
Abstract
Objectives
Colorectal, breast, and cervical cancers are leading causes of morbidity and mortality among Canadian women. While organized screening programs aim to reduce this burden, participation rates remain suboptimal, particularly for colorectal cancer screening. This study examined factors associated with colorectal cancer screening uptake among women participating in breast and cervical cancer screening ('screen-aware” women), investigated patterns of concurrent participation across all three programs, and identified associated factors.
Methods
Cross-sectional data from the 2017 Canadian Community Health Survey were analyzed for women aged 50–69 eligible for breast cancer (mammography), cervical cancer (Pap smear), and colorectal cancer (fecal and/or endoscopy tests) screening (n = 10,426). Multivariable logistic regression evaluated factors associated with colorectal cancer screening among “screen-aware” women. Multinomial logistic regression assessed factors related to full (all three), partial (any two), single, or non-participation across screening programs, using “no screening” as the reference.
Results
Although the majority of women (87%) participated in at least one screening program, only 27% reported full participation. Colorectal cancer screening (53.7%) lagged behind breast and cervical cancer screening (∼64%). Among “screen-aware” women, older age (adjusted odds ratio 1.50, 95% confidence interval 1.31–1.71), higher income, self-rated health as “great” (adjusted odds ratio 1.31, 95% confidence interval 1.05–1.63), and having a regular healthcare provider (adjusted odds ratio 3.29, 95% confidence interval 2.45–4.40) were associated with higher colorectal cancer screening participation. Having multiple chronic conditions reduced colorectal cancer screening likelihood (adjusted odds ratio 0.72, 95% confidence interval 0.55–0.94). Higher income, self-rated health, having a regular healthcare provider, and physical activity increased the odds of full screening participation, while smoking and Asian identity reduced the odds.
Conclusions
Colorectal cancer screening uptake remains low among Canadian women, even those participating in other cancer screenings. Socioeconomic, health-related, and systemic factors influence concurrent screening participation. Tailored interventions addressing identified barriers and promoting equitable access to screening are crucial for improving cancer prevention efforts.
Keywords
Introduction
Colorectal (CRC), breast (BC), and cervical (CC) cancers are a major cause of morbidity and mortality in Canada, accounting for 36% of new cancer cases and 25% of cancer-related deaths among women in 2023.1,2 To address this burden, organized screening programs have been established nationwide, guided by recommendations from the Canadian Task Force on Preventive Health Care.
3
The CTFPHC recommends:
BC screening with mammography every 2–3 years for women aged 50–74. CC screening with a Pap test every 3 years for asymptomatic women aged 25–69. CRC screening with fecal tests every 2 years or either flexible sigmoidoscopy or colonoscopy (endoscopy tests) every 10 years for people aged 50–74 at average risk of CRC.
4
While screening has been recognized as an essential public health measure to reduce cancer incidence and mortality,4,5 participation rates remain well below national targets in many population groups.6–9 The suboptimal uptake leads to a higher proportion of late-stage cancer diagnoses, associated with poorer treatment outcomes and survival. 2 This disparity is particularly striking for CRC, where 49% of new cases are diagnosed at stages III or IV, compared to 17.3% of breast cancers and 28.3% of cervical cancers. 10
The lower uptake of CRC screening compared to BC and CC screening is a persistent issue, even after accounting for sociodemographic and healthcare access disparities shown to be associated with non-participation across all screening programs.8,11,12 The relative recency of organized CRC screening programs and the diverse range of recommended testing modalities may contribute to this disparity. Additionally, individual health beliefs and risk perceptions may play a role in influencing screening uptake.11,13
Furthermore, there is growing interest in understanding patterns of concurrent participation in multiple cancer screening programs. International studies have shown that a surprisingly low proportion of women eligible for all three programs participate in all or any combination of them, with CRC screening consistently lagging behind BC and CC screening.14–16 These findings underscore the need to investigate similar patterns within the Canadian context and identify the factors associated with full, partial, single, or non-participation in screening programs. 17 Understanding the factors associated with lower CRC participation is similarly crucial for designing strategies to promote greater screening uptake.
To guide our analysis, we utilize Andersen's Behavioral Model of Health Services Use, 18 which proposes that healthcare utilization, including preventive screenings, is influenced by an interplay of predisposing, enabling, and need factors. 18 Predisposing factors, such as age, education, and cultural beliefs, can shape an individual's attitudes and beliefs about screening. Enabling factors, including income, access to healthcare services, and having a regular healthcare provider, can facilitate or hinder an individual's ability to participate in screening. Finally, need factors, such as perceived health status, family history of cancer, and presence of chronic conditions, can influence an individual's perceived susceptibility to cancer and their motivation to seek screening.19–21 By examining screening participation through the lens of this framework, we can better understand the interplay of individual, social, and systemic factors that influence cancer screening behaviors.
This study makes a unique contribution as the first in Canada to examine factors associated with participation in one, two, or all three cancer screening programs among women, using nationally representative data from the 2017 Canadian Community Health Survey. Specifically, we aim to:
Examine factors associated with CRC screening uptake among women who participate in BC and/or CC screening ('screen-aware” women). Investigate patterns of concurrent participation in one, two, or all three cancer screening programs. Identify the factors associated with these distinct patterns of screening participation.
By exploring these objectives through the lens of Andersen's Behavioral Model, this study provides valuable insights to inform the development of tailored interventions aimed at improving screening participation and reducing cancer-related morbidity and mortality among Canadian women. Ultimately, a better understanding of the factors influencing screening behavior can support the design of more effective screening programs and contribute to reducing the burden of these cancers in Canada.
