
Abstract
Objective
To examine associations between faecal haemoglobin concentrations below the cut-off used in colorectal cancer screening and outcomes in the next screening round.
Methods
In the Scottish Bowel Screening Programme, faecal haemoglobin concentrations and diagnostic outcomes were investigated for participants with a negative result (faecal haemoglobin concentrations < 80.0 µg Hb/g faeces), followed by a positive result within two years.
Results
Of 37,780 participants with negative results, at the next screening round, 556 (1.5%) screened positive and 30,293 (80.2%) negative. Initial median faecal haemoglobin concentrations (2.1 µg Hb/g faeces, IQR: 0.0–13.2) were higher in those with subsequent positive results than those with subsequent negative results (0.0 µg Hb/g faeces, IQR: 0.0–1.4; p < 0.0001). Using faecal haemoglobin concentrations 0.0–19.9 µg Hb/g faeces as reference, logistic regression analysis showed high adjusted odds ratios for advanced neoplasia (advanced neoplasia: colorectal cancer or higher risk adenoma) detection at the next round of 14.3 (95% CI: 8.9–23.1) in those with initial faecal haemoglobin concentrations 20.0–39.9 µg Hb/g faeces, and 38.0 (95% CI: 20.2–71.2) with 60.0–79.9 µg Hb/g faeces.
Conclusions
A higher proportion of participants with faecal haemoglobin concentrations of ≥ 20 µg Hb/g faeces had advanced neoplasia detected at the next round than participants with lower faecal haemoglobin concentrations. Although most relevant when using high faecal haemoglobin concentrations cut-offs, studies of faecal haemoglobin concentrations and outcomes over screening rounds may provide strategies to direct available colonoscopy towards those at highest risk.
Keywords
Introduction
In colorectal cancer (CRC) screening programmes, participants with faecal haemoglobin concentrations (f-Hb) below the selected cut-off for positivity and referral for follow-up colonoscopy, as determined by a quantitative faecal immunochemical test (FIT) for haemoglobin (Hb), are more likely to be diagnosed with an interval cancer (IC) than those with undetectable f-Hb. 1 Establishing the relationship between a detectable f-Hb below the programme selected cut-off, and diagnostic outcome in the longer term could assist in determining the role of f-Hb as a predictor of the future risk of advanced neoplasia (AN), defined as CRC plus higher risk adenoma (HRA).
Two previous studies from Taiwan are relevant. Firstly, 2 a cohort of 44,324 CRC screening participants aged 40–69, with f-Hb below the cut-off of ≥ 20.0 µg Hb/g faeces, was followed for a median of 4.39 years. The incidence of AN rose from 1.75/1000 person-years for those with f-Hb of 0.2–3.9 µg Hb/g faeces to 7.08/1000 in those with f-Hb of 16.0–19.9 µg Hb/g faeces. Relative to those with f-Hb of 0.2–3.9 µg Hb/g faeces, adjusted hazard ratios (HR) for AN were calculated as 3.41 for those with f-Hb in the category lower than but closest to the cut-off f-Hb used (16.0–19.9 µg Hb/g faeces). The second study used regression modelling to further establish the value of f-Hb as a predictor for colorectal neoplasia 3 ; 54,921 participants invited between 2001 and 2007 were followed up in the Taiwanese annual FIT-based CRC screening programme to identify those diagnosed with IC, screen-detected CRC and adenoma. A trend of increasing HR with increasing baseline f-Hb was demonstrated for colorectal neoplasia, including for those with f-Hb above the traditionally used cut-off of ≥ 20 µg Hb/g faeces.
