
Abstract
Objective
Roll-out of population-based colorectal cancer (CRC) screening with faecal immunochemical test (FIT) is limited by availability of further investigations, particularly colonoscopy and examination of excised lesions. Our objective was to assess whether variation in number of faecal samples and threshold adjustment can optimise resource utilisation and CRC detection rate.
Methods
Three different screening strategies were compared for the same FIT threshold using a quantitative FIT system: one FIT, positive when
Results
In our setting, Region of Murcia, south of Spain (not fully rolled out screening programme), changing the usual strategy of two FIT, positive when either to positive when the mean was
Conclusions
In a population-based CRC screening programme, smart use of number of FITs and positivity threshold can increase population invited and CRC detection without increasing the number of colonoscopies and pathological examinations needed.
Introduction
Colorectal cancer (CRC) has high incidence and age-adjusted mortality world-wide: in 2018, there were over 1,849,000 new cases and more than 880,000 deaths. 1 CRC fulfils the criteria proposed by the World Health Organization (WHO) for the implementation of population-based screening programmes. 2 Several randomised controlled trials and meta-analyses have demonstrated the efficacy of such programmes.3,4 In consequence, in 2003, the European Council recommended that CRC should be subject to population-based screening campaigns in EU Member States and a test for the presence of occult blood in faeces offered to the population aged between 50 and 74 years, adjusting the age range according to the local epidemiology of CRC and each country's priorities. 5 In response to this recommendation, several States developed their own strategies and guidelines, 6 including Spain,7,8 France, 9 United Kingdom, 10 The Netherlands 11 and Italy. 12
One important aspect of implementation of such programmes is to offer the participants a two-fold guarantee of continuity 13 to ensure that (a) participants will be invited over the entire recommended age range and (b) if the screening test result is positive, the system must facilitate access to diagnostic confirmation techniques, adequate treatment and subsequent surveillance. For CRC, once the initial faecal test results are available, colonoscopy is usually offered to participants whose results suggest a greater likelihood of CRC. 6 Screening colonoscopy is a complex investigation which requires specific instrumentation, highly trained staff and considerable patient involvement time, since it might involve the excision and retrieval of polyps and other lesions, and biopsies of suspicious findings. Therefore, it is understandable that health services’ capacities to cope with this type of follow-up may be limited. Developing strategies to increase the detection of CRC when colonoscopy capacity is constrained is necessary. One reasonable approach to solving this problem is optimising the faecal test strategy.
Several approaches to optimisation have been taken, most importantly the use of faecal immunochemical tests (FITs) versus the traditional guaiac-based faecal occult blood tests,14–16 but also a two-tier reflex approach, 17 varying screening frequency 18 or the threshold used with FIT,19,20 personalising the threshold by including factors such as sex and age in a risk-score,21–24 or going further, for example through neural network risk modelling. 25 The European Commission's scientific advisors advocate the approach of threshold individualisation as a way to improve CRC screening programmes. 26 Implementing a programme means deciding about the type of FIT to be used, the faecal haemoglobin concentration (f-Hb) threshold for declaring a result as positive, the number of FITs to be used and the format of the FIT. Few studies have compared one to two or three FITs 27 and only one has compared three alternatives. 28
The objective of this study was to compare three alternatives for the same positive FIT threshold (
Methods
The colorectal cancer screening programme
of the region of Murcia (Spain)
In the Region of Murcia, following recommendations, 29 the pilot project for the CRC screening programme with FIT and colonoscopy began in 2006. 30 Women and men aged between 50 and 69 years in two Health Areas were invited, except for the population in the old part of the city of Murcia: 16,975 were invited in 2006. The roll-out of the programme to other Health Areas began in 2008 and was further extended in 2009. In 2018, coverage had been extended to 130,929, 39.5% of the target population of the Region. The details of the biennial invitation screening methodology are fully described in Supplement 1. Exclusion criteria are detailed in Supplement 2.
Faecal immunochemical tests (FIT)
This study is based on data available in the management and assessment application of the CRC screening programme of the Region of Murcia (PCAColon) since the introduction of FIT (HM-JACKarc, Minaris Medical Co., Ltd, Tokyo, Japan) from 01 July 2014 to 31 December 2018. The data concern participants who submitted testable FIT devices. The two FIT samples are taken from successive bowel motions. Registry order is random, it doesn't take defecation date into account, although it is checked that they belong to successive motions.
Full details of what each variable means, further variable transformation, and generation of estimates of the variations compared for each strategy and estimates in fully rolled out programmes are shown in Supplement 3.