Methods
Study design and data source
This was a cross-sectional study using data from the 2017 Canadian Community Health Survey (CCHS). 22 The CCHS is a nationally representative survey conducted by Statistics Canada that collects information on health status, health care utilization, and determinants of health from Canadians aged 12 and older. The survey employs a complex, multi-stage sampling design to ensure representation across diverse geographic and demographic groups. Full-time members of the Canadian Armed Forces and residents of certain remote areas and First Nations reserves are excluded from the sample, representing approximately 3% of the Canadian population. The 2017 CCHS achieved a response rate of 87% and included nearly 57,000 respondents. 22 The 2017 CCHS was selected because it is the most recent iteration that includes data on CRC screening participation for all Canadian provinces.
Participant selection
This study included women aged 50‒69 residing in the 10 Canadian provinces who participated in the 2017 CCHS. Canada has ten provinces and three territories. While the ten provinces are sampled annually for the CCHS, the three territories are included every two years to ensure sufficient sample size for representativeness. Therefore, this analysis focused on the ten provinces to ensure that the findings are representative of this population. Additionally, the age range was selected to ensure that all participants were eligible for BC, CC, and CRC screening according to current Canadian guidelines. Women were excluded if they reported a history of mastectomy or hysterectomy, or if they underwent mammography as follow-up to breast cancer treatment or due to breast problems. The final analytic sample consisted of 10,426 women.
Variables
The primary outcome variables were participation in BC and CC screening within the past 3 years and participation in either fecal occult blood testing within the past 2 years or endoscopy (flexible sigmoidoscopy or colonoscopy) within the past 10 years, as per Canadian guidelines.
3
Participants were asked about their screening history and the date of their last screening test. Additionally, eight concurrent screening patterns were created to capture participation in all three, any two, one, or none of the screening programs:
Breast + Cervical + Colorectal (full participation) Breast + Colorectal Cervical + Colorectal Breast + Cervical Colorectal only Breast only Cervical only No participation
In line with previous studies15–17,23,24 and data availability within the CCHS, the following independent variables were included in the analysis:
Statistical analysis
Data analysis was performed using SAS 9.4, employing survey procedures to account for the complex sampling design of the CCHS. Survey weights provided by Statistics Canada were applied to generate nationally representative estimates. Bootstrapped analyses with 500 replicate weights were conducted to obtain accurate variance estimates. Descriptive statistics were used to present the distribution of sociodemographic characteristics and screening patterns. Multivariable logistic regression was used to examine factors associated with CRC screening participation among “screen-aware” women (those who participated in BC and CC screening). Multivariable multinomial logistic regression was used to assess factors associated with full, partial, or no screening participation, using “no screening” as the reference category. Covariates included age, marital status, household income, self-rated health, physical activity level, smoking status, race, immigrant status, and number of chronic health conditions. Multicollinearity was assessed using a variance inflation factor of 5 as the cutoff. Educational attainment was not included in the regression models due to its high correlation with household income. Results are presented as weighted proportions and adjusted odds ratios (AOR) with 95% confidence intervals (CI). A p-value of less than 0.05 was considered statistically significant. All analyses adhered to Statistics Canada's confidentiality and data protection guidelines.
“Don't know,” “Refusal,” and “Not stated” responses in the CCHS were treated as missing data. The proportion of missing data was relatively small (less than 5% on average) for all variables. A complete case analysis was conducted, excluding cases with missing data on any of the variables included in the analysis. While complete case analysis can introduce bias if the missing data are not missing completely at random, the low proportion of missing data minimizes this potential bias.
Results
The final analytic sample consisted of 10,426 women aged 50–69 from the ten Canadian provinces who met the inclusion criteria. The majority of respondents were aged 50–59 (52%), married or in a common-law relationship (70%), and identified as White (82.5%). About half of the respondents (50%) had a total annual household income of over $80,000, and 60% reported having post-secondary education. Most respondents reported being physically active (73%) and having a regular healthcare provider (91%). However, a substantial proportion reported having one or more chronic health conditions (76%), with 19% having four or more, and 60% were overweight or obese (Table 1).
Demographic distribution of women aged 50–69, Canada.
