
Abstract
Objective
To investigate the relationship between deprivation and faecal haemoglobin concentration (f-Hb).
Setting
Scottish Bowel Screening Programme.
Methods
A total of 66725 men and women, aged 50 to 74, were invited to provide a single sample for a faecal immunochemical test. Deprivation was estimated using the Scottish Index of Multiple Deprivation quintiles: f-Hb was measured (OC-Sensor, Eiken, Japan) on 38439 participants. The relationship between deprivation quintiles and f-Hb was examined.
Results
Median age was 60 years, 53.6% women, with 14.1%, 19.7%, 17.7%, 25.9% and 22.6% in the lowest to the highest deprivation quintiles respectively. No detectable f-Hb was found in 51.9%, ranging from 45.5% in the most deprived up to 56.5% in the least deprived. As deprivation increased, f-Hb increased (p < 0.0001). This trend remained controlling for sex and age (p < 0.001). Participants in the most deprived quintile were more likely to have a f-Hb above a cut-off of 80 µg Hb/g faeces compared with the least deprived, independent of sex and age (adjusted odds ratio 1.70, 95% confidence interval: 1.37 to 2.11).
Conclusions
Deprivation and f-Hb are related. This has important implications for selection of cut-off f-Hb for screening programmes, and supports the inclusion of deprivation in risk-scoring systems.
Introduction
There is a well-established relationship between deprivation (socio-economic status) and overall cancer incidence, and deprivation has an impact on a number of outcomes in those with colorectal cancer (CRC). Using guaiac-based faecal occult blood tests (gFOBT) in CRC screening programmes, considerable evidence accumulated that deprivation is associated with a high positivity rate, low uptake, and lower acceptance of colonoscopy.1–3 However, gFOBT have many disadvantages 4 , and faecal immunochemical tests (FIT) for haemoglobin are now considered the best non-invasive tests for CRC screening. 5 One of the major merits of quantitative FIT is that faecal haemoglobin concentrations (f-Hb) can be estimated.
In our recent assessment of FIT as a first-line test in Scotland 6 , we documented that use of FIT narrowed current gaps in uptake for sex, age, and deprivation in a bowel cancer screening programme. 7 We found that f-Hb increased with age in both sexes, and was higher in men than in women. 8 We suggested that these data were vital considerations for screening programme design, more tailored strategies were needed, and f-Hb could be included in individual risk-scores, along with sex and age. Because deprivation is of considerable relevance to CRC, including its effect on uptake and positivity rates in screening programmes, we investigated the relationship between deprivation and f-Hb.
Methods
The FIT as a first-line test evaluation has been described previously. 6 All eligible individuals aged 50 to 74 were sent an invitation pack which contained one specimen collection device (Eiken Chemical Co., Tokyo, Japan). Potential pre-analytical sources of variation were minimized by strict adherence to protocols, as described previously. 8 On return to the Laboratory, receipt of a specimen was captured electronically by the Scottish Bowel Screening System through a barcode. Sex and age were derived from the bar-coded CHI number, the 10-digit number used through the health care system in Scotland. Deprivation was categorized from individual postcodes using the Scottish Index of Multiple Deprivation (SIMD), which identifies small area concentrations of multiple deprivation based on income level, employment, health, education, skills and training, housing, geographical access, and crime. Estimation of f-Hb was as described in detail previously in accordance with published guidelines on FIT evaluation reporting (FITTER). 9 The barcode labelled specimen collection tubes were assayed on one of two OC-Sensor Diana analyzers (Eiken Chemical Company, Tokyo, Japan). The distributions of f-Hb were calculated overall and for men and women in deprivation quintiles, and a number of properties 8 were examined. MedCalc (MedCalc Software, Mariakerke, Belgium) statistical software was used for all calculations. It has been proposed that all FIT data be expressed as µg Hb/g faeces, and a multiplier can be applied to each analytical system: 10 for the OC-Sensor Diana, ng Hb/mL buffer data are multiplied by 0.2.
Results
Percentiles (with 95 % CI) of faecal haemoglobin concentrations (ng haemoglobin/mL buffer) in men and women according to deprivation quintile.