Strategy comparison
As stated above, the aim was to compare three alternative strategies for the same positive FIT threshold (
Statistical analysis
For each strategy, the positivity (absolute value) and the positivity as a percentage of positive FIT results in the total number of participants was obtained; the values of the diagnostic categories (CRC; high risk adenoma, HR; intermediate risk adenoma, IR; and low risk adenoma, LR), their detection rates as the percentage of the total number of participants with testable FIT and the positive predictive values (PPV) for each of the diagnostic categories, as the percentage of each diagnosed category out of the total number of positive results. For programmes that are not fully rolled out, each of the strategies was compared to other two, calculating the percentage increase in the invited population and the results expected from the new strategy with regard to the reference strategy: this is the proportional (algebraic) increase of the invited population in the strategy we want to compare with that of the reference strategy expressed as a percentage. With A being the population of the reference strategy and B the new population estimated from A, the aim is to calculate this increase provided that: 1) the participation rate is the same in both strategies; 2) the rate of positives is the one of the strategy being compared; and 3) the number of positives is the same as in A (hence, with the same number of colonoscopies). Therefore, the result obtained is a percentage (positive or negative) that shows the variation of the invited population (B) with respect to the invited population in the reference population (A). For programmes that have been extended to the entire target population, the percentage increases in positive results and the detection of each diagnostic category were calculated regarding those which corresponded to the reference strategy in the comparison. In other words, we estimated the corresponding change in the size of the population which the provider could invite to screening while maintaining the same number of positive results (i.e. the same number of colonoscopies). The 95% confidence intervals were calculated.
Results
A total of 114,049 people participated during the study period (participation rate varied between 44.0% and 53.9% in the years studied); 42.9% (Table 1) participated for the first time (initial screening), whereas the remainder had already participated (successive screening).
Results of the colorectal cancer screening programme from 01 July 2014 to 31 December 2018 in the region of murcia, Spain: participants, detected cancers and participants classified as high (HR), intermediate (IR) or low (LR) risk from the characteristics of the adenomas detected during the study period, distributed by type of screening, age and sex.
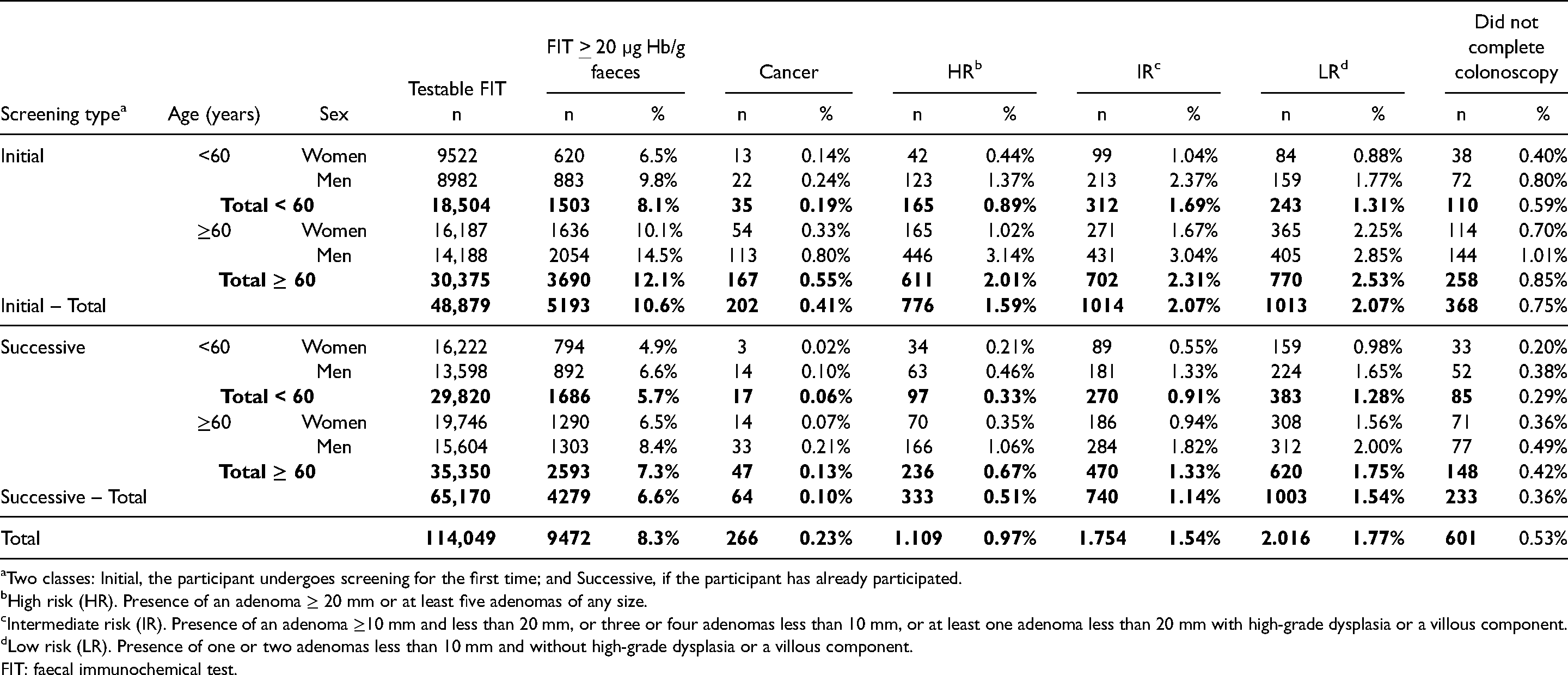
Two classes: Initial, the participant undergoes screening for the first time; and Successive, if the participant has already participated.
High risk (HR). Presence of an adenoma ≥ 20 mm or at least five adenomas of any size.
