
Abstract
Objective
There is evidence that colorectal cancer screening using faecal haemoglobin is less effective in women than men. The faecal haemoglobin concentrations were therefore examined in women and men with screen-detected colorectal cancer.
Setting
Scottish Bowel Screening Programme, following the introduction of a faecal immunochemical test from November 2017, to March 2020
Methods
Data were collated on faecal haemoglobin concentrations, pathological stage and anatomical site of the main lesion in participants who had colorectal cancer detected. The data in women and men were compared.
Results
For the faecal haemoglobin concentrations studied (
Conclusions
To minimise gender inequalities, faecal immunochemical test-based colorectal cancer screening programmes should evaluate a strategy of using different faecal haemoglobin concentration thresholds in women and men.
Keywords
Introduction
Screening for colorectal cancer (CRC) using the detection of faecal haemoglobin (f-Hb) creates gender inequality. Although women are consistently more likely to participate in faecal test-based screening strategies than men, the yield of neoplastic pathology is lower in women.1–3 For example, in the first year of the Scottish Bowel Screening Programme (SBoSP) after the introduction of a faecal immunochemical test (FIT) to determine the f-Hb concentration, 0.09% of all women (n = 307,919) and 0.15% of all men (n = 279,530) screened were diagnosed as having invasive CRC, and 0.36% of women versus 0.80% of men had higher risk adenomas. 2 These findings may be explained partially by the lower incidence of CRC in women, 4 and the tendency for CRC in women to be right-sided and, consequently, less amenable to detection using f-Hb. 5 However, there is now consistent evidence that women are more likely to present with interval CRC (i.e. CRC diagnosed within two years of a “negative” screening test result),6,7 indicating that screening using f-Hb is less sensitive for CRC in women than in men. In addition, there is strong evidence from trials of CRC screening based on f-Hb that the CRC mortality reduction gained is less in women than in men.8,9
To date, this evidence is largely based on the guaiac faecal occult blood test (gFOBT). However, these tests are considered obsolete
10
and screening programmes world wide,
11
including all in the United Kingdom, and many in Europe,
12
have replaced, or are replacing, the gFOBT with the FIT. Unlike the gFOBT, the FIT is specific for human haemoglobin (Hb) and can provide a quantitative estimate of the f-Hb concentration. It is known that in screening populations, and probably in the population at large, f-Hb concentrations are lower in women than in men,13,14 so that, for any given screening f-Hb concentration threshold, the positivity in women is lower than that in men. For example, in the first year of the FIT-based programme in Scotland, which uses a threshold of
However, this in itself does not explain the poorer CRC detection rates and higher interval cancer rates in women, and it would seem likely that the f-Hb concentrations in women with CRC would be lower than in men with comparable lesions. If this is the case, it would lend support to the view that f-Hb concentration thresholds for screening should be lower in women than in men, but, to our knowledge, this has not been studied to date.
We have therefore interrogated the data from the FIT-based SBoSP to determine the f-Hb concentrations in women and men detected with CRC, taking into account the anatomical location of the main lesion within the large bowel and the pathological stage.
Methods
Data analysis
As previously described,
2
the SBoSP began with three pilot screening rounds in three of the 14 National Health Service Boards in Scotland. The national roll-out of the SBoSP using a two-tier reflex gFOBT/qualitative FIT algorithm then began in 2007 and was complete by the end of 2009. This strategy was used until 2017 when FIT as a first-line test was introduced. Data from the SBoSP between the introduction of FIT in November 2017 and March 2020 were used for this study. Of those who had “positive” test results (i.e. with an f-Hb concentration
F-Hb concentration determination
The logistics involved in the FIT-based SBoSP have been described in detail previously.
2
In brief, participants in the SBoSP returned the completed FIT specimen collection device by post to the Scottish Bowel Screening Laboratory (Ninewells Hospital and Medical School, Dundee). Analyses were carried out from Monday to Friday; most devices were analysed on the day of receipt and the f-Hb results were reported electronically to the Scottish Bowel Screening System (BoSS) after f-Hb concentration measurement using one of four HM-JACKarc (Hitachi Chemical Diagnostics Systems, Tokyo, Japan) FIT systems. The Laboratory has ISO (International Organization for Standardization) 15,189 accreditation. Total quality management is comprehensively practised, including internal quality control and external quality assessment carried out by the UK National External Quality Assessment Scheme (UKNEQAS). Use of data outside the analytical measurement range documented by the manufacturer, which is 7–400 µg Hb/g faeces for the FIT system used in this study, has become usual for research as well as clinical purposes at low f-Hb concentrations below the limit of detection, and this approach has been supported in the peer-reviewed literature.
