
Abstract
Objectives
Despite several interventions, colorectal cancer (CRC) screening uptake remains below acceptable levels in Italy. Among the potential determinants of screening uptake, only a few studies analysed the role of general practitioners (GPs). The aim was to evaluate the variation in screening uptake of the clusters of subjects assisted by single GPs.
Setting
Ancona province, Central Italy.
Methods
Cross-sectional study, including all residents aged 50–69 years, who were offered the public screening programme with biannual faecal immunochemical tests. Demographic (of all GPs) and screening data (of all eligible residents) for years 2018–2019 were collected from the official electronic datasets of the Ancona Local Health Unit. The potential predictors of acceptable screening uptake, including GP's gender, age, and number of registered subjects, were evaluated using random-effect logistic regression, with geographical area as the cluster unit.
Results
The final sample consisted of 332 GP clusters, including 120,178 eligible subjects. The overall province uptake was 38.0% ± 10.7%. The uptake was lower than 30% in one-fifth of the GP clusters, and higher than 45% in another fifth. At multivariable analysis, the significant predictors of uptake were younger GP age (p = 0.010) and lower number of registered subjects (p < 0.001). None of the GP clusters with 500 subjects or more showed an uptake ≥45%.
Conclusions
The wide variation across GPs suggests they might substantially influence screening uptake, highlighting a potential need to increase their commitment to CRC screening. Further research is needed to confirm the role of the number of registered subjects.
Introduction
In Italy, almost 50,000 new cases of colorectal cancer (CRC) are diagnosed yearly. 1 Screening programmes are effective in reducing CRC burden, 2 and they have thus been recommended in all Italian provinces since 2001, with most programmes using the faecal immunochemical test (FIT). 3 The screening uptake of many programmes, however, is still below the 45% acceptability threshold set by the Italian Group for Colorectal Cancer Screening (GISCoR).4,5
Several interventions have been attempted to increase the uptake, such as mass educational campaigns, mailing FIT kits, providing reminders, and promotion through general practitioners (GPs).6,7 Although GPs' advice has been associated with higher CRC screening uptake,8,9 and all Italian GPs are trained to promote cancer screening, GPs' potential impact on CRC screening uptake remains largely undetermined.7,10 Indeed, only one similar study was performed in Italy on data from 2006 to 2012, and more recently one in Switzerland, both of which showed large differences in uptake of CRC screening according to the GP.11,12
In order to provide an updated assessment of the potential impact of GPs on CRC screening uptake, we performed a cross-sectional study to assess the extent of variation in uptake among the clusters of subjects registered with different GPs.
Methods
In the province of Ancona, Central Italy, the CRC screening programme uses FIT and is recommended free of charge for all citizens aged 50–69 years, every two years. The programme is managed by the Local Health Unit, which regularly sends letter invitations to all eligible subjects. The letter contains the signature of the Director of the Screening Programme, and also that of each person's GP, as suggested by national guidelines in order to improve the programme's reliability. In the province, all pharmacies distribute FIT vials, 34 collection points are available for vial collection, and one laboratory analyses the specimens (Figure 1).
