
Abstract
Objective
To explore the acceptability of high-risk human papillomavirus self-testing, involving community health workers, for never/under-screened Brazilian women. Cervical cancer is the most common cause of cancer-related death among adult women in a large number of low-income and lower-middle-income countries, where it remains a major public health problem. High-risk human papillomavirus persistence is required for the development of cervical neoplasia.
Methods
The target population was all women aged 30+ from the list of families available in healthcare centre data, who had never been screened or were not screened in the previous 3 years (under-screened women), and who were living in the 17 cities included in this study.
Results
Of the 377 women included, 16.9% (n = 64) had never had a pap smear. Of all samples included in the study, 97.1% (n = 366) were considered adequate for evaluation, as 2.9% (n = 11) were considered invalid for all high-risk human papillomavirus types. Analysing these 366 samples, 9.6% (n = 35) of the women were infected by at least one high-risk human papillomavirus type and 90.4% (n = 331) had no infection with any high-risk type of the virus.
Conclusions
Vaginal self-sampling is an adequate strategy to improve the effectiveness of the cervical cancer program by increasing screening in a high-risk group.
Keywords
Background
Cervical cancer has been relatively well controlled for several decades in many high-income countries. However, it is the most common cause of cancer-related death among adult women in a large number of low-income and lower-middle-income countries (LMICs), and remains an important public health problem in these countries. 1 High-risk human papillomavirus (hr-HPV) persistence is required for the development of cervical neoplasia.2–4 Cervical cancer is a preventable disease because of a long pre-invasive period in which the development of precursor lesions, cervical intraepithelial neoplasia (CIN), can be detected by different methodologies. 5 , 6
In the 1970s, the Ministry of Health in Brazil developed a National Cancer Control Program focusing on cervical cancer screening. In 2011, the Brazilian National Cancer Institute published guidelines for cervical cancer screening. Currently, responsibility for developing actions for cervical cancer prevention is a part of primary health care activities. Despite the various initiatives adopted since the early 1970s by the Brazilian authorities, the mortality rates for this cancer have changed little. 7 Estimates made by the National Cancer Institute indicate an incidence of 16,590 new cases for the year 2020 among Brazilian women. 8
Cytology is the method currently recommended to screen women aged 25–64. In Brazil, a large number of women are used to getting pap tests during opportunistic healthcare centre visits, not specifically for cervical cancer screening. Consequently, 20%–25% of the tests have been performed out of the target group. 7
Studies have shown that testing for HPV is more sensitive than cytology for detecting CIN. 9 Self-collection of vaginal samples for HPV testing has also a high sensitivity, as there is fair agreement between self-collected and physician-collected samples.10–12
A systematic review of cost-effectiveness analyses in LMICs found that cytology is not an efficient screening method in low-resource settings. There are barriers to access, implementation and quality assurance for cytology-based screening in LMICs. HPV testing is more cost-effective than cytology. 13
A previous study realized in Brazil evaluated a strategy of screening involving community health workers (CHWs) and self-collection. Women preferred, and were more likely to adhere to, self-collection. 14 The current study aimed to explore the potential acceptability of hr-HPV self-testing involving CHWs for never/under-screened Brazilian women aged 30 and over.
Patients and methods
Intervention context
In Brazil, those who do not have health insurance have public health coverage; health care is provided free of cost. The cervical cancer screening offered by the Brazilian Unified Health System (SUS) is realized using cytology and no molecular test is available. 7 The SUS organizes the municipalities into regions within the Regional Health Directory. The Barretos Cancer Hospital (BCH) and the 18 municipalities that belong to the same directory, called directory five, form a partnership for cervical cancer screening. Once a year, each city receives a mobile unit from the BCH offering a pap smear and mammography. All tests performed are analysed at the Department of Pathology at BCH, using liquid-based cytology. 15
The follow-up and treatment of women with abnormal tests are realized by the Department of Prevention at BCH. Seventeen municipalities of this directory employ full-time CHWs who visit households monthly for health-related tasks. These are as follows: Altair, Barretos, Bebedouro, Cajobi, Colina, Colômbia, Guaira, Guaraci, Jaborandi, Monte Azul Paulista, Olimpia, Severínia, Taiaçu, Taiúva, Taquaral, Terra Roxa and Viradouro. A small city which does not have CHWs did not participate in this study. Each CHW is responsible for 150–200 families and they are used to visiting 10 families every day, in the morning. The Brazilian Institute of Geography and Statistics (IBGE) provides only the absolute numbers of women, aged between 30 and 89 (124,564 women), of the target population residing in the municipalities in our study. 16 During their visits, CHWs collect socio-demographic and health data about the household and its members. A national screening information system (SISCOLO) registers data on cervical cancer screening tests and diagnostic procedures from women attending public health centres opportunistically.