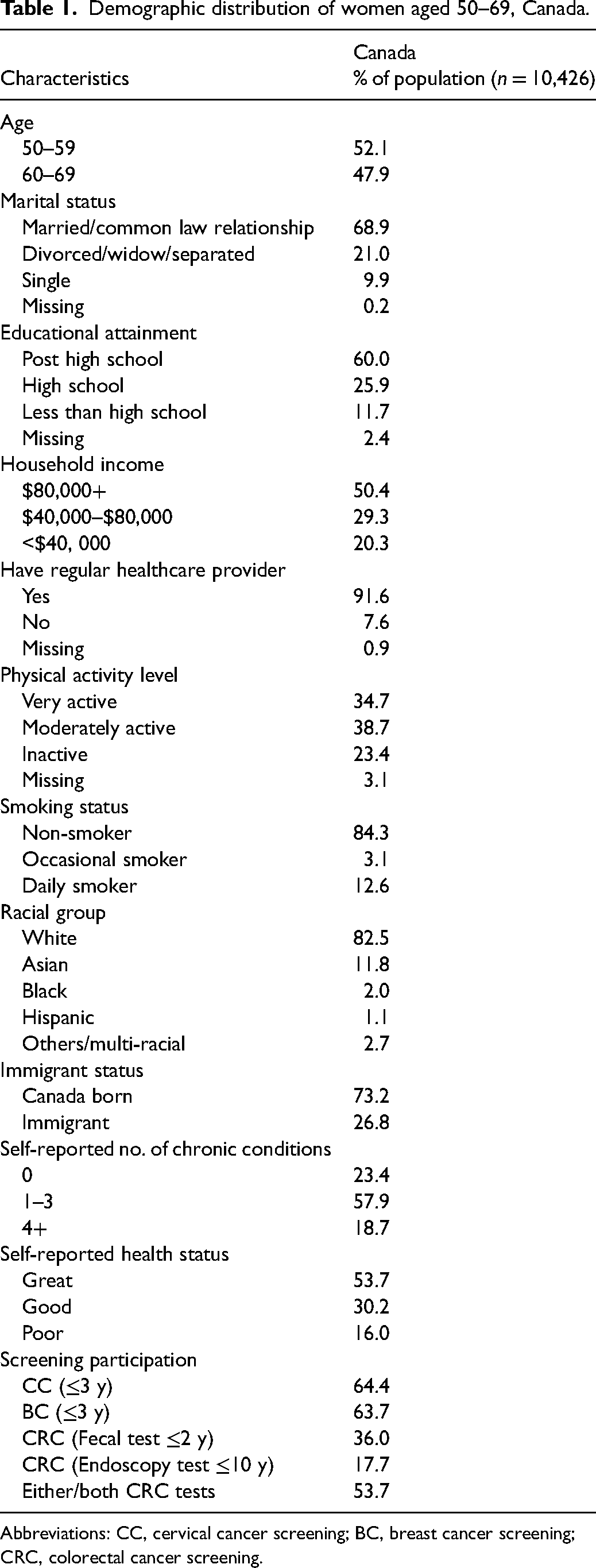
Abbreviations: CC, cervical cancer screening; BC, breast cancer screening; CRC, colorectal cancer screening.
Screening participation
Overall, 53.7% of respondents reported participating in CRC screening, with fecal tests being the most common method (36%). Participation in BC and CC screening was higher, with approximately 64% of respondents reporting participation in each (Table 1).
Concurrent screening patterns
Table 2 presents the patterns of concurrent participation in cancer screening. Full participation (participation in all three screening programs) was reported by 26.7% of respondents. Partial participation (participation in any two programs) was the most common pattern (35.5%), with the BC + CC combination being the most frequent (19.7%). Single program participation was reported by 24.4% of women, with CC only being the most common (10.5%), followed by BC only (9.0%) and CRC only (4.9%). Notably, 13.4% of respondents reported not participating in any of the three screening programs.
Patterns of concurrent cancer screening participation among women aged 50–69, Canada.
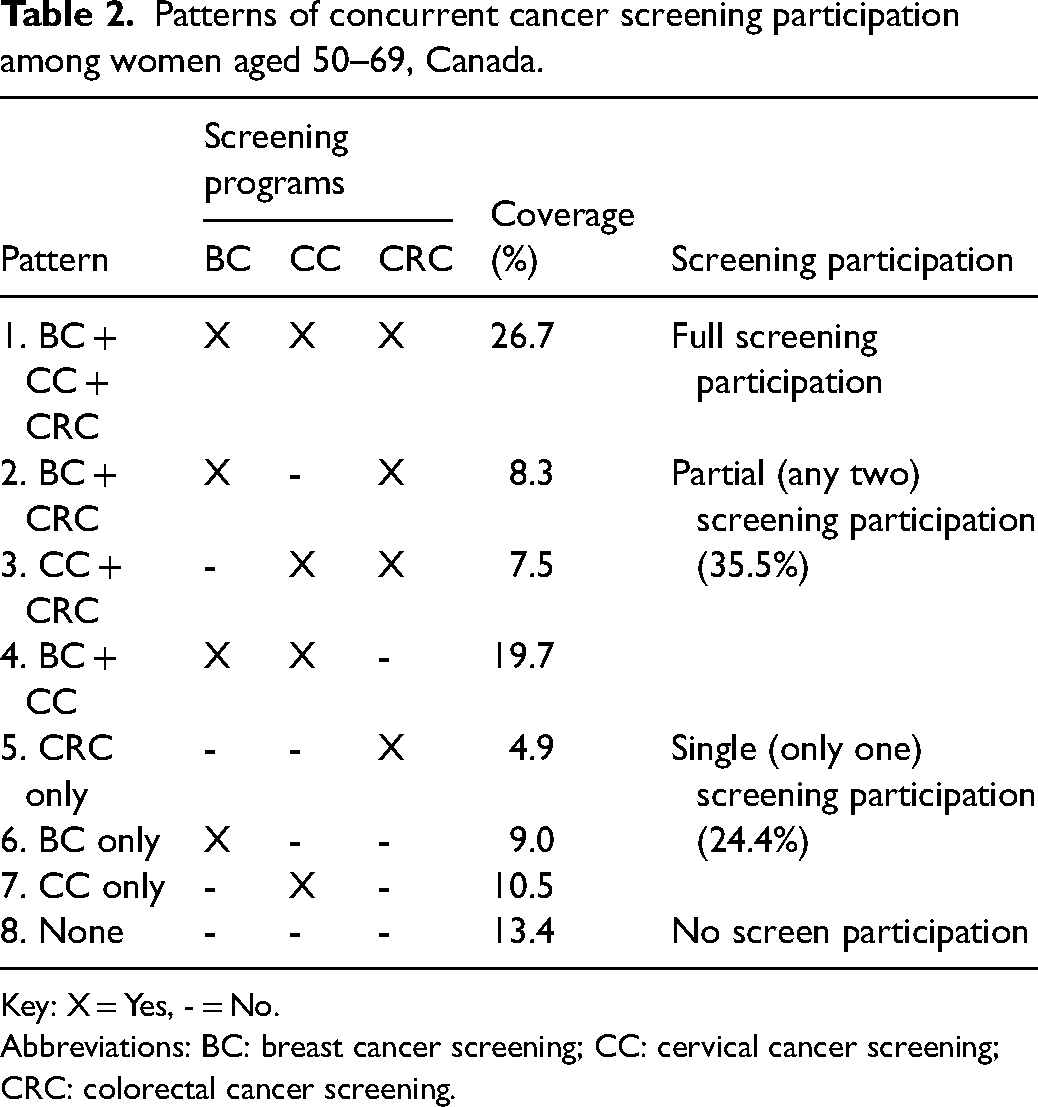
Key: X = Yes, - = No.