The available limited evidence indicates that the higher the baseline f-Hb, the greater the likelihood of a future finding of AN. If verified, this could have implications for the design and execution of CRC screening programmes. For example, those with a negative screening test result, who are at high risk of having AN by virtue of a detectable f-Hb, despite being lower than the cut-off f-Hb applied, could be prioritised for future repeat screening at a shorter interval than the current usual annual or biennial invitation. Conversely, those with undetectable f-Hb, and therefore deemed very unlikely to have a future finding of AN, could require less frequent invitations to screening. Such a strategy could be an important consideration in countries such as Scotland where, in view of demands on the colonoscopy resource, adoption of a cut-off f-Hb of ≥ 80.0 µg Hb/g faeces (equivalent to ≥ 400 ng Hb/ml buffer) for the planned FIT-based programme is likely, given that this was used in the pilot evaluation required to inform future adoption of FIT as a first-line test. 4 This f-Hb cut-off was selected to achieve approximately 2% positivity, to mimic the current screening algorithm based on a two-tier reflex guaiac faecal occult blood test (gFOBT)/qualitative FIT strategy. 4 As ICs are common at this f-Hb cut-off, 1 it is reasonable to postulate that a proportion of participants with f-Hb < 80.0 µg Hb/g faeces will have AN detected at the next screening round. We therefore aimed to investigate the relationship between f-Hb reported as a negative screening test result in our FIT evaluation and diagnostic outcomes identified over the two-year period of the next screening round, to test the hypothesis that those with f-Hb lower than but closer to the cut-off applied are more likely to be subsequently diagnosed with AN.
Methods
Outside the setting of the FIT evaluation, the Scottish Bowel Screening Programme (SBoSP) uses a two-tier reflex gFOBT/FIT screening algorithm (previously described). 4 The pilot evaluation using FIT as a first-line screening test in Scotland has also been previously described. 5 All participants with f-Hb ≥ 80.0 µg Hb/g faeces were reported as positive and offered colonoscopy.
Following completion of the FIT evaluation, the SBoSP returned the two NHS Boards involved (NHS Tayside or NHS Ayrshire and Arran) to the two-tier reflex gFOBT/FIT screening algorithm. The screening test results for all those eligible to take part in the two years of the next screening round after the FIT evaluation (13 January 2011 to 12 January 2013) and resident in either NHS area were examined. The f-Hb from the previous FIT-based pilot evaluation round for those with a positive gFOBT/FIT screening test result was retrieved from the Scottish Bowel Screening IT System. Data for colonoscopy outcomes and any subsequent pathology for those with a positive test result were downloaded from the clinical IT systems in two NHS Board areas. Data on colonoscopy findings, including number, size, Dukes’ stage and localisation of CRC and adenomas were collected. As in the SBoSP, HRAs were defined as adenomas > 10 mm in diameter, or when there were three or more adenoma present. 6 AN was defined as CRC and HRA.
MedCalc (MedCalc Software, Mariakerke, Belgium) statistical software was used for all calculations. The Mann-Whitney U test was used for comparison of median f-Hb between classes. Probability of p < 0.05 was considered significant. Logistic regression analysis was performed to calculate odds ratios (OR) for diagnosis of AN at the next screening round amongst those in different f-Hb classes and different demographic groups, both adjusted and unadjusted for age and gender as known confounding variables.
This study was approved by the Programme Board, SBoSP. Ethical approval was not required.
Results
Number of participants with a negative FIT screening test result and their screening test results in two years in the next gFOBT/FIT screening round.
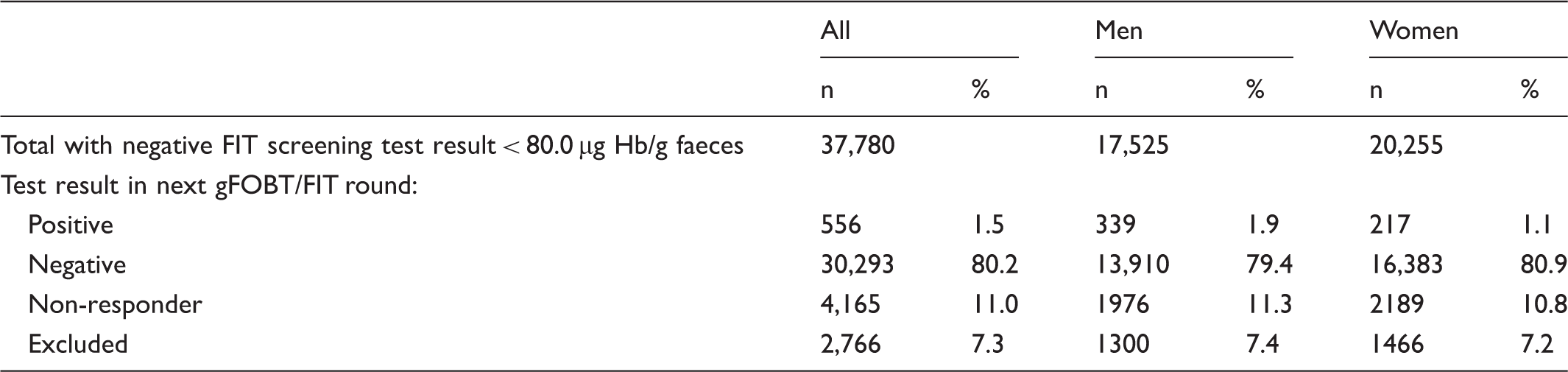
There were 556 (1.5%) participants with a positive result and 30,293 (80.2%) with negative results in the subsequent screening round. The initial median f-Hb was statistically significantly higher in those who then had a positive test result in the next round than in those who remained negative (2.1 µg Hb/g faeces, IQR 0.0–13.2 vs. 0.0 µg Hb/g faeces, IQR 0.0–1.4; p < 0.0001).