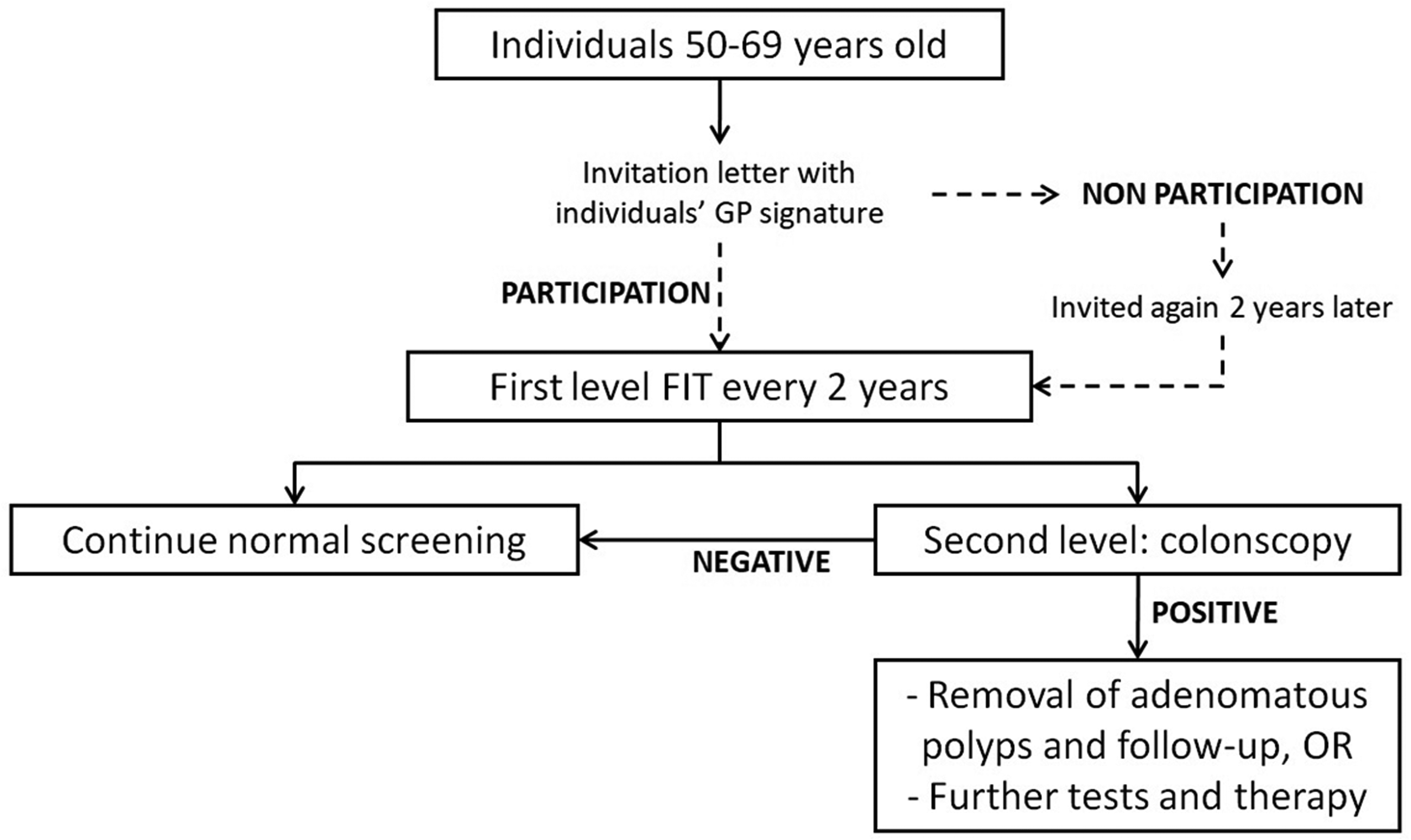
Colorectal cancer screening organization in the Ancona province. GP: general practitioner; FIT: faecal immunochemical tests. The dashed arrows represent the phases of the screening programme in which GP advice could improve uptake.
All data refer to the years 2018–2019 and have been obtained from the cancer screening software of the Local Health Unit of Ancona. For all GPs of the province, we retrieved individual data on age, gender, geographic location of the office, number of registered subjects who participated in CRC screening, and total number of registered subjects who were eligible for screening participation. Data for individual eligible subjects were not available; only the proportion participating for each practice was obtained. GPs with less than 20 eligible registered subjects, or retired during the study period, were excluded from the analyses. Registered subjects are those individuals that are followed and assisted by a single GP, who, in turn, is in charge of the primary healthcare of all the patients registered into his/her list. Assuming a two-tailed p-value of 0.05, the main analysis, based upon a total of 199 GPs aged 61 years or more, and 133 GPs aged up to 60 years, with average screening uptakes of 36.5% (SD 8.3%) and 40.1% (13.2%), respectively, had a statistical power of 79% to detect significant differences in registered patients screening uptake between GPs aged 61 years or more, versus GPs aged up to 60 years.