Abbreviations: BC: breast cancer screening; CC: cervical cancer screening; CRC: colorectal cancer screening.
Sociodemographic variation in screening patterns
Screening participation patterns varied significantly across sociodemographic groups (Table 3). Partial participation, particularly the BC + CC combination, was the most common pattern across most sociodemographic categories. However, “no screening” was prevalent among women with lowest education level (21.2%), those in the lowest income bracket (24.3%), and daily smokers (25.8%). Full participation was highest among women with post-high school education (29.5%), those in the highest income bracket (31.6%), those with a regular healthcare provider (28.1%), those reporting “great” health (31.3%), those who were very physically active (31.0%), and non-smokers (28.4%).
Distribution of screening participation pattern by sociodemographic characteristics among women aged 50–69, Canada.
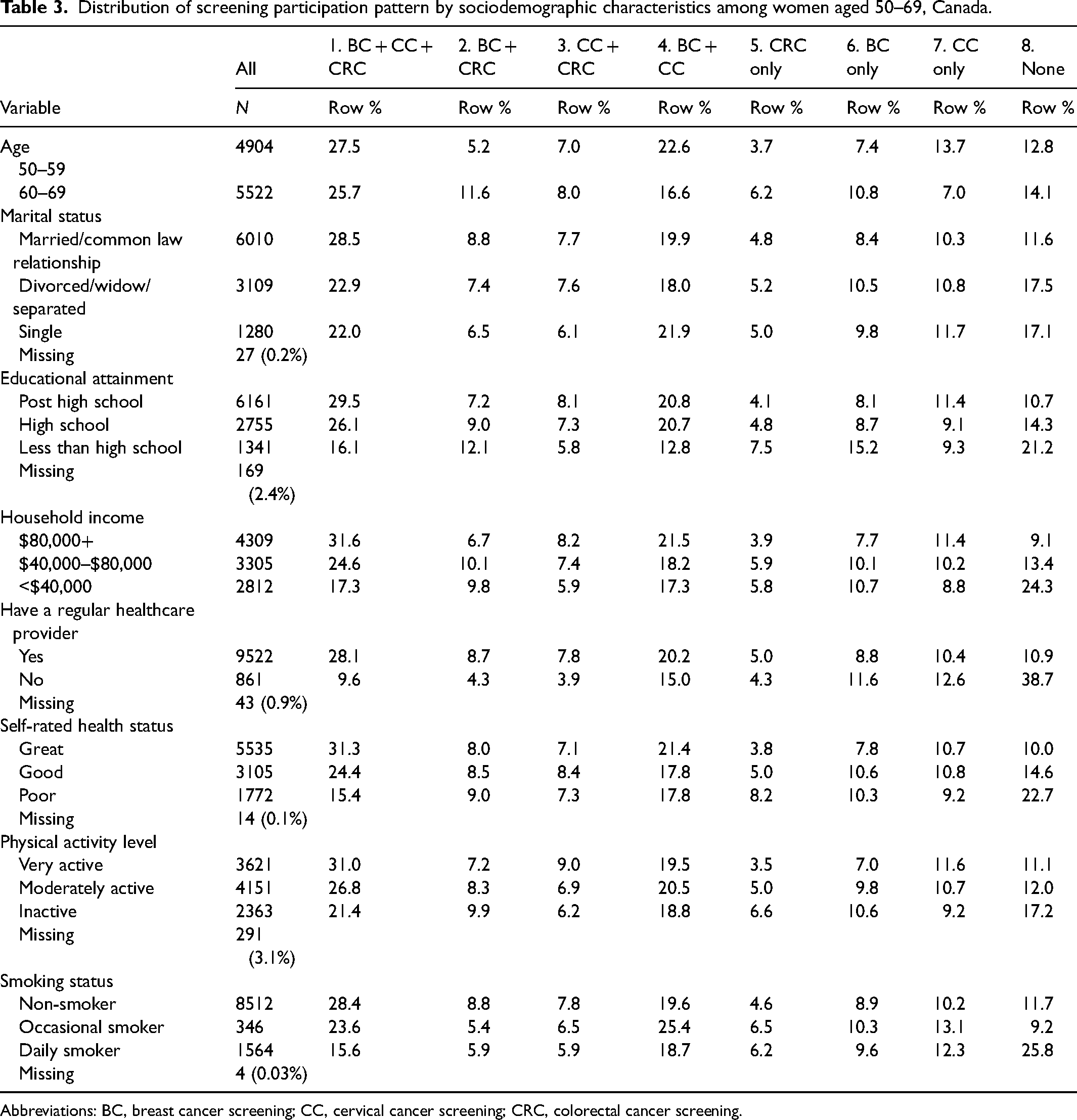
Abbreviations: BC, breast cancer screening; CC, cervical cancer screening; CRC, colorectal cancer screening.