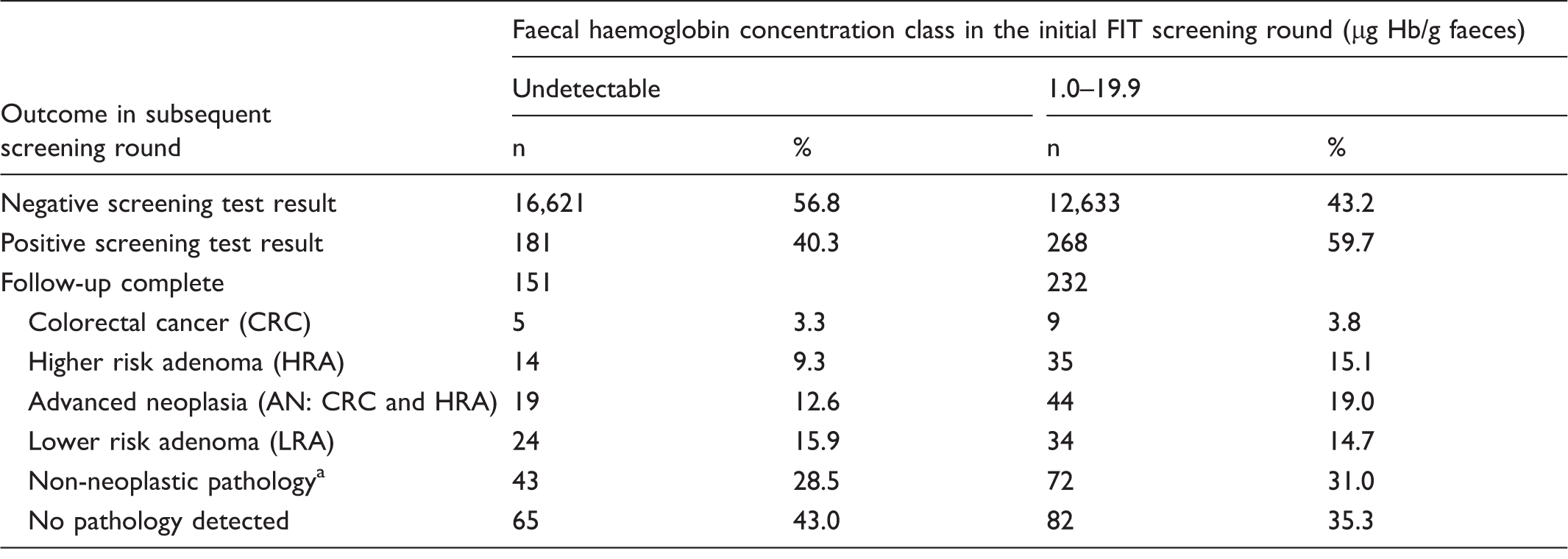
Diagnostic outcomes and median faecal haemoglobin concentrations (f-Hb) at the initial FIT screening round in participants then having a positive screening test result at the next gFOBT/FIT screening round.