The intervention
In this study, we developed a demonstration screening project including HPV tests performed by self-collection. Between November 2016 and August 2019, the strategy of self-collection offered by CHWs during home visits was implemented. Health authorities decided to involve all CHWs (men and women) and a total of 480 CHWs implemented the strategy.
Target population
The target population was all women aged 30+ on the list of families available in the data kept by healthcare centres, never/under-screened (self-reporting no cervical screen in 3+ years), and who were living in one of the 17 cities. The level of adherence to conventional screening was evaluated by CHWs according to the self-reported information. Pregnant or hysterectomized women and those with no history of previous vaginal intercourse were not enrolled.
Offer of self-collection
During the visit, the CHW would ask questions about the family’s health history and provide women with information about cervical cancer prevention. The participant would be asked to complete a short survey about marital status, education level, age, year of last pap smear, and test preference (the latter was not asked of women who were ‘never screened’). Depending on the eligibility criteria, they were offered HPV self-collection, followed by a two-minute step-by-step explanation on how to perform it, using a support video and communication support material. After signing the consent form, self-samples could be collected at home using the Viba Brush (Rovers Medical Devices, the Netherlands).
Sample handling and transportation to healthcare centres
CHWs labelled vials with the woman’s full name and transported specimens at room temperature to healthcare centres; from here they were sent to the Department of Prevention of BCH by a health system driver. The study coordinator proceeded with the conference of the samples. For oncogenic hr-HPV detection, real-time polymerase chain reaction (RT-PCR) was performed using the Cobas® 4800 HPV test platform (Roche Molecular Systems, Inc., Branchburg, NJ) allowing the detection of 12 hr-HPV genotypes (31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) as a pooled result and genotyping HPV16 and HPV18. DNA was extracted by a fully automated sample preparation process using the Cobas ×480 instrument. The samples were then transferred to the Cobas 4800 HPV test analyzer for hr-HPV DNA amplification by RT-PCR, following the manufacturer's instructions.
Follow-up and treatment
Self-collected HPV-positive women were referred to colposcopy and biopsy if needed at BCH. Women with invalid HPV tests were advised to have a conventional cytology exam. Biopsies were reported according to CIN terminology and were referred to the Pathology Department of BCH where they were processed and classified according to the most recent World Health Organization classification. 17 The clinical follow-up and treatment procedures adopted were based on the results of histopathological analysis. 7 HPV-negative women were advised to undergo repeat screening within 3 years.
Training of CHWs
By the first half of 2016, the researcher had travelled to all the municipalities involved and led 17 four-hour workshops aimed at training all 480 CHWs. At the end of each workshop, CHWs were provided with self-collection kits (two each). The kits were composed of a brush, a vial containing BD Surepath Liquid Preservation (BD, Burlington, NJ), consent forms and questionnaires. A short movie made for this study showing that the steps of collection were shared in a WhatsApp group. If needed, additional kits/materials could be requested using this group. One year after the first workshop, refresher training was provided to all CHWs.
Ethics statement
This study was approved (no. 1142/2016) by the Institutional Review Board (IRB) of the BCH and conducted according to the Declaration of Helsinki.
Data and material conference
As all Pap smear samples are analysed by the Department of Pathology of BCH, the date of previous Pap test filled in by the participant was verifiable in the medical records.
Results
Strategy adherence
The study was carried out between November 2016 and August 2019. A total of 405 women who did not adhere to the conventional screening method were identified by CHWs during home visits. Of these, 380 (93.8%) agreed to participate and proceeded with the self-sample collection. Of the 25 (6.2%) women who refused to participate in the study, the reasons listed were fear of self-injury (n = 2), preference for mobile unit examination (n = 1), lack of sexual activity (n = 2), fear of finding a disease (n = 5), and for no specific reason (n = 15). After checking the questionnaires and medical records, three participants did not meet the inclusion criteria that required at least three years since last Pap test; the samples were analysed but the data were not considered for this study (Figure 1).