We computed the CRC screening uptake separately for each cluster of subjects registered with single GPs. 13 First, Student's t tests were used to evaluate uptake according to GPs' characteristics. In order to explore the possible determinants of uptake variability across GP clusters, we evaluated the potential independent association between uptake and GPs' gender, age (continuous), and number of registered subjects (continuous), using random-effects linear regression. Additionally, we evaluated the potential independent association between reaching the 45% uptake acceptability threshold and GPs' gender, age (60 years or younger, over 60), and number of registered subjects (<250, 250–349, 350–449, ≥450), using random-effects logistic regression. For both models, geographical area was used as the cluster unit, and all the other recorded variables were included a priori. 14 Statistical significance was defined as a two-sided p-value < 0.05 for all analyses, which were performed using Stata 15.1 (Stata Corp., College Station, TX, USA, 2017).
Results
The final sample consisted of 332 GPs' clusters, including a total of 120,178 subjects eligible for CRC screening in the years 2018–2019 (mean cluster size: 362). The mean uptake of these clusters was 38.0% (standard deviation: 10.7%; Table 1). The uptake largely varied across clusters, ranging from a minimum of 6.9%, up to a maximum of 76.5%. Out of all the GP clusters, 12 (3.6%) showed an uptake below 20%, and 68 (20.5%) showed an uptake below 30%. Only 67 clusters (20.2%) achieved an uptake of 45% or more (Figure 2).
CRC screening uptake across GP clusters, overall and by selected GP's characteristics. Years 2018–2019.
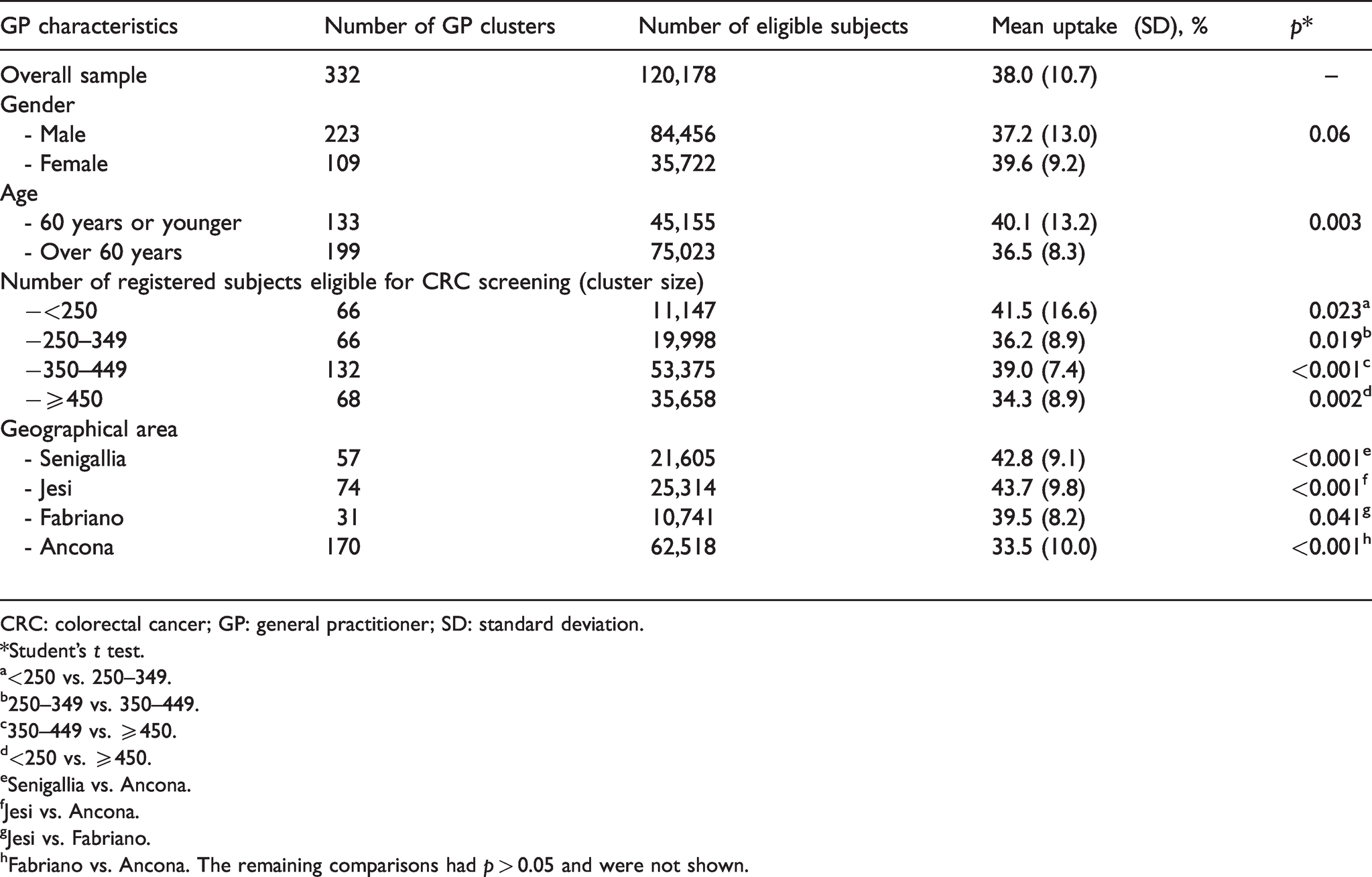
CRC: colorectal cancer; GP: general practitioner; SD: standard deviation.
*Student’s t test.
a<250 vs. 250–349.
b250–349 vs. 350–449.
c350–449 vs. ≥450.
d<250 vs. ≥450.
eSenigallia vs. Ancona.
fJesi vs. Ancona.
gJesi vs. Fabriano.
hFabriano vs. Ancona. The remaining comparisons had p > 0.05 and were not shown.
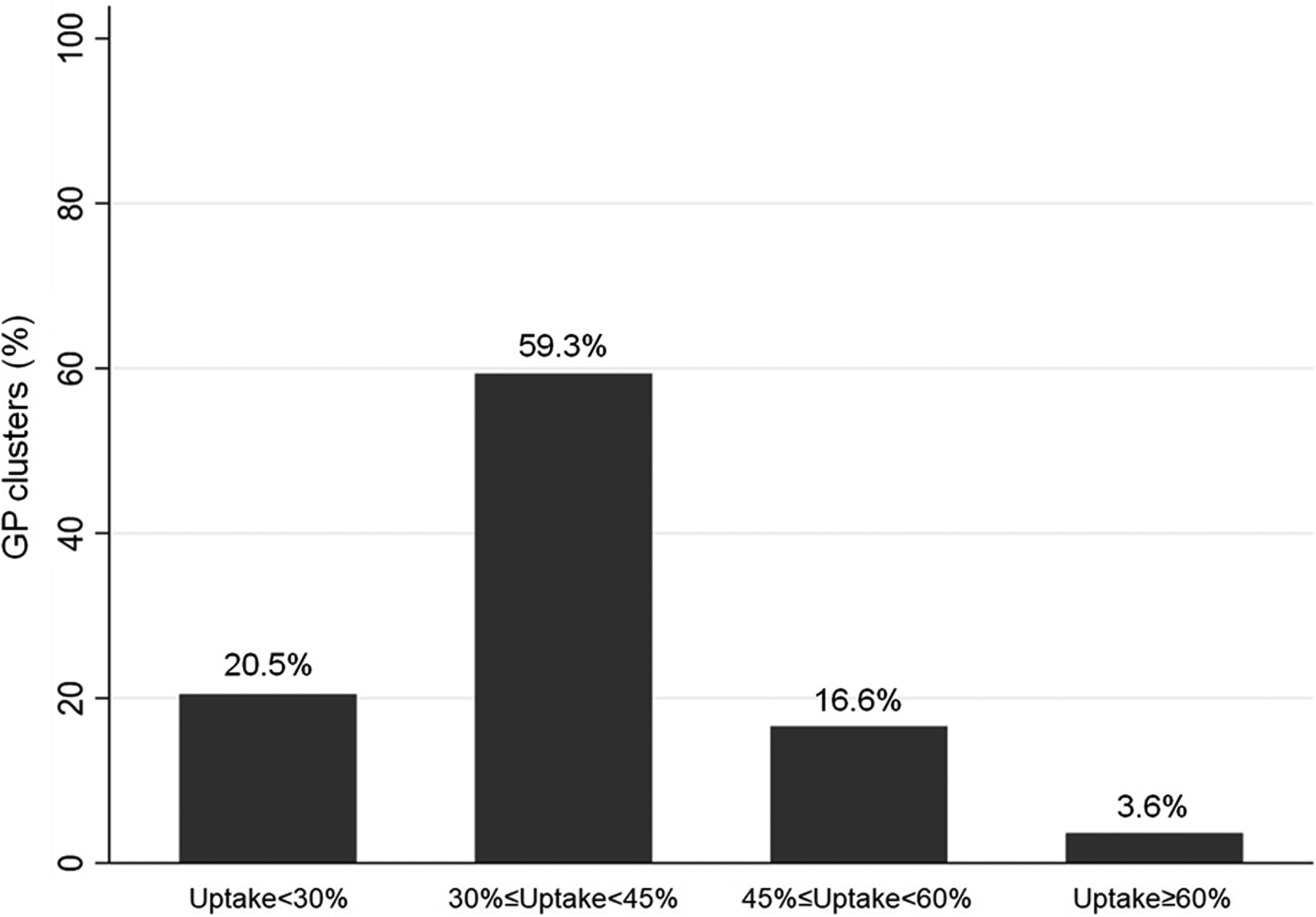
Bar graph showing GP cluster distribution by categories of 2018–2019. CRC screening uptake. GP: general practitioner; CRC: colorectal cancer.