16
We have adopted an analogous strategy through examination of all results
Statistical analyses
Statistical significance for the difference in f-Hb concentrations between women and men was assessed using the Wilcoxon Rank Sum test; p-values were considered significant at the 0.05 level. R statistical software v3.6.1 was used for all data processing and analysis. 17
Results
Table 1 shows the median f-Hb concentrations, percentages of results with f-Hb concentration
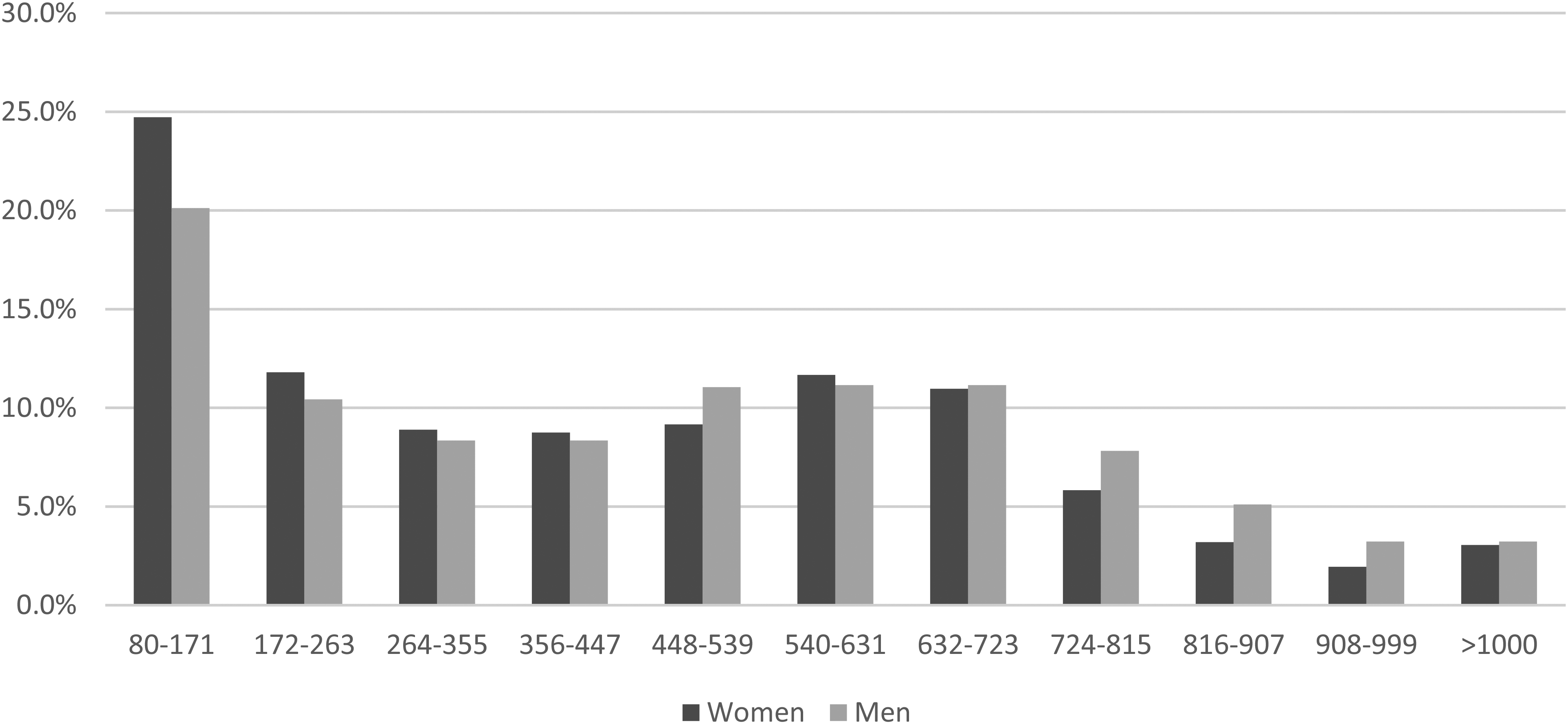
Percentages of women and men with screen-detected colorectal cancer by faecal haemoglobin concentration class (µg Hb/g faeces).