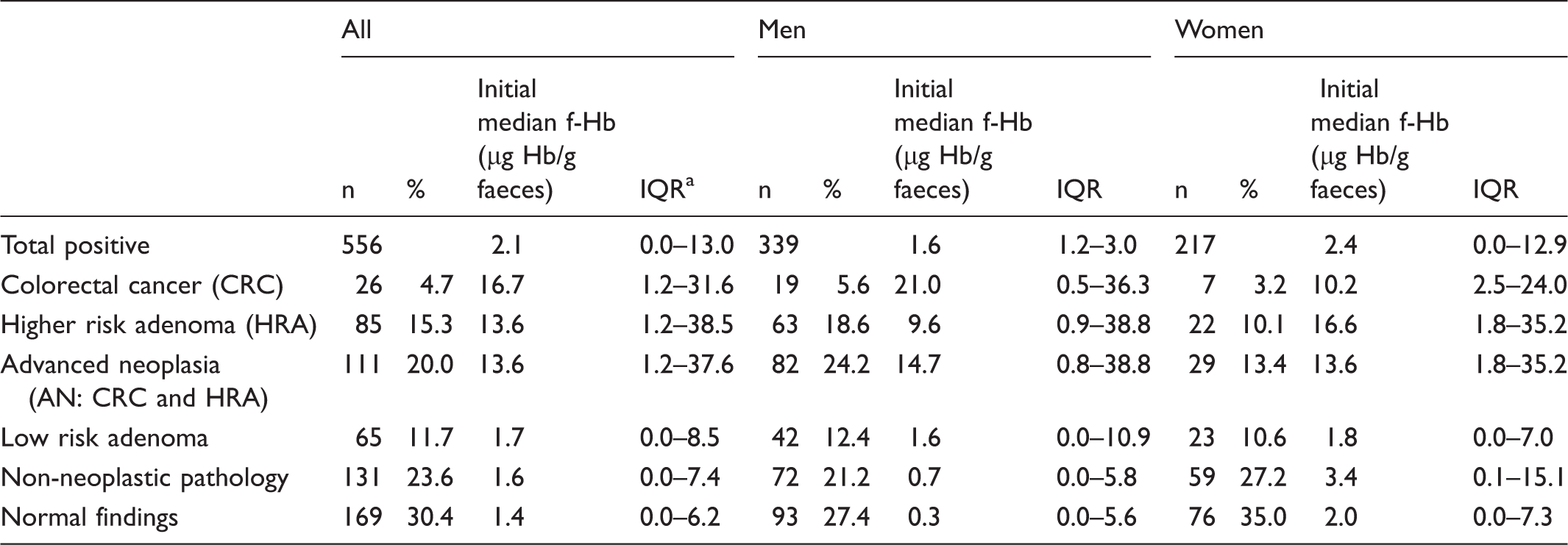
IQR is the interquartile range (difference between the upper quartile and the lower quartile); non-neoplastic pathology comprises conditions including diverticular disease, haemorrhoids and inflammatory bowel disease and haemorrhoids.
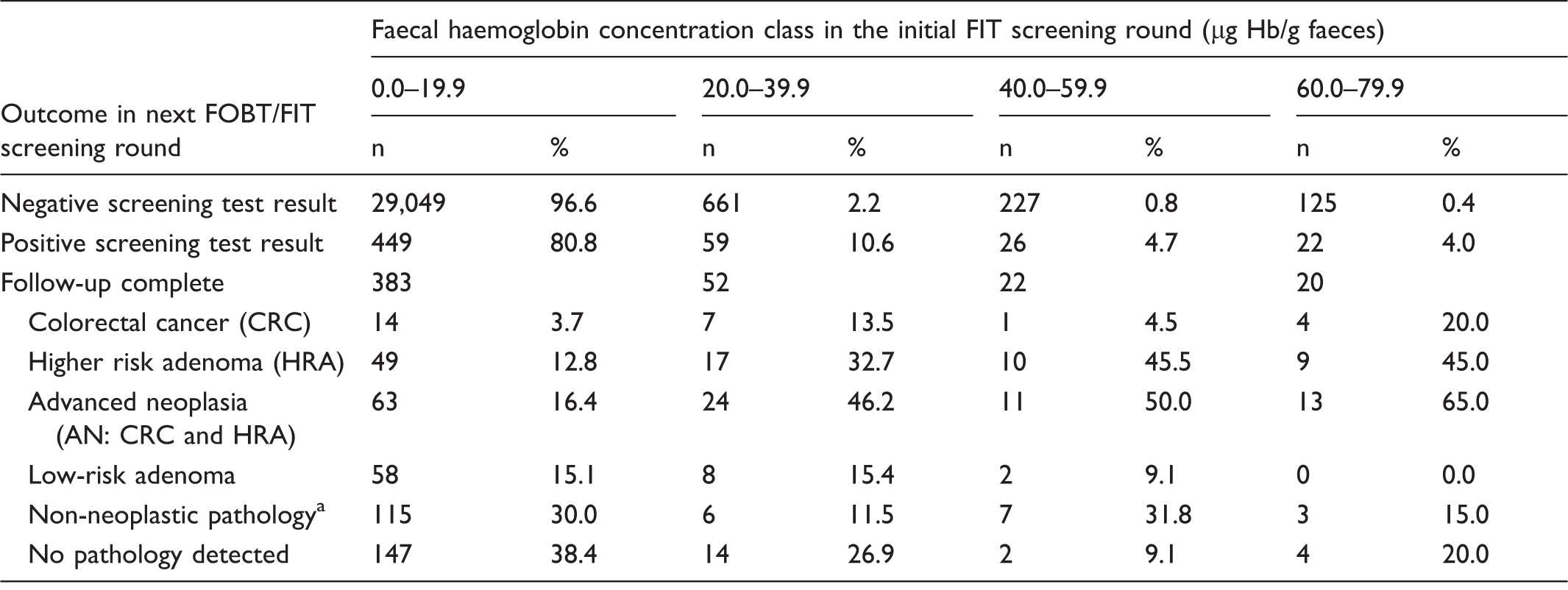
A numerical f-Hb result was available for 30,823/30,849 participants in both screening rounds. In the majority of these (96.6%), f-Hb in the FIT round was in the lowest class of 0.0–19.9 µg Hb/g faeces; 87.4% of participants with a positive gFOBT/FIT result who did not have AN detected were in this low f-Hb class, compared with only 56.8% of those with AN. Table 3 shows the proportions of participants with different diagnostic outcomes according to class of f-Hb at the initial screening