Barriers to screening participation
Among women who did not participate in at least one screening program, the most common barrier reported was the belief that the test was unnecessary (ranging from 23.4% to 34.2% across screening programs). This was particularly true for colonoscopy/sigmoidoscopy (34.2%). For both CRC screening options, the most frequent barrier was healthcare provider deeming the test unnecessary (40.1% for fecal tests and 52.7% for endoscopy). Other barriers, such as lack of time, fear or discomfort, lack of knowledge, and lack of a regular healthcare provider, were reported less frequently (Table 4).
Self-reported barriers to cancer screening among women aged 50–69 with no screening history, Canada.
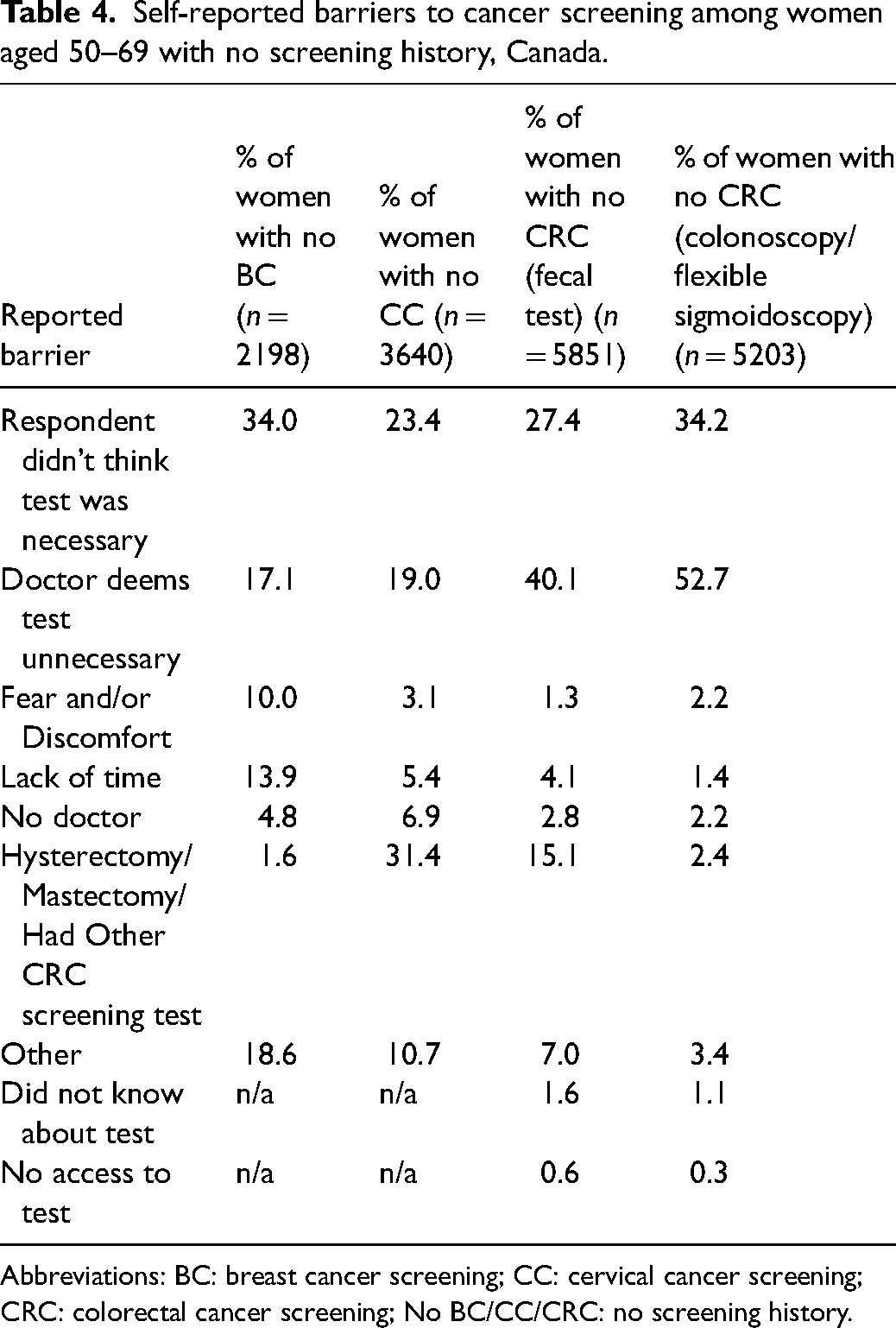
Abbreviations: BC: breast cancer screening; CC: cervical cancer screening; CRC: colorectal cancer screening; No BC/CC/CRC: no screening history.
Factors associated with screening participation
CRC screening among screen-aware women
Among all respondents, older age (60–69 years: AOR 1.50; 95% CI 1.31–1.71), higher income (AOR 1.37; 95% CI 1.13–1.67), “great” self-rated health (AOR 1.31; 95% CI 1.05–1.63), and having a regular healthcare provider (AOR 3.29; 95% CI 2.45–4.40) were associated with higher odds of CRC screening participation, while being a daily smoker and being an immigrant (AOR 0.73; 95% CI 0.56–0.94) were associated with lower odds (Table 5). In stratified analyses among women who participated in BC only or BC + CC, these associations remained significant, with the exception of household income and smoking status, which were no longer significant predictors. Additionally, having multiple chronic health conditions was associated with lower odds of CRC screening in these subgroups (AOR 0.72; 95% CI 0.55–0.94).
Factors associated with CRC screening among women with BC and BC + CC screening participation among women aged 50–69, Canada.