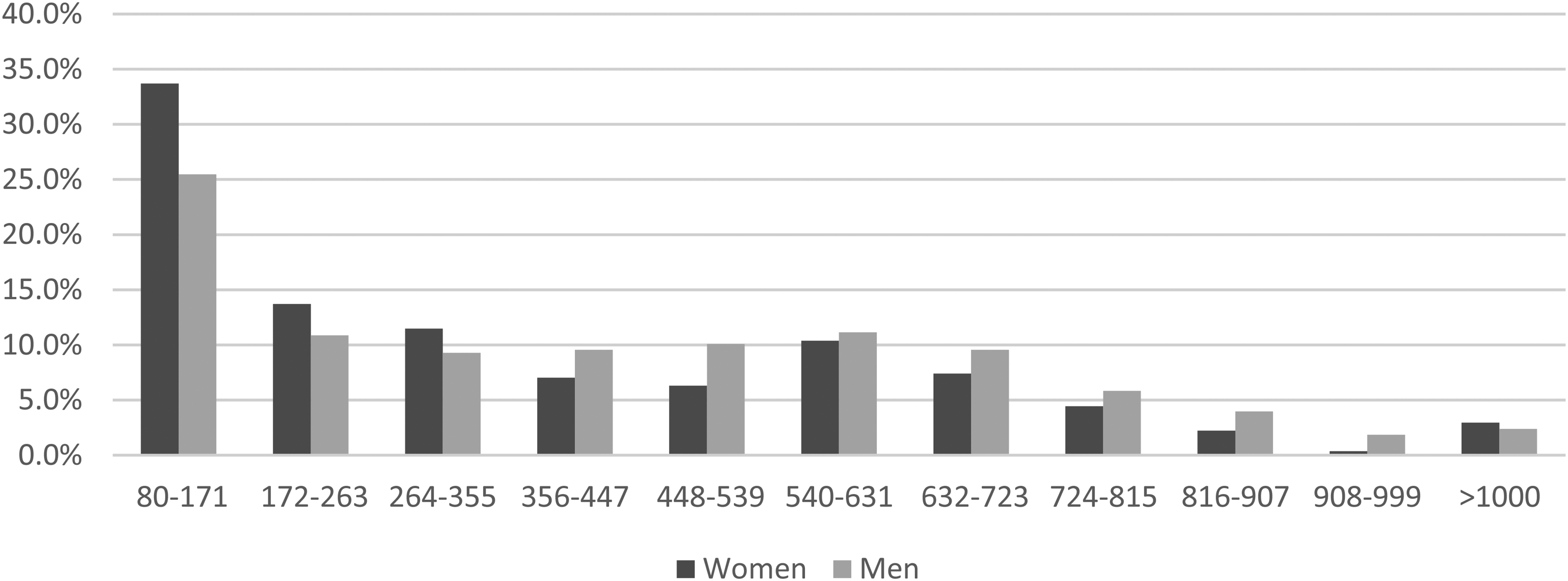
Percentages of women and men with stage I screen-detected colorectal cancer by faecal haemoglobin concentration class (µg Hb/g faeces).
Median faecal haemoglobin concentration (faecal haemoglobin (f-Hb), µg Hb/g faeces), percentage with faecal haemoglobin concentration
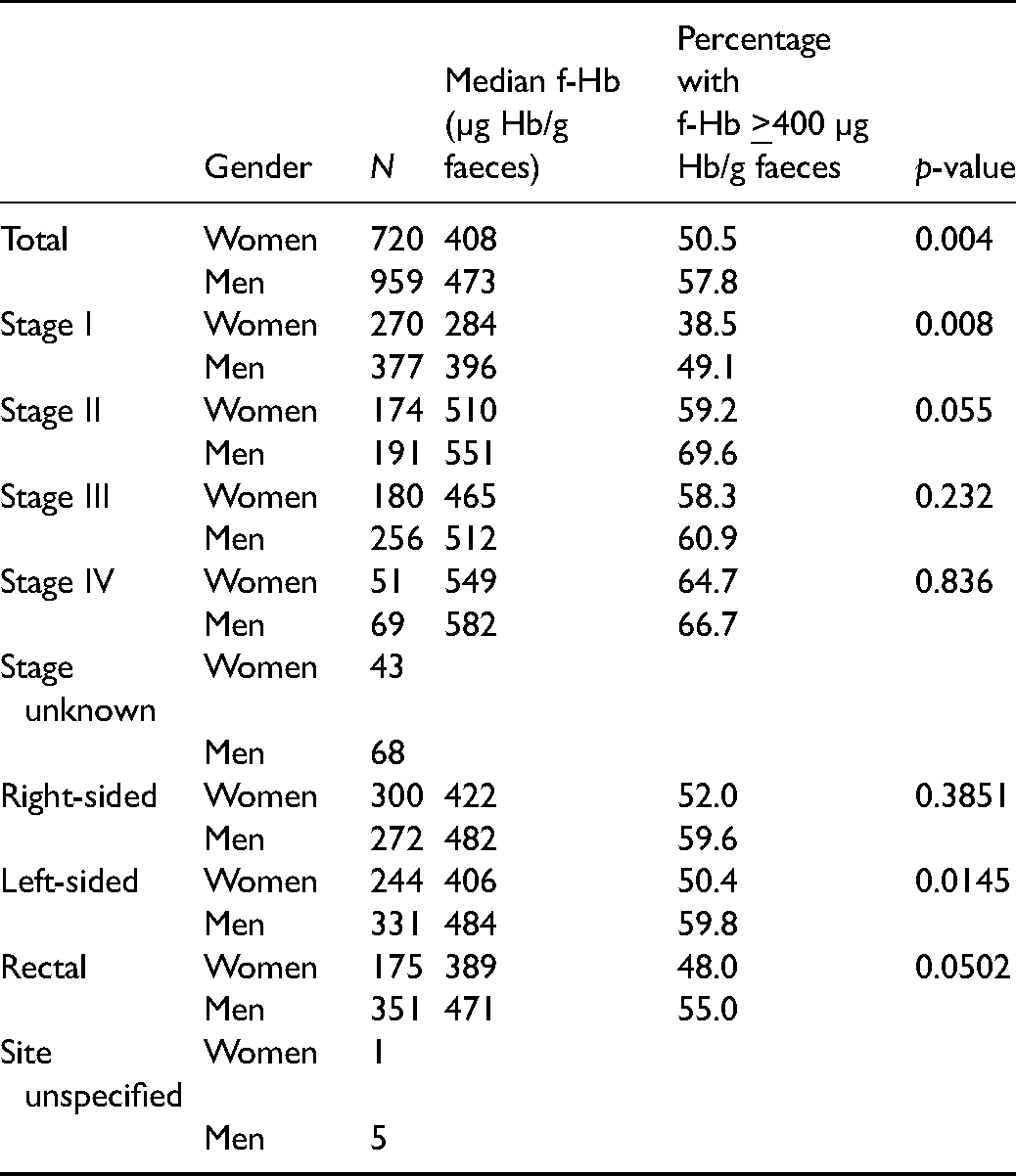
The median f-Hb concentration for all screen-detected CRC women was 408 µg Hb/g faeces compared to 473 µg Hb/g faeces for men (p = 0.004) and 50.6% of the results were
Discussion
Since women do have lower f-Hb concentrations than men,13,14 it is not surprising that, in screening programmes based on the use of a single f-Hb concentration threshold, positivity is found to be lower in women than in men. What is less easy to explain is the lower CRC detection rate, the higher interval cancer rate, and the smaller effect of screening on CRC-specific mortality, since it might be expected that CRC would bleed to the same extent in women and men. Thus, the explanations of a lower CRC incidence and more right-sided lesions in women than men are attractive, although a previous analysis of a FIT-based screening pilot in Scotland has indicated that interval cancers were more common in women irrespective of anatomical site. 5
This issue is clarified by the findings presented here which indicate that stage for stage and site for the site within the large bowel, CRCs are associated with lower f-Hb concentrations in women than in men. This could be explained by the lower background f-Hb concentration in women, such that a CRC would have to bleed more in a woman than a man to render the f-Hb concentration above the pre-determined threshold that triggers a further investigation, usually a colonoscopy. It is interesting that the difference between women and men becomes less with more advanced CRC. This may be related to sample size, since early CRCs are more common in a screening programme than the later disease as evidenced by the data presented here. However, an alternative explanation might be that because more advanced CRCs bleed more than early cancers, the effect of differential background f-Hb concentrations is reduced. Given that the mortality advantage of screening is dependent on the detection of early disease, the large difference between women and men in early disease that we have observed is of particular significance.