round with FIT. A lower proportion of participants with previously low f-Hb had AN detected than less severe outcomes, but this trend reversed with rising f-Hb (see Figure 1). A commonly used f-Hb cut-off for screening programmes outside Scotland is ≥ 20 µg Hb/g faeces. Table 4 shows further analysis of the class with f-Hb below this concentration, dissected into two f-Hb classes: those with undetectable f-Hb at the initial FIT screening round and those with f-Hb 1.0–19.9 µg Hb/g faeces.
Percentages of FIT positive screening participants completing follow-up who had advanced neoplasia or less severe outcomes in the next gFOBT/FIT screening round, according to faecal haemoglobin concentration (f-Hb) class. Outcomes of participants in both screening rounds according to faecal haemoglobin concentration class at the initial FIT screening round. Non-neoplastic pathology comprises conditions including diverticular disease, haemorrhoids and inflammatory bowel disease and haemorrhoids. Outcomes of participants of both screening rounds with faecal haemoglobin concentration < 20 µg Hb/g faeces at the initial FIT screening round, dissected into two classes. Non-neoplastic pathology comprises conditions including diverticular disease, haemorrhoids and inflammatory bowel disease and haemorrhoids.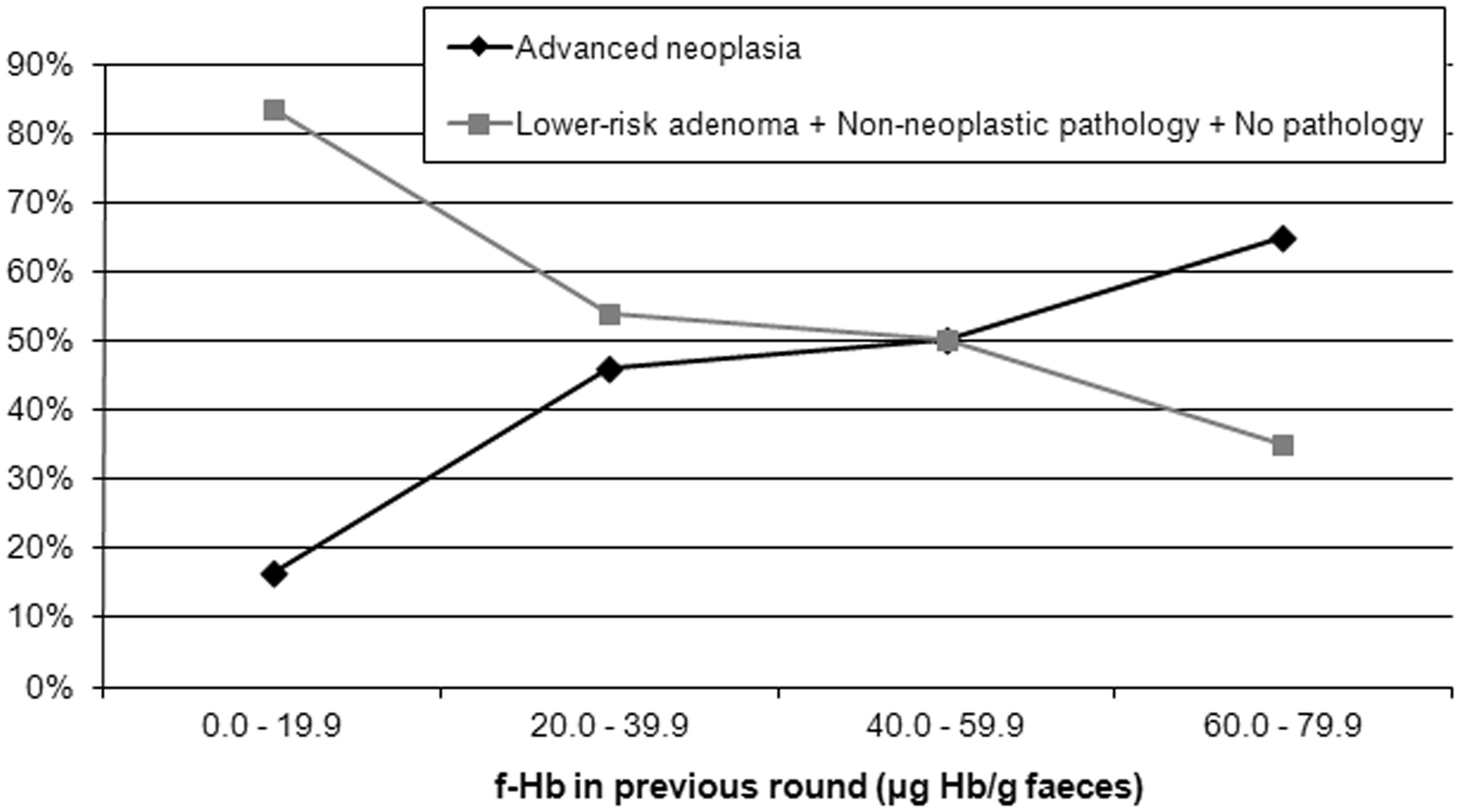
Odds ratios (both unadjusted and adjusted for age and gender) for advanced neoplasia (AN) found at the next gFOBT/FIT round after a positive screening test result, according to faecal haemoglobin concentration (f-Hb) class in the previous FIT screening round.