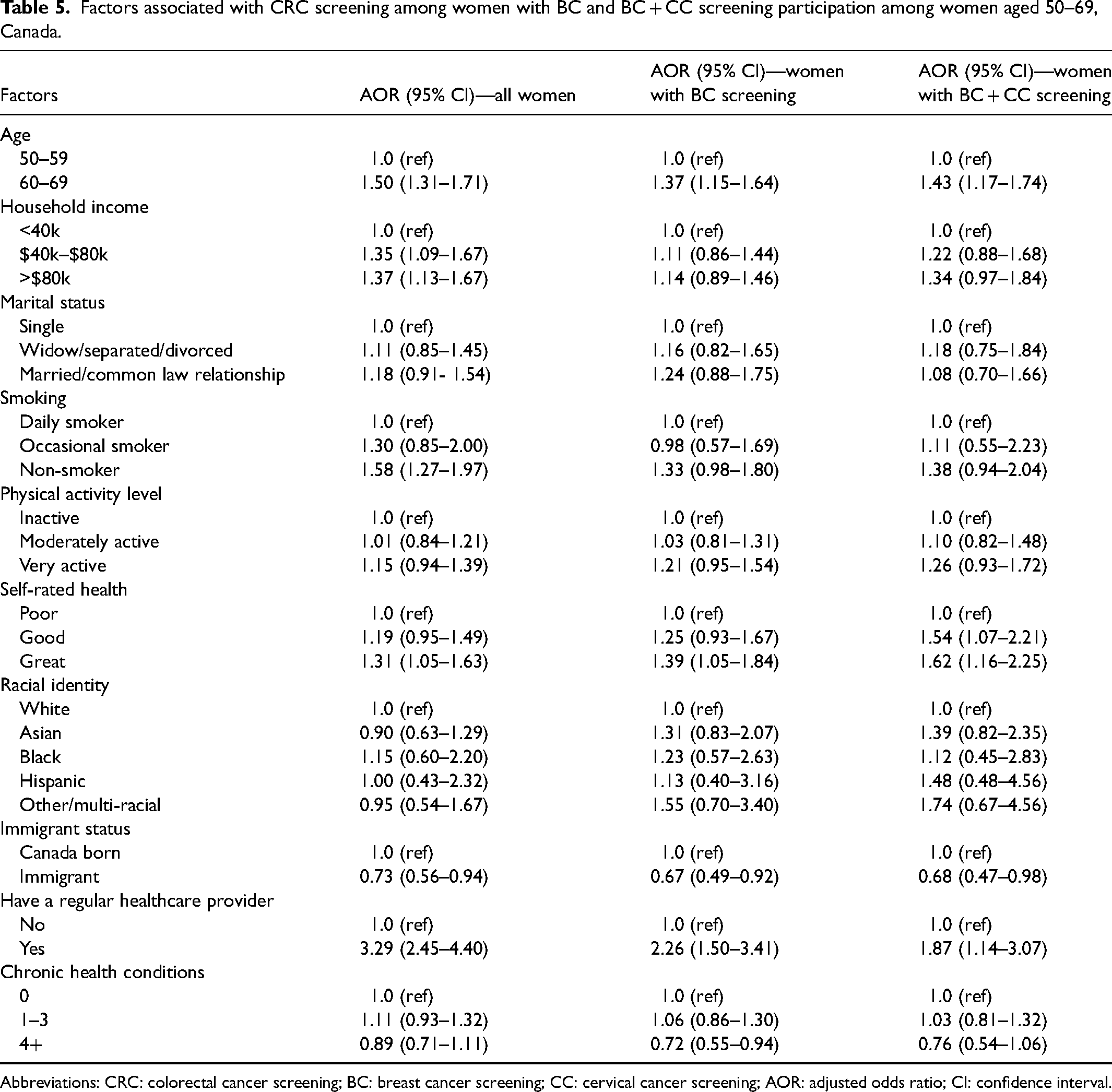
Abbreviations: CRC: colorectal cancer screening; BC: breast cancer screening; CC: cervical cancer screening; AOR: adjusted odds ratio; CI: confidence interval.
Concurrent screening patterns
Household income was significantly associated with all screening patterns (Table 6). Women in the middle-income bracket had higher odds of full participation (AOR 2.30; 95% CI 1.70–3.10), compared to those in the lowest income bracket. Similarly, women in the highest income bracket had significantly higher odds of full (AOR 3.15; 95% CI 2.27–4.37), partial (AOR 2.01; 95% CI 1.47–2.75) and single (AOR 2.04; 95% CI 1.50–2.77) screening participation. Self-rated health and physical activity were positively associated with full participation. Having a regular healthcare provider was strongly associated with all screening patterns, with particularly high odds for full participation. Smoking status was also a significant predictor, with occasional and non-smokers having higher odds of participation compared to daily smokers. The presence of multiple chronic health conditions was associated with increased odds of partial and single participation. Racial disparities were also observed, with Asian women having lower odds of full participation (AOR 0.68; 95% CI 0.43–0.98) and Black women having higher odds of full participation compared to White women (Table 6).
Multivariable multinomial regression of factors associated with full, partial (any two), single or no cancer screening participation, using “no screening” as the reference category, among women aged 50–69, Canada.
