not on the vaccination register.
Conclusions
Screening participation at first invitation among vaccinated women was higher than among unvaccinated women. Active policies are needed to reduce inequalities, targeting the unscreened and unvaccinated, and particularly non-native women in order to accelerate the elimination of cervical cancer in Italy.
Supplemental Material
sj-doc-1-msc-10.1177_09691413231165237 - Supplemental material for The Consensus Project: Participation in cervical cancer screening by the first cohorts of girls offered HPV vaccination at age 15–16 years in Italy
Supplemental material, sj-doc-1-msc-10.1177_09691413231165237 for The Consensus Project: Participation in cervical cancer screening by the first cohorts of girls offered HPV vaccination at age 15–16 years in Italy by Carmen B Visioli, Paolo Giorgi Rossi, Paola Armaroli, Anna Iossa, Raffaella Rizzolo, Luigina A Bonelli, Ezio Venturino, Francesca M Carozzi, Simonetta Bisanzi, Laura De Marco, Livia Giordano, Elisa Camussi, Annarosa Del Mistro, and Marco Zappa in Journal of Medical Screening
Supplemental Material
sj-doc-2-msc-10.1177_09691413231165237 - Supplemental material for The Consensus Project: Participation in cervical cancer screening by the first cohorts of girls offered HPV vaccination at age 15–16 years in Italy
Supplemental material, sj-doc-2-msc-10.1177_09691413231165237 for The Consensus Project: Participation in cervical cancer screening by the first cohorts of girls offered HPV vaccination at age 15–16 years in Italy by Carmen B Visioli, Paolo Giorgi Rossi, Paola Armaroli, Anna Iossa, Raffaella Rizzolo, Luigina A Bonelli, Ezio Venturino, Francesca M Carozzi, Simonetta Bisanzi, Laura De Marco, Livia Giordano, Elisa Camussi, Annarosa Del Mistro, and Marco Zappa in Journal of Medical Screening
Footnotes
Acknowledgements
We would like to thank Guglielmo Ronco, who made a critical contribution to the design of The Consensus Study project; Silvia Franceschi, for analysis suggestions; Elena Biffoli and Manola Turci, ISPRO Research Support Activities, for technical support throughout the study period. Many thanks to The Consensus Working Group: Florence centre – Paola Mantellini, Carmelina Di Pierro, Carolina Filomena, Noemi Auzzi, Lisa Lelli, Marzia Matucci, Jessica Viti, Andrea Baldini, Alessandro Miglietta, Francesco Cipriani. Piedmont Centre – Cristina Larato, Laura Massari, Leo Nicolina, Luigia Macrì, Stefano Valentini, Carla Contessa, Enrico Albanese, Eva Anselmo, Piero Bestagini, Gabriella Comuniello, Benedetto Francese, Silvia Iodice. Liguria Centre – Susanna Lualdi, Elisabetta Depetrini, Alessandra Franco. Veneto Centre – Helena Frayle, Silvia Gori, Manuel Zorzi. Emilia-Romagna Centre – Francesco Venturelli.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LDM and PGR declared that they have negotiated financial and non-financial support with Becton & Dickinson for the genotyping of stored samples from the New Technologies for Cervical Cancer Screening 2 (NTCC2) study. The other authors report no conflicts of interest.
Funding information
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This project is funded by the National Centre for Disease Prevention and Control (CCM) within the Italian Ministry of Health, grant No D59D16002130001.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.