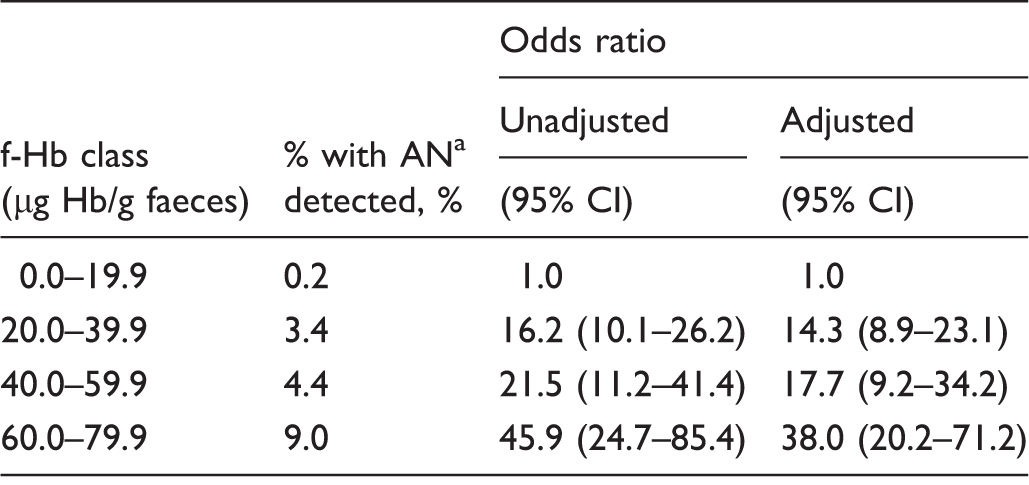
Advanced neoplasia (AN) includes colorectal cancer and higher risk adenoma.
Discussion
A higher proportion of participants with a previous f-Hb lower than, but approaching, the cut-off used in our FIT pilot evaluation had AN detected at the next round than participants with low f-Hb. This provides further evidence that f-Hb is a strong predictor of future risk.
Positivity in participants with a previous round f-Hb below the applied cut-off of ≥ 80.0 µg Hb/g faeces was 1.5%. This was lower than either the overall positivity seen in the Scottish FIT pilot evaluation 7 or the current gFOBT/FIT algorithm at ca.2%. 4 This suggests that participants with a previously negative screening test result, even with a relatively high cut-off f-Hb, are less likely to have a positive test result in the subsequent screening round than the overall population (including first-time participants and participants with a previous positive test result) invited for screening.
Our findings further support the concept of f-Hb being a valuable predictor of risk of AN, as f-Hb was statistically significantly elevated, not only in those who would have a positive test result in the next round compared with those who again had a negative result but also in those who had AN detected at follow-up investigations compared with those with no pathology (both p < 0.0001). One in five participants with f-Hb in the f-Hb range nearest to the cut-off applied who were then positive in the next screening round were diagnosed with CRC. This compares with 1 in 27 participants in the lowest f-Hb class examined. Those with elevated f-Hb who go on to have a positive screening test result in the next round are over five times more likely to have CRC detected. When also taking into account detection of HRA, 65% of participants with a positive screening test result who previously had f-Hb in the highest f-Hb class examined had any AN diagnosed, compared with just 16.4% in the lowest. There is also a trend of a higher proportion of AN in participants from each of the four classes of increasing f-Hb. From these data, the odds of having AN detected following a positive screening result are even in those with previous f-Hb between 40.0 and 59.9 µg/g faeces. After this point, it is more likely than not that AN will be present at follow-up investigations in those with a positive screening test result in the next round. Almost one-tenth of all participants with f-Hb approaching the cut-off f-Hb applied went on to have AN detected, representing a 40-fold increase in the risk compared with those in the lowest f-Hb class. This finding is important when considering f-Hb as a predictor of future risk of AN at the time of a negative screening test result. Strong evidence is provided not only for the value of f-Hb as a risk factor for AN being detected at follow-up investigations of participants going on to have a positive test result but also for predicting future positivity and the subsequent detection of AN. As it has been suggested that f-Hb is a predictor not only of CRC mortality but also of all-cause death, 8 there may be other benefits in the more general application of f-Hb as a predictor of ill health.
Figure 1 shows a graph that could be used to determine the effect of cut-off f-Hb on yield of AN for screening programmes collecting data such as these, irrespective of the faecal test used. The f-Hb, where the percentage of participants with positive screening results completing follow-up who had AN crosses that of those less severe outcomes, can indicate the cut-off f-Hb associated with the greatest benefit in terms of yield of AN, although this only includes participants with a positive result at the next screening round, not those with negative subsequent results. CRC FIT screening programmes use a wide range of f-Hb cut-offs, and that used by the SBoSP FIT evaluation was much higher than most. Our data allow some comparison of strategies using lower f-Hb cut-offs. Combining the data presented here with those in our recent publication on IC arising in the pilot evaluation of FIT screening, 1 if Scotland used a cut-off of ≥ 60.0 µg Hb/g faeces rather than the ≥ 80.0 µg used in the FIT evaluation, 4 then 25.6% additional colonoscopy would yield 20.0% more CRC, or at least possible precursor lesions, presuming these were present at the time of the FIT-based screening. However, in addition to the reduction in the number of false-negative screening test results, the number of false-positive results will also increase, requiring assessment of the associated harms, such as overdiagnosis of lesions that would never have become symptomatic, and the risk of complications of colonoscopy.