Intermediate risk (IR). Presence of an adenoma ≥10 mm and less than 20 mm, or three or four adenomas less than 10 mm, or at least one adenoma less than 20 mm with high-grade dysplasia or a villous component.
Low risk (LR). Presence of one or two adenomas less than 10 mm and without high-grade dysplasia or a villous component.
FIT: faecal immunochemical test.
By sex, while almost 54.1% of the participants and 45.8% of those with positive results were women, we found a lower proportion of women with CRC (31.5%). Differences by sex were similar with high-risk adenomas (HRA), intermediate-risk adenomas (IRA) and low-risk adenomas (LRA) too (percentage of women: 28.1%, 36.7% and 45.6%, respectively).
By age, 42.4% of the participants were under 60 years. Of those with positive FIT, only 33.7% belonged to this age group. We found a lower percentage of CRC and related lesions among them, as well (cancer: 19.5%; HR: 23.6%; IR: 33.2%; LR: 31.1%), compared to the ≥ 60 years group.
In the programme's usual strategy, (two samples, positive when at least one was ≥20 µg Hb/g faeces
Results of the colorectal cancer screening programme from 01 July 2014 to 31 December 2018 in the Region of Murcia: neoplasia detection rates and positive predictive values (PPV) with 95% confidence intervals (CI) depending on the screening strategy.
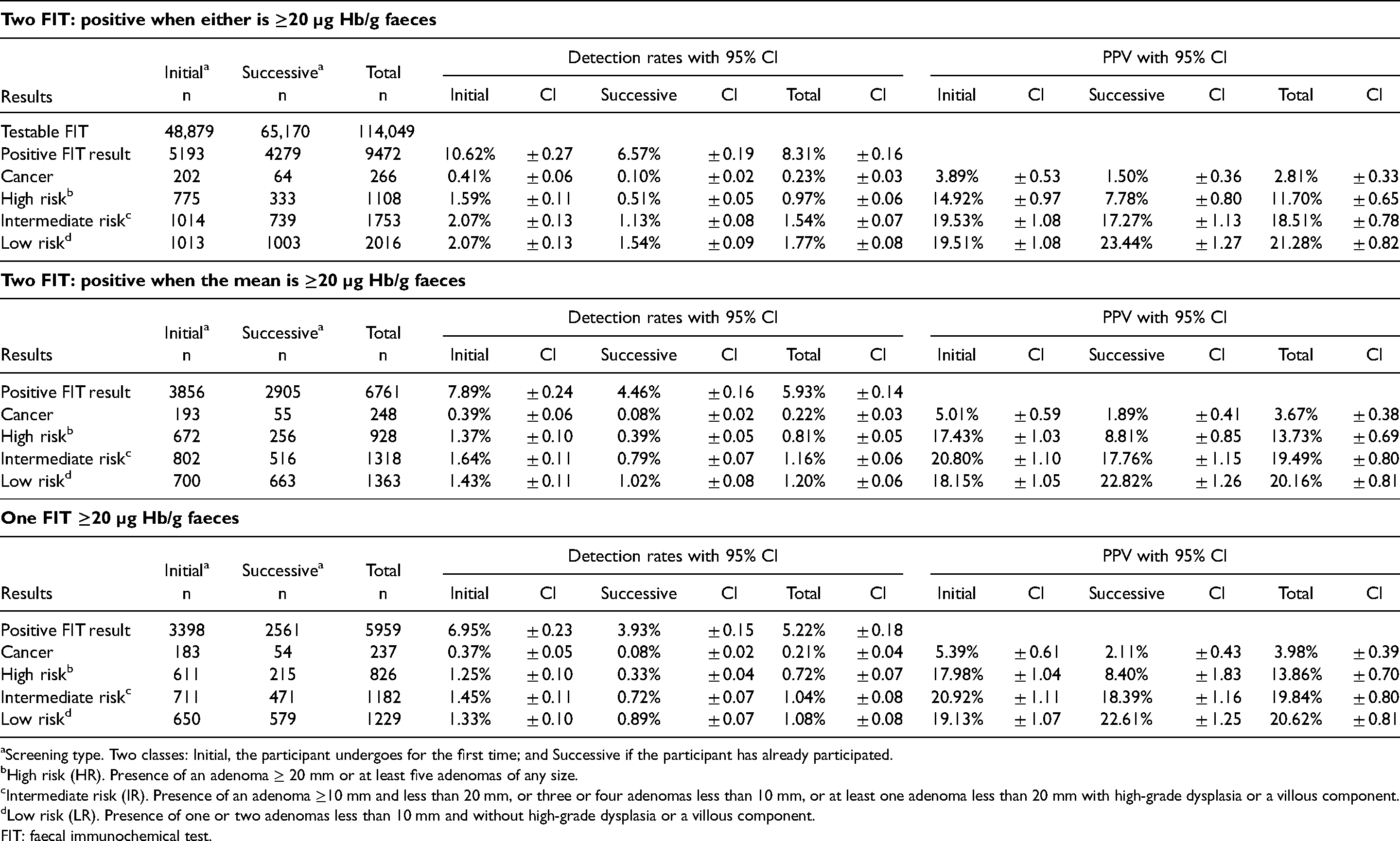
Screening type. Two classes: Initial, the participant undergoes for the first time; and Successive if the participant has already participated.