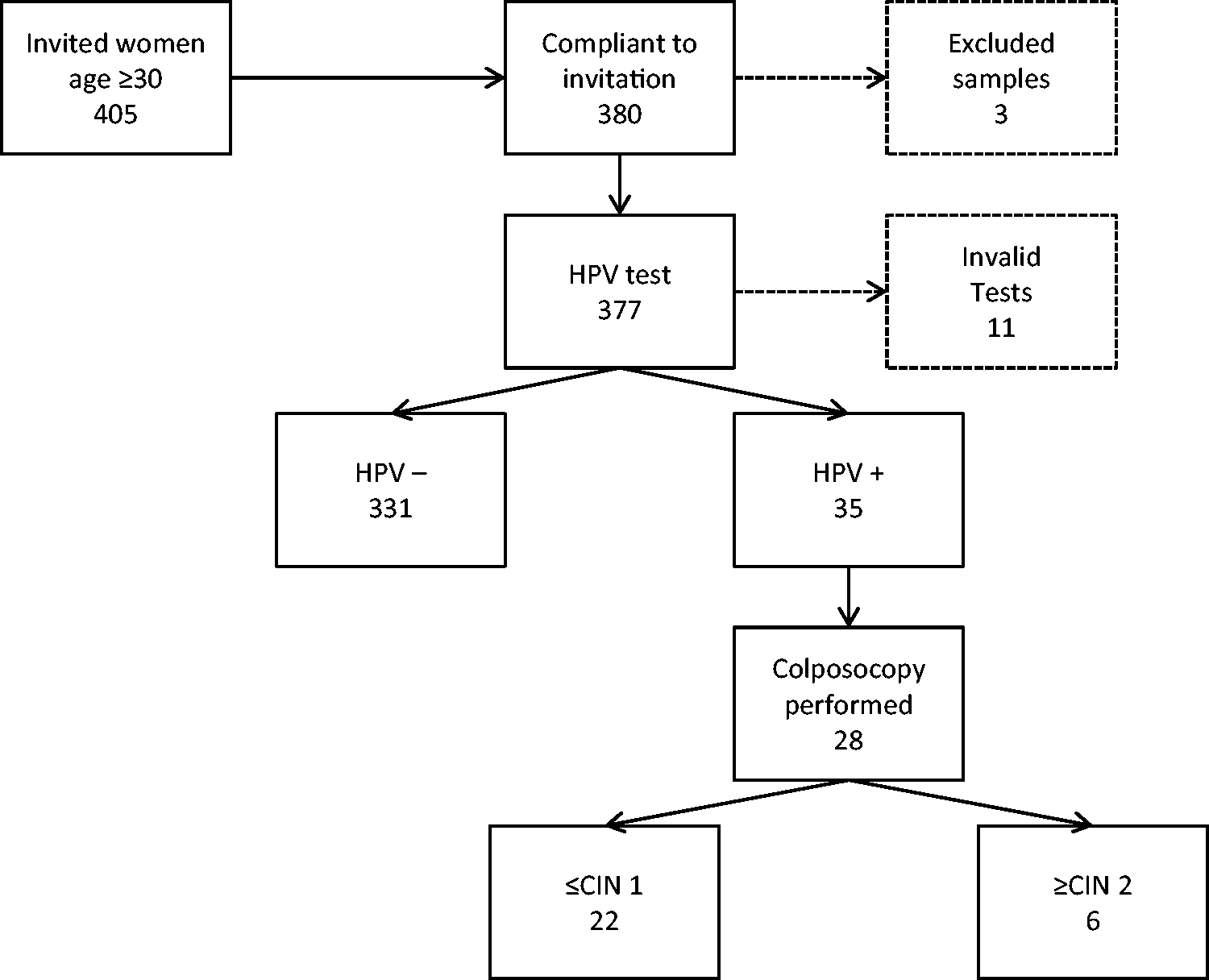
Flowchart and main data of the human papillomavirus test-based screening strategy: years 2016–2019.
Population characteristics
The mean age of the participants was 49.4 (SD: 12.9; 30–86). The age distribution and self-reported sociodemographic characteristics are presented in Table 1.
Sociodemographic characteristics of the study participants (N = 377): women from regional health directory V, São Paulo State, 2016–2019.