The mean uptake varied significantly by GPs' age (36.5% and 40.1%, respectively, in the clusters registered with GPs aged >60 and ≤60 years; p = 0.003), geographical area (33.5% and 43.7%, respectively, in the clusters from Ancona and Jesi; p < 0.001), and number of registered subjects (34.3% and 41.5%, respectively, in the clusters with ≥450 and <250 eligible subjects; p = 0.002) (Table 1), with an uptake lower than 45% in all of the clusters including 500 subjects or more (Supplementary Figure 1).
Multivariable analysis substantially confirmed univariate results (Table 2): uptake was significantly and independently associated with younger GP's age (+4.8% for a 10-year decrease; 95% confidence interval – CI: 3.7%–5.9%), and smaller cluster size (+1.5% for a 100-subject decrease; 95% CI: 0.4%–2.6%). Finally, concerning the uptake acceptability threshold, GPs aged over 60 years had odds ratio – OR 0.47 (CI 0.27–0.84) of reaching this threshold, compared to the younger ones. Also, those with 450 or more registered eligible subjects had OR 0.16 (CI 0.07–0.37) of reaching the same acceptability threshold, compared to the GPs with less than 250 subjects, (Table 3). No significant differences in screening uptake were observed by GP's gender.
Results of the random-effects linear regression predicting CRC screening uptake, with geographical area as the cluster variable.