High risk (HR). Presence of an adenoma ≥ 20 mm or at least five adenomas of any size.
Intermediate risk (IR). Presence of an adenoma ≥10 mm and less than 20 mm, or three or four adenomas less than 10 mm, or at least one adenoma less than 20 mm with high-grade dysplasia or a villous component.
Low risk (LR). Presence of one or two adenomas less than 10 mm and without high-grade dysplasia or a villous component.
FIT: faecal immunochemical test.
In the next strategy (two samples, positive when the mean was ≥20 µg Hb/g faeces), positivity fell to 6.0% (Table 3), being 8.1% in initial and 4.5% in successive participants. However, the CRC detection rate only fell from 0.23% to 0.22%; from 0.41% to 0.39% in initial and from 0.10% to 0.08% in successive participants. In contrast, positivity for HRA fell from 0.97% to 0.81%; from 1.59% to 1.37% in initial and from 0.51% to 0.39% in successive participants. The differences in the IRA and LRA were greater.
Distribution of each studied strategy. By screening type, age, and sex, of the main results: Positivity.
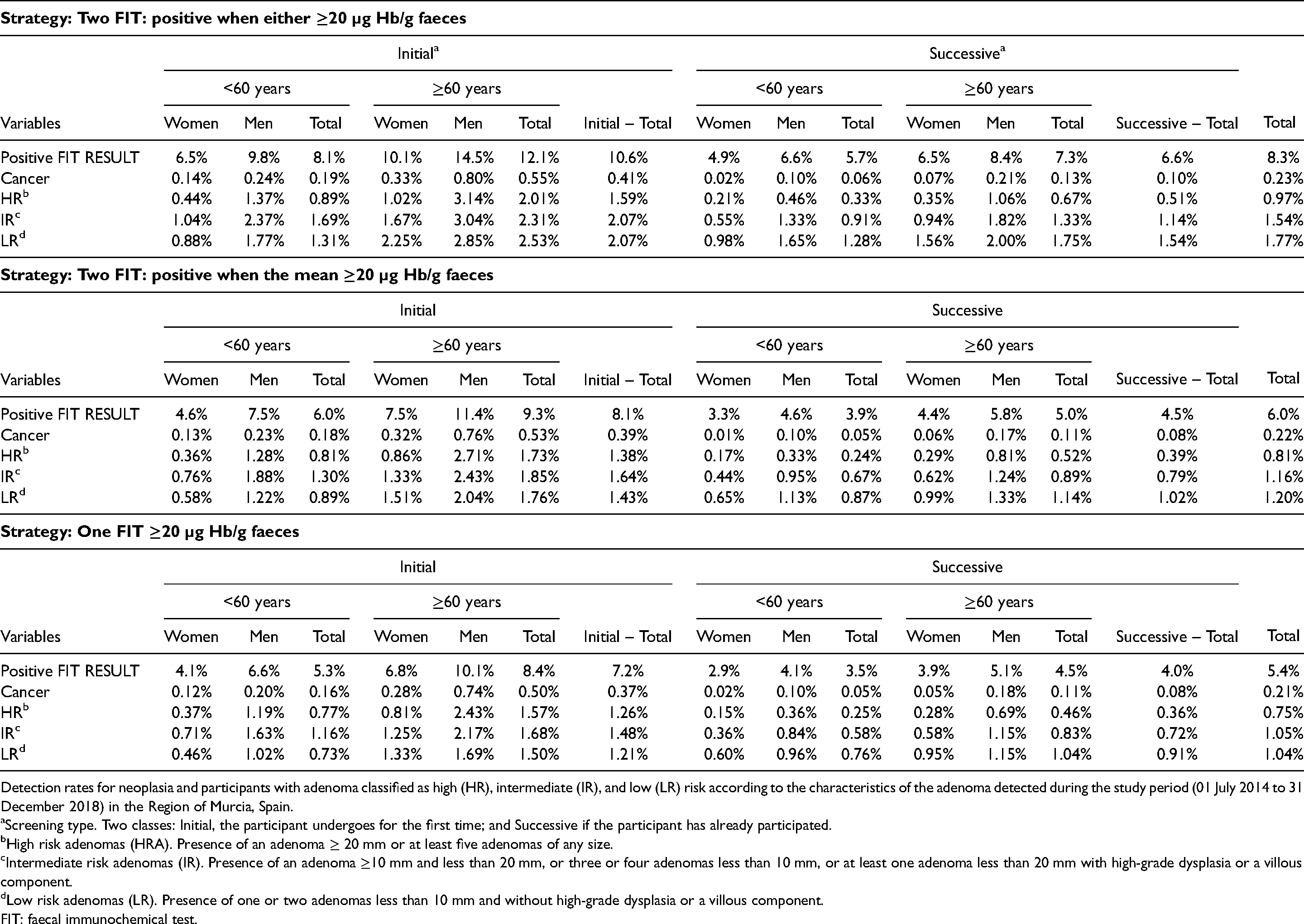
Detection rates for neoplasia and participants with adenoma classified as high (HR), intermediate (IR), and low (LR) risk according to the characteristics of the adenoma detected during the study period (01 July 2014 to 31 December 2018) in the Region of Murcia, Spain.