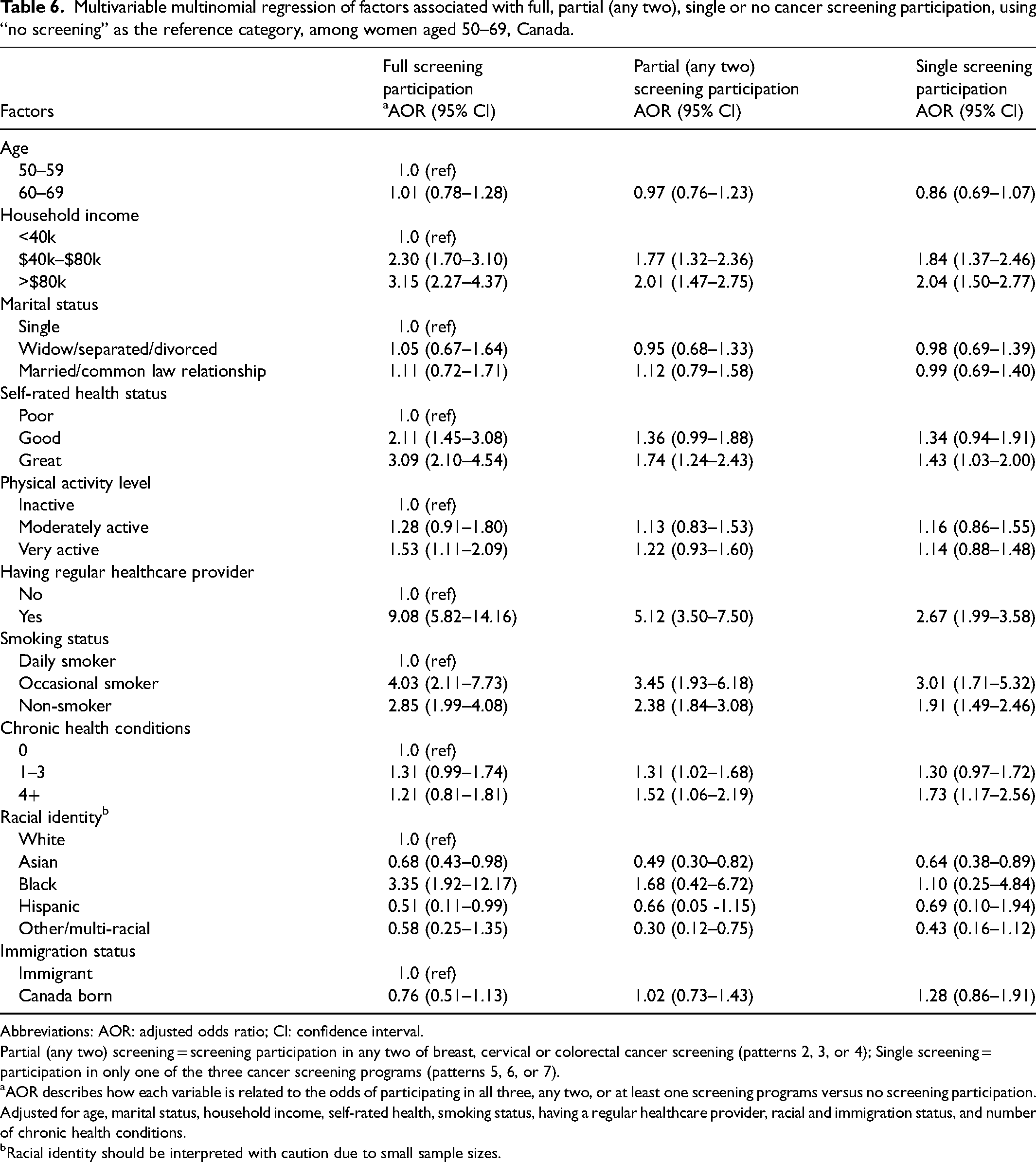
Abbreviations: AOR: adjusted odds ratio; CI: confidence interval.
Partial (any two) screening = screening participation in any two of breast, cervical or colorectal cancer screening (patterns 2, 3, or 4); Single screening = participation in only one of the three cancer screening programs (patterns 5, 6, or 7).
AOR describes how each variable is related to the odds of participating in all three, any two, or at least one screening programs versus no screening participation. Adjusted for age, marital status, household income, self-rated health, smoking status, having a regular healthcare provider, racial and immigration status, and number of chronic health conditions.
Racial identity should be interpreted with caution due to small sample sizes.
Discussion
Drawing from nationally representative cross-sectional survey data, this study investigated two key aspects of cancer screening behavior among Canadian women: (1) participation in CRC screening compared to BC and CC screening, and (2) the factors associated with concurrent participation in multiple screening programs. Findings show that among women eligible for all three cancer screenings, participation in CRC screening was lower compared to BC and CC screening. While 87% of women participated in at least one screening program, only 27% were up-to-date with all three, and 13% did not participate in any screening. Age, perception of health status, access to a regular healthcare provider, and immigrant status were factors associated with CRC screening participation among women up-to-date with BC and CC screenings. Additionally, income and lifestyle factors such as smoking status and physical activity level were associated with concurrent participation in multiple cancer screening programs. These findings, interpreted through the lens of Andersen's Behavioral Model of Health Services Use, 18 shed light on the complex interplay of predisposing, enabling, and need factors that contribute to preventive health behaviors like cancer screening.