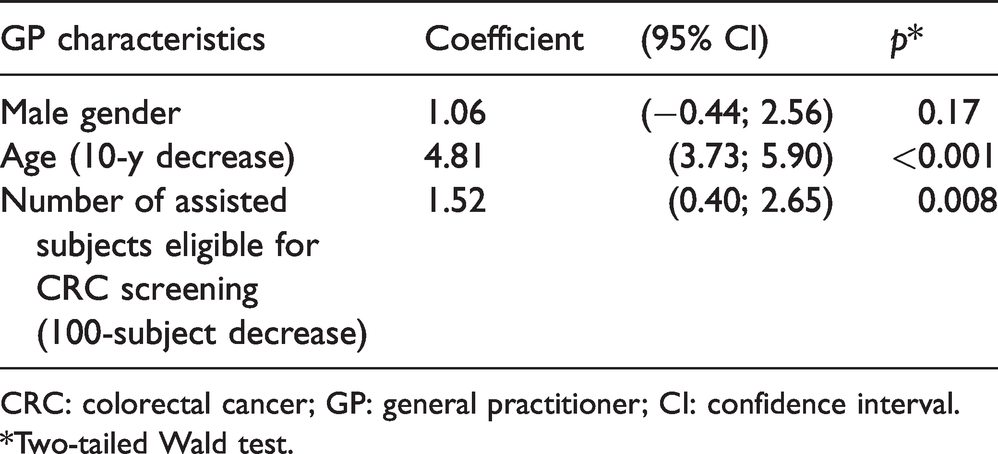
CRC: colorectal cancer; GP: general practitioner; CI: confidence interval.
*Two-tailed Wald test.
Results of the random-effects logistic regression predicting CRC screening uptake at or above the 45% acceptability threshold, with geographical area as the cluster variable.
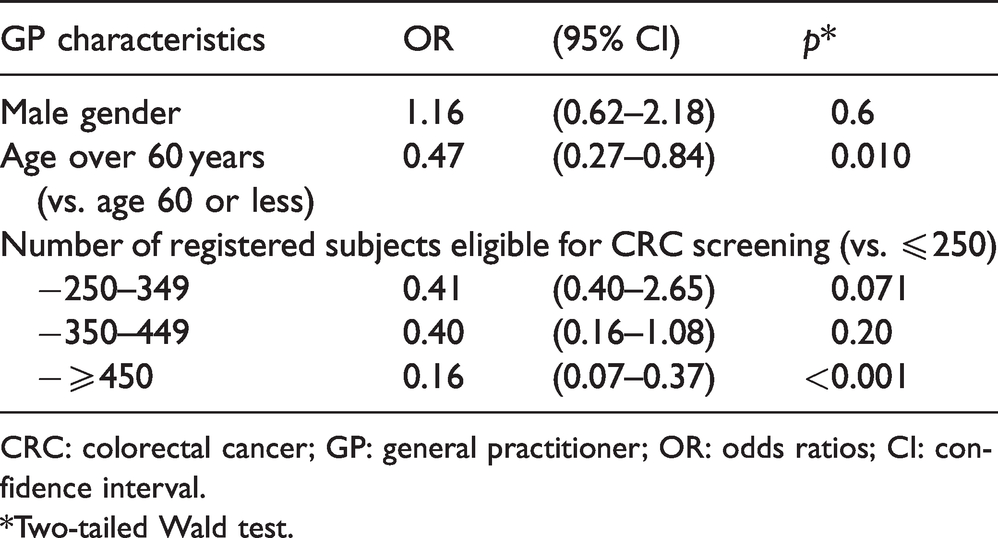
CRC: colorectal cancer; GP: general practitioner; OR: odds ratios; CI: confidence interval.
*Two-tailed Wald test.
Discussion
Overall, during the 2018–2019 biennium, in a province of Central Italy, we observed wide variations in CRC screening uptake between clusters of citizens registered with different GPs: about one-fifth of the clusters showed an uptake lower than 30%, while only another fifth showed the acceptable uptake of 45%. After adjusting for GP's gender and geographical area, the clusters of younger GPs, with less registered subjects, showed a significantly higher screening uptake.
This study offers evidence on a scarcely explored subject, namely the impact of GPs on uptake of CRC screening, and it is the first, in Italy, to assess the possible role of a GP’s target population size. 15 The screening database provided official certified data on the entire resident population, with a very low (<5%) proportion of privately performed FIT which was missed. Also, although monocentric, this study included a large sample of over 120,000 subjects registered with GPs.