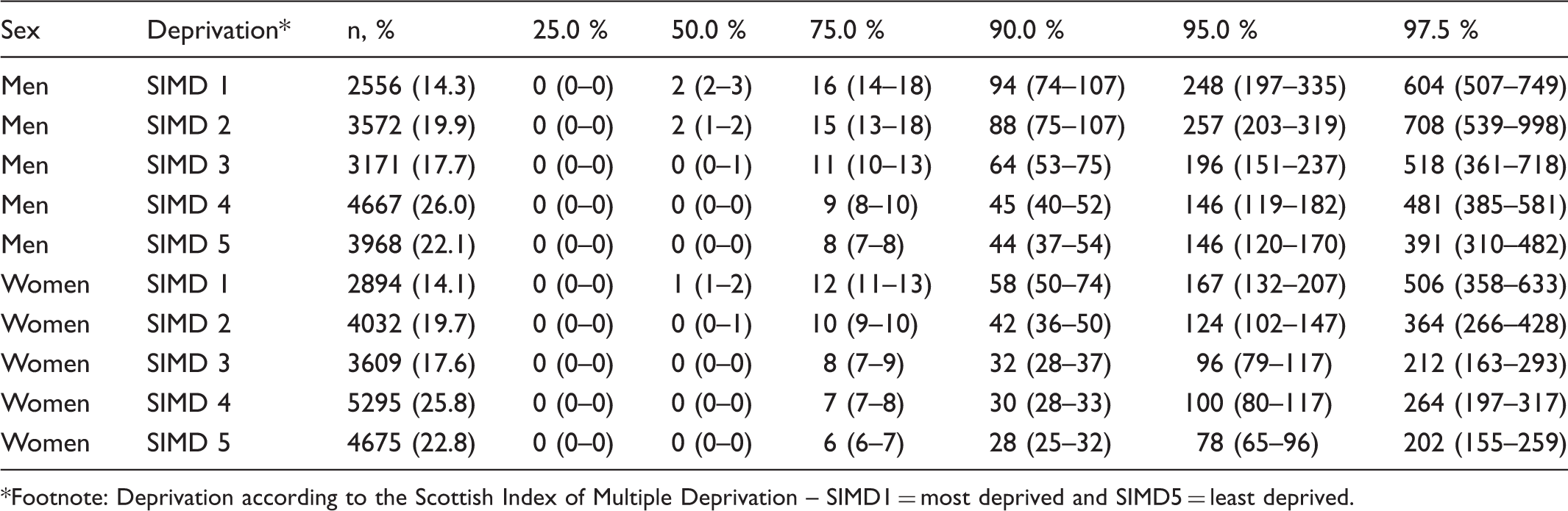
Footnote: Deprivation according to the Scottish Index of Multiple Deprivation – SIMD1 = most deprived and SIMD5 = least deprived.
Krusall-Wallis non-parametric analysis of variance (ANOVA) showed that highly statistically significant variation existed in f-Hb in both sexes across deprivation quintiles (p < 0.000001), with f-Hb increasing as deprivation increased. Those in the most and second most deprived quintiles had significantly higher f-Hb than those in each of the three remaining less deprived quintiles (p < 0.001).
The positivity rate with the previously used f-Hb cut-off of 400 ng Hb/ml 6 would range from 1.96% in the least deprived up to 3.21% in the most deprived overall, and would be higher in men than in women. Logistic regression analysis showed that participants in the most deprived quintile were more likely to have a f-Hb above this cut-off for positivity, compared with the least deprived quintile, independent of gender or age (adjusted odds ratio: 1.70, 95% CI: 1.37 to 2.11).
Detection of advanced colorectal neoplasia (defined as cancer or high-risk adenoma (>3 or any >1 cm diameter)) in participants with f-Hb above the cut-off concentration adopted was examined. The odds ratios rose with each increasing deprivation quintile compared with the least deprived (adjusted odds ratio: 1.48, 95% CI: 0.99–2.22).
Discussion
We examined deprivation and f-Hb in a large group of ostensibly asymptomatic people aged 50 to 74. Men had higher concentrations than women in all deprivation quintiles. As degree of deprivation increased, f-Hb overall and in both men and women increased, showing that the mechanisms driving this relationship do not appear to be gender-specific.
The relationship between f-Hb and deprivation is reflected by a higher proportion of participants with f-Hb above the cut-off used in our evaluation 6 in those in the more deprived groups. As increasing f-Hb relates to severity of colorectal disease, it is important to determine whether increasing deprivation was indeed associated with higher rates of advanced neoplasia detection in our cohort, when controlling for the effects of age and gender, or a greater prevalence of false-positive results were seen in the more deprived groups. Although the trend of increasing odds of advanced neoplasia detection with increasing degree of deprivation did not quite reach significance, it came very close, and this perhaps is sufficient to merit at least the consideration of degree of deprivation for inclusion in risk-scoring systems.
Conclusions
A clear relationship exists between degree of deprivation and f-Hb. Although this relationship is likely to be related to lifestyle factors associated with increasing deprivation, for example, poorer diet and increased tobacco smoking, further work is warranted to investigate the mechanisms. With an association existing between deprivation and increased CRC incidence and poorer outcomes, our data further highlight the need to consider adoption of better strategies for setting f-Hb cut-offs. Our findings show that there is potential for deprivation to be included, along with f-Hb, sex, and age, in the risk-scoring systems that are of ever-growing interest.
Footnotes
Declaration of interests
CGF has consultancy relationships with Immunostics Inc and Mode Diagnostics and has received travel funding from Alpha Labs Ltd: all other authors have no competing interests.
Acknowledgements
We thank Iain McElarney of Mast Diagnostics Division, Bootle, Merseyside, UK, for his input into the preparation of material for potential participants and the setting up of the data capture for the automated analytical systems.
Funding
The additional resources required to undertake the FIT as a first-line test evaluation were provided in part by the Scottish Government Health Directorates. Data analysis was in part supported by a grant from the Chief Scientist Office (grant no. CZH/6/4) to establish a Bowel Screening Research Unit. JD was supported by Tenovus Scotland. These sponsors had no role in the collection, analysis, or interpretation of data or in the writing of the report. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. All authors are independent of the funders in terms of freedom to publish.
Ethics approval
Ethics approval was not required for the FIT as a first-line test evaluation. Ethics approval to collect data additional to that generated in the Scottish Bowel Screening Programme was granted by NHS Tayside Ethics Committee and West of Scotland Research Ethics Service. The work was approved by the Scottish Bowel Screening Programme Board and had Caldicott Guardian approval from both NHS Tayside and NHS Ayrshire & Arran.