Screening type. Two classes: Initial, the participant undergoes for the first time; and Successive if the participant has already participated.
High risk adenomas (HRA). Presence of an adenoma ≥ 20 mm or at least five adenomas of any size.
Intermediate risk adenomas (IR). Presence of an adenoma ≥10 mm and less than 20 mm, or three or four adenomas less than 10 mm, or at least one adenoma less than 20 mm with high-grade dysplasia or a villous component.
Low risk adenomas (LR). Presence of one or two adenomas less than 10 mm and without high-grade dysplasia or a villous component.
FIT: faecal immunochemical test.
In the one-test strategy (in which one of the two FIT results was examined), with the same threshold (Table 3), the positivity fell to 5.4%; 7.2% in initial and 4.0% in successive participants. Here, the CRC detection rate fell from 0.23% to 0.21%; from 0.41% to 0.37% in initial and from 0.10% to 0.08% in successive participants. The detection rates of HRA, IRA and LRA showed a noteworthy reduction.
The estimates of the possible changes in strategy maintaining the f-Hb threshold at ≥20 µg Hb/g faeces (Table 4) showed:
Population A (two FIT, positive when either is ≥20 µg Hb/g faeces) versus Population B (positive when the mean is ≥20 µg Hb/g faeces): with the same positivity, the invited population may increase by 37.81%, also achieving, if the correction for false negative FIT results is not included in the comparison strategy with regard to the reference strategy, an increase of 28.49% in CRC detected, 15.43% more HR, 3.62% more IR and reducing the detection of LR by 6.82%. Population A (two FIT, positive when one ≥20 µg Hb/g faeces) versus Population B (one FIT ≥20 µg Hb/g faeces): with the same positivity, the invited population might increase by 56.20%, achieving an increase of 39.17% in CRC detected, and 16.45% more in HR, 5.32% more in IR and a 4.78% reduction in LR. Population A (two FIT, positive when the mean is ≥20 µg Hb/g faeces) versus Population B (one FIT ≥20 µg Hb/g faeces): with the same positivity, the invited population might increase by 13.34%, achieving an increase of 8.31% in CRC detected, 0.88% in HR, 1.65% in IR and 2.20% in LR.
Distribution of the proportional detection rate increases (Δ%) by changing the screening strategy on invited population; invasive cancer detection, and high, intermediate, and low risk adenoma detected.
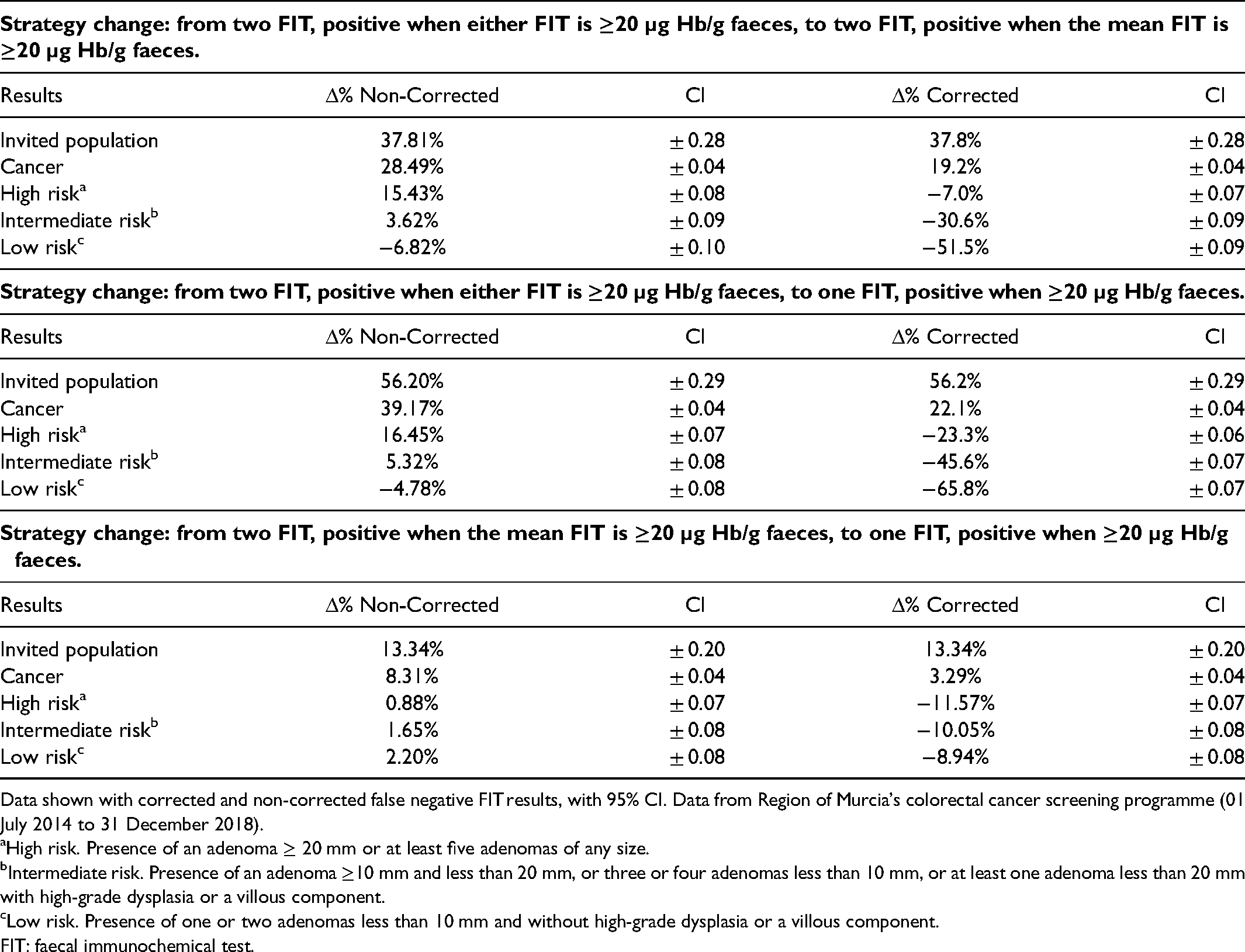
Data shown with corrected and non-corrected false negative FIT results, with 95% CI. Data from Region of Murcia's colorectal cancer screening programme (01 July 2014 to 31 December 2018).