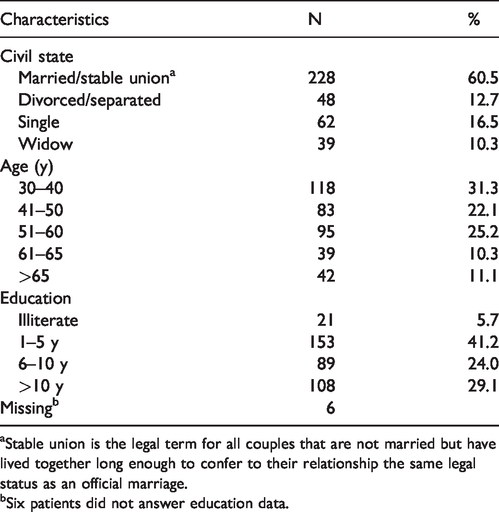
aStable union is the legal term for all couples that are not married but have lived together long enough to confer to their relationship the same legal status as an official marriage.
bSix patients did not answer education data.
History of previous Pap smear
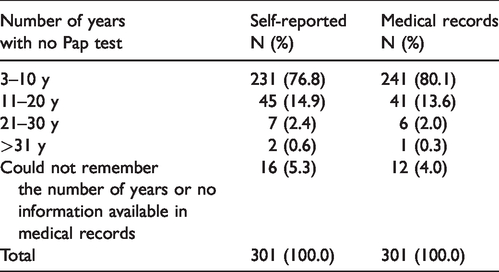
Of the 377 women included, 16.9% (n = 64) had never had a Pap smear. An additional 12 women (3.2%) did not report any information about a previous Pap and no registration was available in the medical records. These samples were not excluded. Considering the 301 women with at least one registration available and a previous Pap collected, the self-reported and medical record data are presented in Table 2. Women included were at least eight years (SD: 5.3; 3–33) without undergoing a preventive test according to the medical records.
Number of years without a preventive test self-reported and according to medical records (São Paulo State, 2016–2019).
Test preference
Participants who had previously undergone a Pap test were asked for their preferred method. A total of 270 (86.3%) reported a preference for self-sampling. Only 10 women (3.2%) preferred to continue with the Pap test. Two women (0.6%) reported not liking either choice, 10 (3.2%) stated that the type of test did not matter to them, and 21 (6.7%) could not specify a preference. Obese and bedridden women included in this study reported self-sampling preference.
High-risk HPV testing
Of all samples included in the study, 97.1% (n = 366) were considered adequate for evaluation and 2.9% (n = 11) were considered invalid for all hr-HPV types. Among the 366 valid samples, 9.6% (n = 35) of the women were found to be infected by at least one hr-HPV type and 90.4% (n = 331) showed no infection with any high-risk type of the virus. Table 3 shows the frequency of each HPV genotype.
HPV results by Cobas 4800 system.
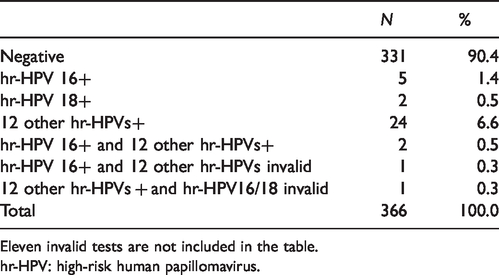
Eleven invalid tests are not included in the table.
hr-HPV: high-risk human papillomavirus.
Patient follow-up
A total of 35 women were contacted and referred for colposcopy examination. However, five (17.1%) refused to attend the hospital and one of these (2.9%) chose a private appointment for further investigation. A total of 28 (80%) women completed the colposcopy procedure. Macroscopic impression, squamous-columnar junction visibility, and histopathology and cytology results are detailed in Table 4. CIN2+ lesions were detected in six patients.
Results of colposcopy procedures.
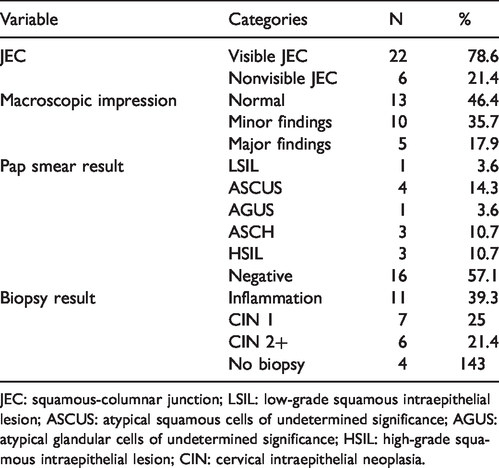
JEC: squamous-columnar junction; LSIL: low-grade squamous intraepithelial lesion; ASCUS: atypical squamous cells of undetermined significance; AGUS: atypical glandular cells of undetermined significance; HSIL: high-grade squamous intraepithelial lesion; CIN: cervical intraepithelial neoplasia.