Why women have lower f-Hb concentrations than men is by no means clear. Blood Hb concentrations tend to be lower in women than men, and it has been suggested that f-Hb concentrations could mirror this; however, this seems implausible given the age range invited for screening (50–74 years) and that the small difference disappears a few years after the menopause. 18 Another possibility is related to the intrinsically lower bowel transit times in women, 19 and it is, therefore, possible that degradation of f-Hb before defaecation occurs to a greater extent in women than in men. Similarly, more degradation of any f-Hb present in women as compared to men could be due to slower transit caused by constipation, much common in women than men. 20 An alternative explanation is presented by the observation that f-Hb is related to death from multiple causes unrelated to CRC 21 and to the prescription of medicines that do not cause gastrointestinal bleeding for a range of conditions including heart disease, hypertension, depression, and type two diabetes. 22 Since these conditions all have an inflammatory component, it has been hypothesised that f-Hb is an index of systemic inflammation21,22 but, whatever the reason, f-Hb is a marker for poor health. Thus, an intriguing possibility is that, in participants who have detectable f-Hb but no significant disease on colorectal visualisation, such f-Hb identifies those who are at a high risk of harbouring or developing chronic conditions. 22 In Scotland, it is well established that women have a healthier lifestyle than men and they are also less likely to suffer from chronic non-communicable diseases. 23 Thus, the lower f-Hb in women may reflect less systemic inflammation in women than in men.
Whatever the explanation for the findings presented in this communication, employing a lower f-Hb concentration threshold for women than for men should alleviate the current gender inequality, since this is highly likely to bring the CRC detection and interval cancer rates in women more in line with those in men. This would, of course, generate an increased number of colonoscopies for women and there is also a concern that, since the positive predictive value (PPV) falls with decreasing f-Hb concentration thresholds,
24
and since the PPV is lower in women than in men in gFOBT screening,
6
there might be a significant burden of “false positive” test results in women. However, recent Scottish data indicated that using FIT at an f-Hb concentration threshold of
CRC incidences vary from one country to another; f-Hb distributions also vary between countries 28 and even between regions of a small country like Scotland. 14 In addition, in FIT-based screening programmes, different f-Hb concentration thresholds are employed to take account of national colonoscopy capacities.11,12 Thus, the issue of whether or not partitioned f-Hb thresholds should be used for women and men can only be resolved by prospective, observational studies. The distributions of f-Hb concentrations in men and women with CRC, the newer data from Scandinavia,25,28 and other evidence on screening outcomes, as detailed above, indicate that lowering the f-Hb concentration threshold in women would increase the chances of detecting CRC in those participating in screening. However, there are areas of significant uncertainty and these include the extent to which CRC detection rates in women and men would converge, the effect on the PPV and the consequent harms of any increase in the false positive rate, the effect on interval cancer rates in women and the cost-effectiveness of this strategy.
Given the quantitative nature of the FIT used in the SBoSP and in most other programmatic CRC screening, it would be straightforward to set the screening threshold at different f-Hb concentrations for women and men. Data from the SBoSP indicates that a threshold of
Conclusions
To obviate the clear gender inequalities occasioned by using the same f-Hb concentration threshold for women and men, we urge all countries with national or regional FIT-based CRC screening programmes to evaluate a strategy of using different f-Hb concentration thresholds in women and men such that gender-related differences in positivity are eliminated. This would provide the evidence required to decide whether or not a gender-based approach is effective in a country- or region-specific CRC screening programme. This simple approach could be a first step to the initiation of stratified approaches to CRC screening, such as those recently advocated which involve additional variables. 29
Supplemental Material
sj-docx-1-msc-10.1177_09691413211056970 - Supplemental material for Faecal haemoglobin concentrations in women and men diagnosed with colorectal cancer in a national screening programme
Supplemental material, sj-docx-1-msc-10.1177_09691413211056970 for Faecal haemoglobin concentrations in women and men diagnosed with colorectal cancer in a national screening programme by Gavin RC Clark, Jayne Digby, Callum G Fraser, Judith A Strachan and Robert JC Steele in Journal of Medical Screening
Footnotes
Authors’ Contribution
GRCC collected and analysed the data, created the table and the figures, and contributed to writing the paper. JD contributed to the analysis of the data and to the writing of the paper. CGF contributed significantly to the analysis and interpretation of the data and to the writing of the paper. JAS supervised the laboratories that analysed the FIT in the SBoSP and contributed to writing the paper. RJCS is Clinical Director of the SBoSP, initiated and coordinated the project, and created the first and final drafts of the paper. All authors approved of the final draft submitted.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The FIT roll-out of FIT in the SBoSP was funded by Scottish Government.
Data Availability Statement
Data are available upon reasonable request Data may be available following consultation with Professor RJC Steele: r.j.c.steele@dundee.ac.uk
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.