High risk. Presence of an adenoma ≥ 20 mm or at least five adenomas of any size.
Intermediate risk. Presence of an adenoma ≥10 mm and less than 20 mm, or three or four adenomas less than 10 mm, or at least one adenoma less than 20 mm with high-grade dysplasia or a villous component.
Low risk. Presence of one or two adenomas less than 10 mm and without high-grade dysplasia or a villous component.
FIT: faecal immunochemical test.
In populations for which the programme is not fully rolled out, by changing from the one to two FIT strategy, positive when the mean is ≥20 µg Hb/g faeces (Table 5), there would be a proportional increase in positivity of 13.34%. For CRC, there would be an increase in detected cases of 4.64% and a reduction in the PPV for CRC of 7.68%. The increase in the detection rate of HR would be 12.35% and of IR 11.51%.
Screening strategy change effects on FIT positivity, cancer detection, and adenoma detection (3 risk categories), shown as proportional detection rate variation (Δ%) and positive predictive value variation (Δ%).
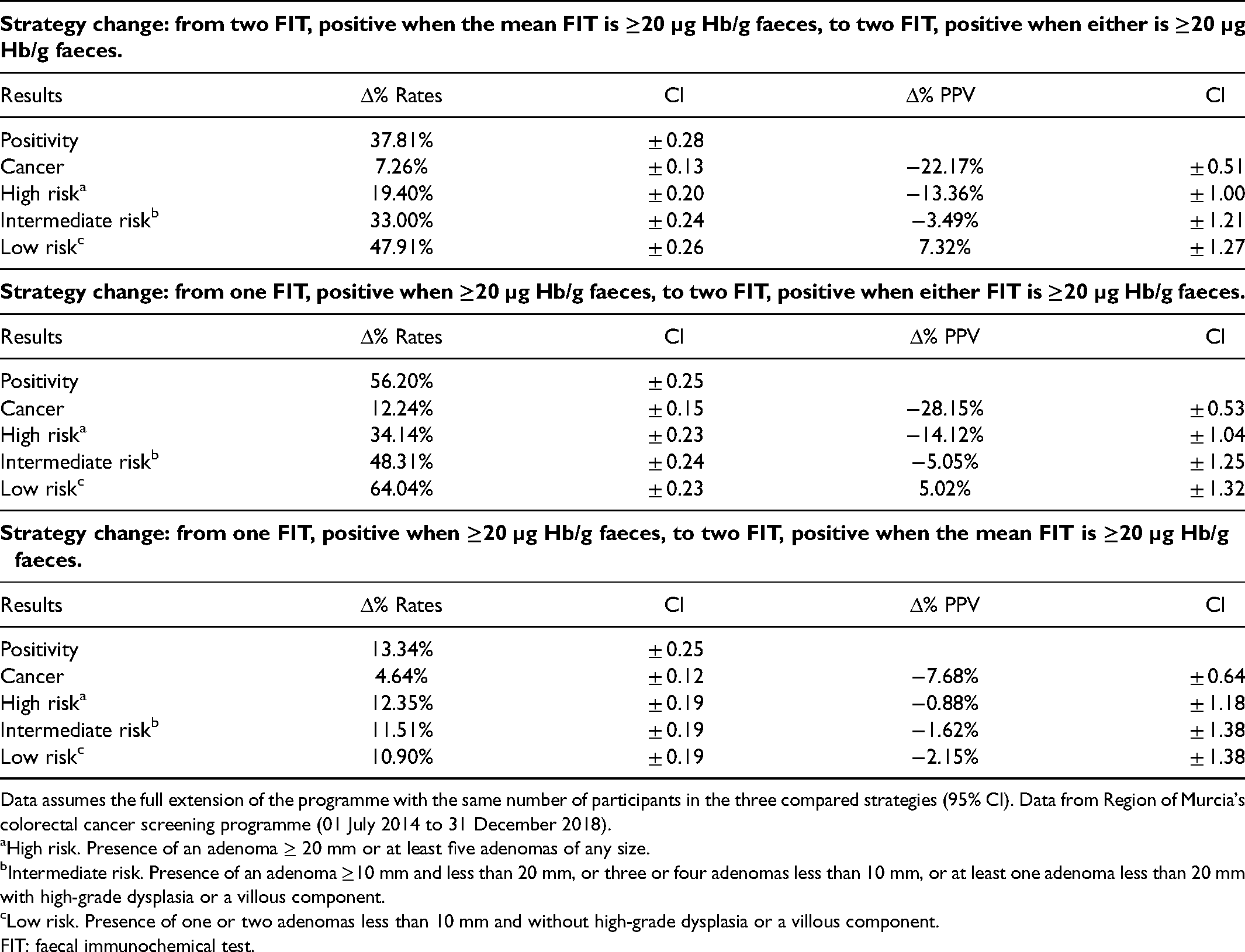
Data assumes the full extension of the programme with the same number of participants in the three compared strategies (95% CI). Data from Region of Murcia's colorectal cancer screening programme (01 July 2014 to 31 December 2018).