Discussion
This study shows that, in Brazil, HPV self-testing has high acceptability and can be an effective strategy to increase adherence to cervical cancer screening. It can be easily incorporated as part of the screening program to reach under-screened women. After approach by CHWs, the data and samples were collected in the women’s houses. Considering that CHWs perform routine home visits as part of health programs, resources would be more efficiently invested if, during these home visits, under-screened women were offered the self-sampling alternative. No patients included in this study were approached in a hospital or outpatient health unit facility. The purpose of this study was precisely to introduce a new strategy for never/under-screened women.
If records of the women targeted by the cervical cancer program were available, those who did not adhere to the conventional screening strategy could be searched for and contacted. However, in Brazil, the records and information about preventive tests are incomplete. In this study, women never/under-screened were identified during household visits. Field workers required only a short training session; additionally, since the HPV test does not require refrigeration of samples, they did not need to carry excessive materials and therefore could perform visits in remote areas. 18
The coverage rate for the cervical cancer screening program in Brazil, i.e., the number of women who undergo a Pap test within three years, is estimated to be below 70%. The Brazilian screening program is considered opportunistic, with no control over the screened population, resulting in a small impact on the incidence and mortality from cervical cancer. 19
There are several methods to offer self-sampling, such as self-sampler by mail directly at home, self-sampling device up at an area pharmacy, invitation letters, and using CHWs.20–22 This study involved CHWs and we did not face any major logistical problems.
Some studies have shown a high acceptance of self-collected vaginal tests among women who do not attend the cytological cervical screening service. 18 , 23 Our high acceptance rate (93.8%) could be explained by the use of home visits. This study did not explore knowledge around cervical cancer screening. CHWs realized that some women are not aware of the recommended frequency of Pap tests. Women have correctly stated that the Pap test can prevent cervical cancer but they have difficulty knowing the frequency and when screening should begin. 24
Factors associated with preference for vaginal self-sampling by non-attendees to Pap test might include experiencing less fear and avoiding the uncomfortable position required for a gynecological exam. In our study, 86.3% reported a preference for self-sampling. The acceptability of self-sampling is also related to its practicality and could be especially useful for women with difficulties accessing a health centre. Other studies have reported that the majority of participants said it was better to perform their own exam in their own time instead of being examined by a professional with the need for an appointment. 22 , 25
A total of 9.6% of the valid samples in our study were found to be hr-HPV positive for at least one genotype. Over 46% of the HPV-positive women had a negative colposcopy, and among those who underwent biopsy 39% were negative. Our study did not increase the demand for colposcopy, but an increase in the colposcopy and cervical biopsy rate has been reported as a result of using the more sensitive molecular HPV test instead of cytology for screening. 26
In Brazil, studies on the use of self-sampling HPV tests have been developed in different settings, such as rural areas, hospitals, remote areas and in home visits performed by CHWs.14,27–30 Studies realized in a hospital setting offered self-collection for Brazilian women who were looking for a preventive test. The participants reported high acceptance and understanding of the procedure 27 and 12.3% were shown to have at least one HPV genotype. 28 In remote areas, self-administered sampling had a high level of acceptance among Brazilian women, with only 2% disapproving of the procedure; 95% considered it simple to perform and 80% preferred this mode to collection by a health professional. 29 A previous study developed by our group was designed to evaluate the use of self-sampling for HPV in the rural communities served by BCH. We trained a local police officer, and a high acceptance of self-sampling was reported. 30
Our study had some limitations. First, we were not told how many women in total were contacted by the CHWs; therefore, we cannot evaluate how successful they were in the offer of self-collection and the proportion of screening-age women that were covered by this intervention. Second, we used a simplified form to avoid increasing the length of home visits, and health characteristics were not collected. Third, most screening programs focus on women aged <65, but we did not set an upper age limit for participants. 7
Conclusions
This study shows that vaginal self-sampling is an adequate strategy to improve the effectiveness of the cervical cancer program, by increasing screening in a high-risk group. Ideally, prevention strategies should be developed according to each region and population, and future studies could assess the implementation of other recruiting strategies.
Footnotes
Acknowledgements
Our thanks to the biologist Fernanda Cury who analysed all samples for HPV testing, and to the CHWs.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Public Ministry of Labor of São Paulo State for the financial support.