Lower CRC screening participation
Despite the years of organized screening programs, our study found that participation in CRC screening remains lower than that for breast and cervical cancer screening. This disparity is consistent with findings from other countries.11,13,15,17,25–27 These differing participation rates suggest that each screening program may be associated with unique barriers, perceptions, and access issues, highlighting the need for targeted interventions to improve CRC screening uptake. 28
Our findings suggest that several factors may contribute to this lower participation in the CRC screening program. Predisposing factors, such as lower perceived susceptibility to CRC or concerns about the screening process may play a role.11,12,29,30 Public health campaigns that increase awareness of CRC risk factors and address misconceptions about screening could help improve participation. Enabling factors, such as access to a regular healthcare provider, are also crucial. 31 Our study found that having a regular healthcare provider was strongly associated with CRC screening participation, emphasizing the importance of provider recommendations and support. 31
However, the finding that a significant proportion of women reported their healthcare provider deeming CRC screening unnecessary highlights the need for better engagement with healthcare providers by cancer screening program administrators, improved provider–patient communication, and more emphasis on shared decision-making. This could involve educating providers on current screening guidelines and encouraging them to engage in more proactive discussions about CRC screening with their eligible patients. 31 Similarly, empowering women with clear and accessible information about CRC screening, including the benefits and risks of different screening modalities, can enable them to actively participate in informed discussions with their healthcare providers and make choices that align with their individual needs and preferences.29–31
Concurrent screening participation
Beyond individual screening programs, our study examined concurrent participation in CRC, BC and CC screening programs. We found that only 27% of women participated in all three screening programs, while 13% did not participate in any. These findings underscore the need to promote a more holistic approach to cancer prevention that encourages participation in all recommended screenings.
Predisposing factors, such as race/ethnicity and cultural beliefs, may influence women's attitudes towards different types of screening. 13 Our findings revealed racial disparities, with Black women having higher odds and Asian women having lower odds of full participation compared to White women. These differences may reflect variations in cultural beliefs about health and cancer, as well as potential systemic barriers to accessing healthcare.6,32 Culturally tailored interventions that address the specific needs and beliefs of diverse population groups are needed to improve equity in screening participation. 33
Enabling factors, such as income and access to healthcare, also play a critical role. Lower income was a strong predictor of lower concurrent screening participation, highlighting the need to address socioeconomic disparities in access to preventive care.15,17,34 Andersen's model suggests that individuals with lower incomes might face multiple barriers, including differing health beliefs (predisposing factors), limited resources or time constraints (enabling factors), and potentially poorer perceived health status (need factors), all of which can hinder screening participation.20,35 Targeted interventions, such as subsidized transportation or community-based screening programs, could help reduce these disparities. 36
Furthermore, our findings revealed associations between concurrent screening participation and lifestyle factors such as smoking status and physical activity level. This clustering of health behaviors aligns with the notion that individuals who prioritize proactive health choices in one domain might also be more likely to engage in preventive screenings.29,30
Synthesis and implications
Our findings demonstrate the complex and intertwined influences of predisposing, enabling, and need factors on cancer screening behavior. To improve both individual and concurrent screening participation, interventions should address all three components of Andersen's Model. This may involve increasing awareness of cancer risk and promoting positive attitudes towards screening (predisposing factors), improving access to healthcare and addressing financial barriers (enabling factors), and increasing perceived susceptibility to cancer and emphasizing the benefits of early detection (need factors).36–38
The interconnected nature of cancer screening behaviors offers opportunities for integrated public health initiatives. Leveraging participation in one screening program to promote participation in others could be a promising strategy. For example, healthcare providers could use appointments for breast or cervical cancer screening as opportunities to discuss the importance of CRC screening.
While this study highlights the need to increase screening participation, it is important to acknowledge the ethical considerations surrounding screening promotion. Informed choice is a cornerstone of ethical healthcare, and individuals should have the autonomy to make decisions about their health after receiving adequate information about the benefits and risks of screening. Therefore, efforts to promote screening should focus on:
Improving healthcare provider communication: Equipping healthcare providers with the knowledge and skills to engage in clear and comprehensive discussions about screening with their patients, addressing individual needs and concerns. Enhancing patient education: Providing accessible and culturally-sensitive information about screening benefits and risks, empowering individuals to make informed decisions. Addressing barriers to access: Ensuring equitable access to screening services for all individuals, regardless of socioeconomic status, geographic location, or cultural background.
The ultimate goal of screening promotion should be to facilitate informed decision-making and support individuals in making choices that align with their values and preferences. Achieving the participation rate targets for each screening program while respecting individual autonomy requires a multifaceted approach that addresses both individual and systemic barriers.
Strengths and limitations
This study has several strengths. The use of nationally representative data from the CCHS allowed us to examine cancer screening behavior across a diverse range of Canadian women. The large sample size provided sufficient power to detect significant associations. Furthermore, the comprehensive nature of the CCHS dataset allowed us to consider a wide range of sociodemographic, health-related, and healthcare access factors in our analyses.
However, the study also has limitations. As a cross-sectional study, it can only demonstrate associations, not causal relationships. The reliance on self-reported data may be subject to inaccurate recall, possible recall bias, or social desirability bias. While we attempted to exclude women who did not meet the criteria for routine screening, the CCHS dataset may not have captured all relevant clinical information. Additionally, the relatively small sample sizes for certain racial and ethnic groups limit the generalizability of findings for these populations. Finally, the use of complete case analysis, while justified by the low proportion of missing data, may have introduced some bias.
Conclusion
This study reveals a complex interplay of factors influencing cancer screening participation among Canadian women. While most women engage in some form of screening, participation in CRC screening lags behind breast and cervical cancer screening, and concurrent participation in all three programs remains low. These findings underscore the need for a comprehensive approach that addresses individual, social, and systemic barriers to screening. Targeted interventions, culturally tailored strategies, and efforts to improve healthcare access and provider–patient communication are essential to enhance screening uptake and reduce the burden of these cancers among Canadian women. Given the critical role of early detection in improving cancer outcomes, prioritizing increased and equitable screening participation is a crucial public health imperative.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.