High risk. Presence of an adenoma ≥ 20 mm or at least five adenomas of any size.
Intermediate risk. Presence of an adenoma ≥10 mm and less than 20 mm, or three or four adenomas less than 10 mm, or at least one adenoma less than 20 mm with high-grade dysplasia or a villous component.
Low risk. Presence of one or two adenomas less than 10 mm and without high-grade dysplasia or a villous component.
FIT: faecal immunochemical test.
Discussion
The design and delivery of the screening programme studied here differ somewhat from others in Spain, 31 and other countries. 32 The positivity was greater, as were detection rates (particularly those in participants with HR and IR though less significantly for CRC), particularly when compared to longer running programmes, perhaps mainly due to the different screening strategies. Although the f-Hb threshold for positivity is often ≥20 µg Hb/g faeces, our programme uses two FITs collected from consecutive bowel motions, being termed positive when either is ≥20 µg Hb/g faeces. This yields a high positivity, which necessitates a high number of colonoscopies: this has hampered the rapid roll-out of the programme to the entire target population in the Region. As in other programmes, the positivity and neoplasia detection rates varied depending on the screening round, age, and sex. In general, these were greater in those undergoing initial as opposed to successive screenings, men as opposed to women, and participants ≥60 years versus those <60 years. In the first round, all participants are undergoing an initial (prevalence) screening, whereas in the successive (incident) rounds there are increasingly more participants (Table 1); moreover, participants in initial screening are younger, meaning that there are important overall reductions in positivity and detection rates over time.
As expected, a change of strategy meant changes in the positivity, neoplasia detection rates and PPV (Table 2). Thus, on changing from the two FIT strategy in which the result is regarded as positive when at least one is ≥20 µg Hb/g faeces to positive when the mean is ≥20 µg Hb/g faeces, or to a one FIT ≥20 µg Hb/g faeces strategy, there is a reduction in positivity (8.31%; 5.93% and 5.22%, respectively) which is statistically significant; the CI do not overlap. In contrast, the CRC detection rates show very small differences (0.23%; 0.22% and 0.21%), with overlapping CI, although the 0.02% difference in the rate is equivalent to 29 fewer CRC detected during the study. However, the reduction in the aggregated HR plus IR detection rates is significant: 2.51%, 1.97% and 1.76%, whose CI do not overlap, which could lead to a loss in programme capacity to reduce incidence. 32 Finally, there is a gain in PPV (for all CRC, HR, IR plus LR combined detection): 54.3%; 57.1% and 58.3% respectively, and therefore a somewhat greater clinical efficiency of colonoscopy. Interestingly, the results of the one FIT strategy are comparable to those of other programmes that use the same strategy31,32: it is therefore plausible that our results and others 33 using two FITs are transferable to other programmes.
Toyoshima et al. have recently undertaken a comparison of the results obtained using two FITs, with a result being declared positive when either f-Hb is above the threshold, with using one FIT and no FIT. As expected, using two FITs gives a much higher yield of more advanced colorectal neoplasia than the other two strategies. In contrast to our work, the capacity of the health system to cope with the increase in colonoscopies due to the higher detection rate was not considered. 34 Turvill et al. have also recently contributed showing no improvement in diagnostic yield using one or two FITs, but their study assessed FIT in patients presenting with symptoms, not in an asymptomatic screening population. 35
A germane question is to what extent would a change in strategy that reduces the positivity and allows an increase in the participating population without changing the total number of participants with positive FIT results (and therefore the same colonoscopy requirement) affect neoplasia detection rates. This study has shown (Table 4) that either of the two alternatives substantially increases the proportion of those that can be invited and the detection of CRC, HR and LR when there is no correction for false negative FIT results, although the increased detection of HR and IR is lost when the correction is applied. In our opinion, these results justify a change of strategy, both on account of the greater capacity to detect neoplasia and increasing equality, since coverage can be broadened with the same colonoscopy requirement. Thus, which of the two alternatives should be chosen? If false positive test result correction is not used, the one FIT alternative is clearly better. On the other hand, if correction is used, both alternatives have their pros and cons. In the alternative where the mean of two FITs is used, the increased population coverage and CRC detection rate are somewhat lower, although presenting a greater detection rate for participants with HR and IR, likely meaning that the primary prevention capacity is greater.