The study has also some limitations that must be considered. First, no individual-level determinants of screening, such as socio-economic status, were available for the subjects registered with the GPs. However, within the province of Ancona, it is unlikely that the differences across GP clusters were large enough to explain the observed wide variation in screening uptake.16,17 Moreover, the large number of clusters minimizes the chances of potential differences being unbalanced in the overall sample. Another limitation is the small number of GP-level variables, preventing the assessment of potential determinants of screening uptake beyond gender, age, and cluster size. Finally, the cross-sectional design did not allow inferring causal relationships.
With regard to the observed wide variations in CRC screening uptake across GP clusters, only one Italian study analysed the uptake in 320,534 subjects registered with GPs in Perugia in 2006–2008 and 2011–2012, with both GPs and geographical areas as cluster units, and found similarly broad differences among GP clusters (range 21%–57%). 11 Even larger variations across GPs (range 0%–91%) were found in a 2017 Swiss study including 3451 subjects. 12
The finding of an inverse association between uptake and the number of patients registered with GPs is in line with the only Italian study available to date: in the Lazio Region, the GPs visiting more than 25 patients per day showed a 26% lower screening uptake compared to those visiting less patients. 13 In contrast, a study from Wisconsin, USA, reported a positive association between a larger number of eligible registered individuals and screening uptake. 18 However, this study was performed within a collaborative of healthcare providers and purchasers committed to improving healthcare quality, where specific enabling factors, incentives, or controls might have increased CRC screening uptake. 18 In fact, in the province of Ancona there was no system motivating GPs to promote CRC screening.
Also, the observation of a lower mean uptake in the metropolitan area (Ancona) is in agreement with one Italian National study, 19 and a study from England, where London was the area with the lowest uptake. 20 However, one study from USA and one from Australia found the lowest uptake in rural communities.21,22 Indeed, it is plausible that the provision of cancer screening could differ substantially in rural areas of European countries, as opposed to rural areas of countries with lower population density, where remoteness may represent a very large barrier to healthcare. 23
Finally, our observation of a higher uptake in clusters of younger GPs contrasts with the articles cited above from Italy, Switzerland, and Wisconsin, which found no association between GPs' age and uptake.12,15,18 While these three studies included less than 100 GPs, and therefore could have been underpowered to assess this association, it cannot be excluded that the determinants associated with CRC screening uptake, such as cluster size and GPs' age, might be context-specific.12,15,18
A variety of interventions involving GPs, or ‘regular doctors’, have been designed to improve CRC screening uptake: the most common are GP endorsement of screening invitations, sending reminders to both patients and GPs (lists of registered persons not adhering to the screening), providing FIT kits at physicians' offices, or distributing printed screening advice.24–28 Of these, GP endorsement of the invitation to CRC screening, as well as point-of care FIT kits provision, were shown to produce substantial improvements in uptake, while scarce evidence is available in support of reminders to GPs and distribution of printed material.24–29
In the province of Ancona, the GP's signature is already present on invitation letters, and therefore the detected variations in uptake may be concerning, suggesting the need to increase the commitment of the GPs to CRC screening. In the area under investigation, the policies may prioritize older GPs and those with larger clusters. Further research is needed to determine whether the observed variations are common in other areas, as well as to confirm the influence of the age of GPs and of the number of citizens registered with each GP on CRC screening uptake. Also, future studies are required to interview older and younger GPs, as well as those with larger and smaller populations, to better understand why these populations have higher or lower screening participation, what the GPs are doing differently in relation to CRC screening promotion, and their perceived role.
Supplemental Material
sj-pdf-1-msc-10.1177_09691413211035795 - Supplemental material for Wide variability in colorectal cancer screening uptake by general practitioner: Cross-sectional study
Supplemental material, sj-pdf-1-msc-10.1177_09691413211035795 for Wide variability in colorectal cancer screening uptake by general practitioner: Cross-sectional study by Cecilia Acuti Martellucci, Maria E Flacco, Margherita Morettini, Giusi Giacomini, Matthew Palmer, Stefania Fraboni and Francesca Pasqualini in Journal of Medical Screening
Footnotes
Data availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethics Committee of the Marche Region on April 1st 2020, with number 20202084.
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.