Further analysis was performed on clinical outcomes at the subsequent screening round of those with an initial f-Hb below the commonly used cut-off f-Hb ≥ 20 µg Hb/g faeces. With the prevalence of AN higher in those with f-Hb between 1.0 and 19.9 µg Hb/g faeces than in those with undetectable f-Hb, evidence is provided that f-Hb is a predictor of future risk of colorectal neoplasia, even at a lower f-Hb cut-off than that used in Scotland.
As it is well accepted that men have higher median f-Hb than women,9,10 it is surprising that the median initial f-Hb of participants with a positive screening test result at the next round was higher (although not statistically significantly so) in women than in men. Significantly higher median initial f-Hb was detected in women compared with men in those with non-neoplastic pathology, or normal findings at colonoscopy triggered by a positive screening test result at the next screening round. Men who had a false-positive screening test result appeared to be more likely to have had a low f-Hb in the previous screening round before experiencing short-term colonic blood loss to trigger their subsequent positive screening test result. Women, however, may have had longer term colonic bleeding, rising over time. The reasons for this are unclear and may be worthy of further study. Although not statistically significant, median f-Hb of participants with CRC detected at the next screening round was higher in men than in women, but the opposite was apparent for HRA. The previous median f-Hb for women with CRC was very similar to previous median f-Hb of men with HRA, further demonstrating the variation in f-Hb by gender as documented previously,9,10 which should be taken into account in setting cut-off f-Hb for any screening programme.
An obvious weakness of this analysis is that different tests were employed in the two screening rounds examined. However, the cut-off used in the quantitative FIT pilot evaluation was equivalent, in terms of positivity, to the current gFOBT/FIT algorithm, to which the programme reverted. It would be of interest to conduct a similar study in which quantitative FIT was used in consecutive screening rounds, to allow investigation of the variation in f-Hb over time according to diagnostic outcomes. In addition, the number of CRC cases is low, limiting detailed analysis by sub-groups such as age, gender, and lesion site.
Two recent studies have compared clinical outcomes between two consecutive screening rounds with very large cohorts, allowing sub-analyses by gender and lesion site. A Spanish study showed that the second screening round was associated with lower median f-Hb and an increased proportion of proximal CRC. 11 The authors suggested various strategies to improve diagnosis of proximal CRC, such as using a lower cut-off f-Hb at the first compared with the second round. A French study has demonstrated that subsequent screening was associated with increased detection of proximal AN, particularly in women, and CRC was more often later stage. 12 It was concluded that, as the late stage CRC was likely to be previously missed lesions, the findings stressed the importance of repeated screening after a previous negative test result. These studies demonstrate the scope that exists for further work into the relationship between f-Hb and outcomes in subsequent screening rounds according to various sub groups, if working with a large enough sample size.
Our data could have an impact on CRC screening strategies. Risk scoring models are becoming increasingly developed, with an escalation in published studies in recent years.13–22 We have confirmed that f-Hb predicts the presence of colorectal disease, through analysis of positivity in the next screening round. Screening programmes using FIT and considering the application of risk-scoring should incorporate f-Hb into such models, along with age and gender, and perhaps deprivation, 23 to improve their predictive power. The fact that f-Hb is related, not only to colorectal disease severity, 24 but also to future risk, has important implications for FIT-based CRC screening strategies.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CGF undertook consultancy with Immunostics Inc., Ocean, NJ, USA, Mode Diagnostics, Glasgow, Scotland, and Kyowa-Medex, Tokyo, Japan.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Chief Scientist Office of the Scottish Government Health Department. Project: Establishing a Bowel Screening Research Unit (Grant Ref: CZH/6/4). JD was supported from a grant from Tenovus Tayside.