Finally, when the programme has reached, or approached, 100% coverage rate, is a change of strategy reasonable? According to this study, perhaps. Indeed, in one FIT programmes, switching to two FIT, where the result is positive when the mean is above the set threshold (Table 5), increases the CRC detection rate (4.64%) and that of other significant neoplasia (12.35% HR and 11.51% IR), whose excision has been associated with a lower incidence of CRC.36,37 Although the number of positive FIT results increases (13.34%), this does not have a substantial effect on colonoscopy (PPV: −7.68%, −0.88% and −1.62%, respectively). In fact, this increase in colonoscopy requirement can be absorbed by the programme's diagnostic confirmation strategies, since the increased workload is lower than the reduction in participants with FIT positive results due to a greater population undergoing successive screening. Indeed, as shown (Table 2), the positivity in participants undergoing initial screening when one FIT is used (6.95%) is greater than the total positivity when two FITs are used and the mean is used for classification (5.93%). Moreover, as the rounds in a programme progress, the population ≥60 years is almost exclusively undergoing successive screening (with lower positivity) whereas the younger population is undergoing initial screening and the positivity is also lower than at older ages.
One very interesting aspect is to consider the distribution of the results of the three strategies across the different categories of type of screening, age, and sex. That said, a weakness of this study is our lack of data in some of the subgroups (divided by sex, age and colonoscopy findings), which makes our statistical analysis less powerful. Another drawback is that the study was performed using data from an organised programme and not designed as a specific research study. Therefore, although there do exist protocols for performance of colonoscopy, there may be greater inter-observer differences than in research studies. However, this could also be a strength of the study since the data are from an organised programme, reflecting actual practice.
It is important to consider that the characteristics of the one FIT strategy, in which one FIT result is selected, could impact the participation rate in the screening programme, since greater participation might be expected with one FIT required than with two, and therefore this could result in an artificially reduced CRC and adenoma detection rate. Nevertheless, careful revision of similar studies showed that the differences in participation in screening programmes using either one or two FITs were either insignificant or low, and thus the number of FITs would not be likely to have a major impact on our findings.38–42
In conclusion, in a situation in which colonoscopy resources are limited, thus hampering the rapid roll-out of a screening programme to the entire population, beginning the programme with one FIT seems a good strategy, with the threshold for positivity being
Supplemental Material
sj-docx-1-msc-10.1177_09691413221094919 - Supplemental material for One or two faecal immunochemical tests in an organised population-based colorectal cancer screening programme in Murcia (Spain)
Supplemental material, sj-docx-1-msc-10.1177_09691413221094919 for One or two faecal immunochemical tests in an organised population-based colorectal cancer screening programme in Murcia (Spain) by Carlos Tourne-Garcia, Francisco Perez-Riquelme, Olga Monteagudo-Piqueras, Callum G Fraser and Pedro Yepes-Garcia in Journal of Medical Screening
Supplemental Material
sj-docx-2-msc-10.1177_09691413221094919 - Supplemental material for One or two faecal immunochemical tests in an organised population-based colorectal cancer screening programme in Murcia (Spain)
Supplemental material, sj-docx-2-msc-10.1177_09691413221094919 for One or two faecal immunochemical tests in an organised population-based colorectal cancer screening programme in Murcia (Spain) by Carlos Tourne-Garcia, Francisco Perez-Riquelme, Olga Monteagudo-Piqueras, Callum G Fraser and Pedro Yepes-Garcia in Journal of Medical Screening
Supplemental Material
sj-docx-3-msc-10.1177_09691413221094919 - Supplemental material for One or two faecal immunochemical tests in an organised population-based colorectal cancer screening programme in Murcia (Spain)
Supplemental material, sj-docx-3-msc-10.1177_09691413221094919 for One or two faecal immunochemical tests in an organised population-based colorectal cancer screening programme in Murcia (Spain) by Carlos Tourne-Garcia, Francisco Perez-Riquelme, Olga Monteagudo-Piqueras, Callum G Fraser and Pedro Yepes-Garcia in Journal of Medical Screening
Footnotes
Authors’ Contributions
CTG was the main contributor on the Methods section and one of the coordinators of the screening programme. FPR was the main contributor on the Results and Discussion section, and the main responsible of the screening programme. OMP contributed significantly to the analysis, interpretation of the data and quality control of the study database, and was the main coordinator of the screening programme. CGF contributed significantly to the analysis and interpretation of the data and to the writing of the paper. PYG was the main contributor on the Introduction section and helped with the coordination of all the previous authors. All authors approved of the final draft submitted.
Patient Consent for Publication
Not required. It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Data Availability Statement
Data are available upon reasonable request to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.